“If we attend to the needs of the most vulnerable people, which we won't see unless we purposefully look, everyone has what they need.”
- seen on twitter
A friend passed this to me, saying it might be helpful - it's about getting help on Long Covid from your GP, it's for a UK setting, but some of it will be applicable anywhere - read the note at the end for more too.
"I work in AI. I used it to research and write my mum a letter about her Long COVID. Her GP called her the next day after 3 years of being dismissed!
*Reposting here as myself since it blew up in another support group and people really want help with this… feel free to add/DM me.*
So I work in AI, specifically in healthcare tech. So when my mum had been fobbed off by her GP for the third year in a row about her Long COVID, I figured I should actually do something useful with what I know.
This isn't about gaming the system or bending rules. Everything I'm sharing here is publicly available on NHS and government websites. I just used AI to find it, understand it, and turn it into something a GP couldn't easily brush off.
Here's what most people don't know. The NHS publishes detailed guidelines that GPs are expected to follow. NICE published a specific Long COVID guideline called NG188 that sets out exactly what a GP has to do when a patient comes to them with ongoing post-Covid symptoms. Most patients have never heard of it. Most GPs don't follow it unless someone pushes them on it.
The other thing most people don't know: verbal dismissal is easy to ignore. A formal written letter that references specific guidelines creates a paper trail. The GP now has a documented duty of care they're expected to respond to. It genuinely changes everything.
My mum is 61. Not remotely tech savvy. She would never have found any of this herself. I spent about 20 minutes using AI to pull the relevant guidelines, match them to her situation, and draft a letter. She sent it to her GP by email on a Tuesday. Her GP called her on Wednesday afternoon. First time in three years a GP had called her. She now has a referral to a Long Covid clinic and a written management plan, after years of being told it was probably anxiety or just her age.
Posting her letter below with her details redacted. Copy it, adapt it to your situation, send it by email not in person. You need a timestamp. You need a record. That's what actually forces a response.
───
[Her letter, personal details redacted]
████████████████
████████████████
████████, ██████
██ ██████ 2025
Dr ████████████
████████████ Surgery
████████████████
████████, ██████
Re: Formal written request for Long COVID assessment and personalised management plan
Dear Dr ████████,
I am writing to formally request appropriate assessment and management for post-COVID-19 syndrome (Long COVID), and to create a written record of this request for my medical file.
I contracted COVID-19 in ████████ 2022 and have experienced the following ongoing symptoms for over three years:
• Severe fatigue and post-exertional malaise, symptoms worsen significantly following any physical or cognitive exertion
• Cognitive dysfunction, difficulty with memory, concentration, and word retrieval
• Breathlessness disproportionate to exertion
• Heart palpitations and episodes of tachycardia
• Disrupted sleep despite significant fatigue
• Generalised pain and joint discomfort
These symptoms have substantially impaired my ability to work, maintain daily activities, and quality of life.
CLINICAL BASIS FOR THIS REQUEST
NICE guideline NG188, COVID-19 rapid guideline: managing the long-term effects of COVID-19, was developed jointly by NICE, SIGN and the Royal College of General Practitioners. It applies to any patient with new or ongoing symptoms four or more weeks after acute COVID-19.
Under NG188 section 5.2.1, GPs are expected to use a multidisciplinary approach to guide rehabilitation, including physical, psychological and psychiatric aspects of management.
Under NG188 section 5.2.2, GPs must work with the patient to develop a personalised rehabilitation and management plan, which must be recorded in writing. NICE states explicitly that healthcare professionals are expected to take this guideline fully into account. This is not optional guidance.
Under GMC Good Medical Practice (2024), where a GP cannot adequately manage a patient's condition, they are required to refer to a specialist with the relevant expertise.
Under the NHS Constitution, I have the right to be referred to an appropriate specialist where my GP is unable to provide the required clinical management.
I have not received a personalised management plan or specialist referral in three years of presenting with these symptoms.
WHAT I AM FORMALLY REQUESTING
1. A holistic clinical assessment consistent with NICE NG188, including physical, psychological and functional domains
2. A personalised rehabilitation and management plan recorded in writing, as required under NICE NG188 section 5.2.2
3. Referral to the Long COVID clinic or appropriate multidisciplinary rehabilitation service
4. A written response to this letter within 14 days
I would like this letter to be added to my medical record. I am not requesting anything outside published NHS guidelines. I am asking for what those guidelines state I am entitled to receive.
Yours sincerely,
████████████████
Date of birth: ██/██/████
NHS number: ███ ███ ████
Based on: NICE NG188 (January 2024) | GMC Good Medical Practice (2024) | NHS Constitution (2023)
*Verify current guidelines at https://t.co/1G9ny67PrQ before sending.*
───
Same approach works for basically any condition where you're being dismissed. MCAS (I am currently writing myself a letter to escalate my own issues with this), fibromyalgia, EDS, POTS, chronic fatigue. The escalation pathways exist for all of them, most people just don't know how to use them.
If it’s useful I could build a tool that does this automatically for you. You answer a few questions about your condition, it finds the relevant guidelines and drafts the letter for you. If that sounds useful, DM me or comment. Happy to write one manually for anyone in the meantime.
Not medical advice! Keep seeing your GP. Call 111 if anything gets worse."
L0NG C0VID IS QUIETLY WRECKING HEARTS.
Maybe time for a recap based on 2026 science.
Here’s the comparison for MACE, Stroke, Deadly Clots & overall CV risks:
➡️MACE (heart attack, stroke, heart failure)
• Non-COVID: HR 1.0
• COVID-19: 1.8–3.9x
• Long COVID: ~4.5x
➡️Stroke (ischemic):
• Non-COVID: HR 1.0
• COVID-19: ~2–3x
• Long COVID: ~3.5x
➡️Deadly clots (PE / VTE):
• Non-COVID: HR 1.0
• COVID-19: ~2–4x
• Long COVID: 3.2–4.4x
➡️Overall CV risks:
• Non-COVID: baseline
• COVID-19: ↑1.5–2.5x (arrhythmias, CAD, HF)
• Long COVID: 2–4.5x higher
Long COVID adds extra danger beyond regular post-COVID.
Risks hit even non-hospitalized patients and last for years.
Vax may reduce risks but certainly doesn’t erase it.
Absolute risks lower in young/healthy, but serious if older/comorbid.
‼️Today’s evidence shows that while any COVID-19 infection elevates cardiovascular risks, long COVID dramatically amplifies them, making proactive heart monitoring essential for affected patients.
Bottom line: Get your heart checked post-Covid19/ LongC0vid and #AvoidSars2 #AvoidReinfections!
🚨C0VID-19/L0NG C0VID are serious CV RISK FACTORS!
@HelloCanada Yaas, Stephen and Evie. Keep on walking in your light. You have not been dimmed, and you've still got a kind, authoritative voice that commands attention. Thank-you for the goodness you put out into the world. I can't wait for it to keep coming.
Bruce Springsteen appeared on Stephen Colbert’s show tonight and COOKED Trump and his goons
“I’m here in support tonight for Stephen, because you are the first guy in America who lost his show because we got a president who can't take a joke…. and because Larry and David Ellison feel they need to kiss his ass to get what they want. Stephen, these are small minded people. They got no idea what the freedoms of this beautiful country are supposed to be about”
On September 11, 1974, a ten-year-old boy named Stephen Colbert lost his father and two of his closest brothers, Paul and Peter, when Eastern Air Lines Flight 212 crashed into a cornfield hillside just three miles from the Charlotte, North Carolina airport. Only 13 of the 82 people on board survived. In a single afternoon, the youngest of eleven children in a warm, intellectually curious Catholic household went from a boy surrounded by laughter and big family energy to a kid sitting in a suddenly very quiet, very dark home with only his grieving mother for company. The two leaned on each other in a way that most people never experience. Lorna Colbert held herself together not out of bitterness, but out of a fierce, quiet love, and Stephen watched that and absorbed it into his bones. He later said his mother was never bitter, just broken, and that her example became the blueprint he carried for the rest of his life. For years, though, the real weight of the loss stayed buried. He floated through prep school detached, unbothered by the things other kids cared about, because nothing felt quite real anymore. It wasn't until he went off to Hampden-Sydney College in Virginia that the grief finally cracked through, and it hit him hard. He dropped from 185 pounds down to 135 during his freshman year, barely eating, barely functioning, consumed by a sadness he had held at bay for nearly a decade. But something remarkable happened on the other side of that collapse. He found theater. He found improvisation. He found that making people laugh was actually a way to connect with human suffering rather than run from it. He transferred to Northwestern University, stumbled into the world of Second City, and slowly built himself into one of the most empathetic, genuinely funny voices in American media. He later reflected that losing his father and brothers gave him an awareness of other people's pain that allowed him to love more deeply and connect more honestly with what it means to be human. That is not a small thing. That is everything. Via Chronicles Through Lenses
wowww Paul McCartney just returned to the Ed Sullivan theater as Stephen Colbert's final guest on The Late Show...62 years after his first appearance with the Beatles in 1964. he surprised Stephen with a signed photo from that performance
Stephen: "To Stephen: you're better than the Beatles."
Paul: "No, it doesn't say that!"
Stephen: "When my editors are done, that's what it's gonna say, Paul"
The Late Show ends tonight. After 33 years.
Letterman built it. Colbert inherited it & turned it into something entirely his own.
Across town, Jimmy Fallon & Jimmy Kimmel cleared their schedules.
Both shows going dark tonight. No competition. Just space for the finale.
When your rivals voluntarily cancel themselves so you can have the night to yourself, that's not just common courtesy. That's the industry telling you what it actually thinks of what you built.
Whatever you think of the show, that's not just a send-off. That's a verdict. 🥂
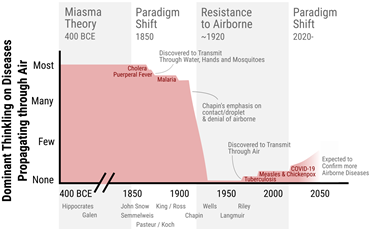
12/ So what about the contribution of history to the denial of and resistance to airborne transmission by Public Health authorities worldwide?
It is summarized in this diagram, which I'll explain in this thread:
https://t.co/2SuvreBOxK
1/ What were the historical reasons for the resistance to recognizing airborne transmission during the COVID-19 pandemic?
Our peer-reviewed open-access paper is now published:
https://t.co/2SuvreBOxK
@ShellyMBoulder@D_Higuera_Ing@el_pais 8/ Lo mas desesperante de la transmision de COVID-19 (y otras enfermedades de transmision por el aire) entre viviendas en Espana:
- Se entiende perfectamente
- Seria facil de prevenir con muy poco coste
- Los gobiernos lo niegan y se niegan a hacer nada al respecto!
@WHO Ebola can aerosol transmit & it is critical there is airborne mitigation- ppe, isolation, tracing protocols, etc.
Many refs in🧵s below.
Final post covers how EVERYTHING we think is droplet/ close contact is actually aerosol (inhaled / thru the air / AIRBORNE)
#ebola
[Kinshasa has already run out of PPE. It looks like Uganda is up next. What a mess.]
🚨
➡️ 🇨🇩 Health workers race to respond to Congo’s fast-spreading Ebola outbreak
- Medical personnel are rushing to the front lines of a new Ebolaoutbreak in eastern Democratic Republic of Congo (DRC) whose late detection and quick spread have alarmed health experts.
- The World Health Organisation (WHO) on Sunday declared the outbreak a public health emergency of international concern because of the high risk the disease could spread further beyond DRC’s borders after two cases were confirmed in Kampala, the capital of neighbouring Uganda.
- The outbreak is suspected to have killed around 80 people in recent weeks, with eight cases confirmed by laboratory testing and 246 suspected cases reported in eastern DRC’s Ituri province.
- ⚠️ Another case was confirmed in neighbouring North Kivu province’s capital, Goma, according to the ⚠️M23 rebels who control the city.
- The US Centers for Disease Control and Prevention also said on Sunday that it was supporting partners withdrawing a small number of directly affected Americans.
- A delegation led by DRC health minister Samuel Roger Kamba arrived in Ituri’s capital Bunia on Sunday with tents to set up treatment centres to support strained local hospitals.
- “This is not a mystical disease,” he said. “Make yourself known so that you can be taken care of and so that we can prevent the disease from spreading.”
- WHO’s representative in DRC, Anne Ancia, said
🚨WHO had emptied its stocks of protective equipment in the capital Kinshasa and ⚠️ was now preparing a cargo plane to bring additional supplies from a depot in Kenya.
- The International Rescue Committee and Medecins Sans Frontieres aid groups said on Monday they had teams responding to the outbreak.
- The current outbreak is caused by the Bundibugyo virus, which unlike the more common Zaire strain of Ebola, has no approved virus-specific therapeutics or vaccine.
- An outbreak from 2018-2020 in North Kivu and Ituri provinces was the second deadliest on record, killing nearly 2,300 people.
- The ⚠️ response to that outbreak was complicated by widespread armed violence in eastern Congo and distrust of first responders by locals. In recent weeks, clashes between rival armed groups in Ituri have killed scores of civilians, worsening an already-dire humanitarian situation.
- Jean Pierre Badombo, the former mayor of Mongbwalu, a mining town in Ituri at the epicentre of the outbreak, said ⚠️ people started falling ill in mid-April after a large open-casket funeral procession arrived from Bunia.
- ⚠️ “After that, we experienced a cascade of deaths,” he said.
- WHO director general Tedros Adhanom Ghebreyesus said on Friday that WHO first learned of suspected cases on May 5th and dispatched a team to Ituri, but samples collected in the field initially tested negative. Subsequent ➡️ tests in Kinshasa confirmed positive cases on May 14th, and WHO declared the outbreak the following day.
- Bangali, IRC’s senior health coordinator in DRC, said ➡️ declining funding from international donors had weakened disease detection.
- “When surveillance networks break down, dangerous diseases like Ebola are able to spread further and faster before communities and health workers can respond,” he said.
- Congo has experienced 17 outbreaks of Ebola since the virus was first identified in the country in 1976. The disease spreads through direct contact with the bodily fluids of infected people or contaminated materials.
- According to WHO, the average fatality rate from Ebola is around 50 per cent, varying from 25-90 per cent in past outbreaks.
- Uganda on Sunday postponed next month’s celebrations of martyrs’ day, a national holiday that typically attracts thousands of pilgrims from eastern DRC, because of the outbreak.
- Haggai Sunday, a doctor at Uganda’s health ministry, told an online briefing that ⚠️ several people from western Uganda who had recently gone to ⚠️ a burial in eastern Congo and then returned home were under observation, with ⚠️ some who developed symptoms taken to the city of Fort Portal
https://t.co/wUjFqBdnmH
Dear @WHO
Pls find a way to get this poor woman some N95s
The handwashing station she operates will generate copious aerosols
That surgical mask won't protect her from inhaling aerosols
😢😢😢
PS - there are thousands more in danger, just like her
Dear @WHO
"people are "really scared" and doing what they can to protect themselves"
"locals are taking precautions such as washing hands with clean water, but added that he wished they could get access to other protective supplies such as face masks"
Send in the N95s
If you dread PPE, you have no business in medicine or public health.
You don’t hear people speak this way about helmets, seatbelts or condoms.
It’s only PPE for airborne viruses that folks take an issue with.
Their unwillingness to promote the right tools will kill people.