Pulmonary embolism: rising incidence, aging patients, more comorbidities. The clinical landscape is shifting: are we keeping up? Read more in #EHJ.
https://t.co/J4qBLHLhUz
#cardiotwitter@ESC_Journals@escardio
Can Earlier LDL-C Lowering Change the Trajectory of Cardiovascular Disease?
https://t.co/eVDmXuZrsT
A thought-provoking simultaneous publication new @ProfKausikRay published in @AJPCardio presented at @society_eas yesterday revisits one of the central questions in prevention:
Are we intervening too late?
Using data from 17 randomized lipid-lowering trials involving more than 105,000 participants, Karungi and colleagues examined how the relative cardiovascular benefit of LDL-C lowering changes across different baseline risk levels.
The findings are intriguing.
1. Contrary to the traditional assumption that lower-risk individuals derive only modest benefit, the investigators observed that relative risk reduction per 1 mmol/L LDL-C lowering was actually greater in lower-risk primary prevention populations.
2. In trial populations with annualized event rates around 1% per year, each mmol/L LDL-C reduction was associated with roughly a 36% relative reduction in events, compared with approximately 13% in populations with event rates near 3% per year.
The paper bring to light an important conceptual framework.
1. As atherosclerosis advances, larger LDL-C reductions may be required to achieve the same proportional benefit.
2. In lower-risk and presumably earlier-stage disease, even modest LDL-C reductions may yield meaningful relative risk reduction.
This shifts the discussion from simply “who is high risk today?” toward a broader life-course perspective:
1. Are we waiting long before intervening?
2. Can modest but earlier LDL-C lowering alter cumulative vascular exposure before disease becomes biologically irreversible?
3. Should early primary prevention become more central to our prevention frameworks?
I think the implications extend beyond statins alone. For the future we need to think around long-duration therapies, , AI-guided risk prediction, imaging-guided prevention, and cumulative LDL exposure increasingly points toward a future where prevention may begin earlier, become more personalized, and focus more on preserving vascular health before advanced disease develops.
@ASPCardio@rblument1
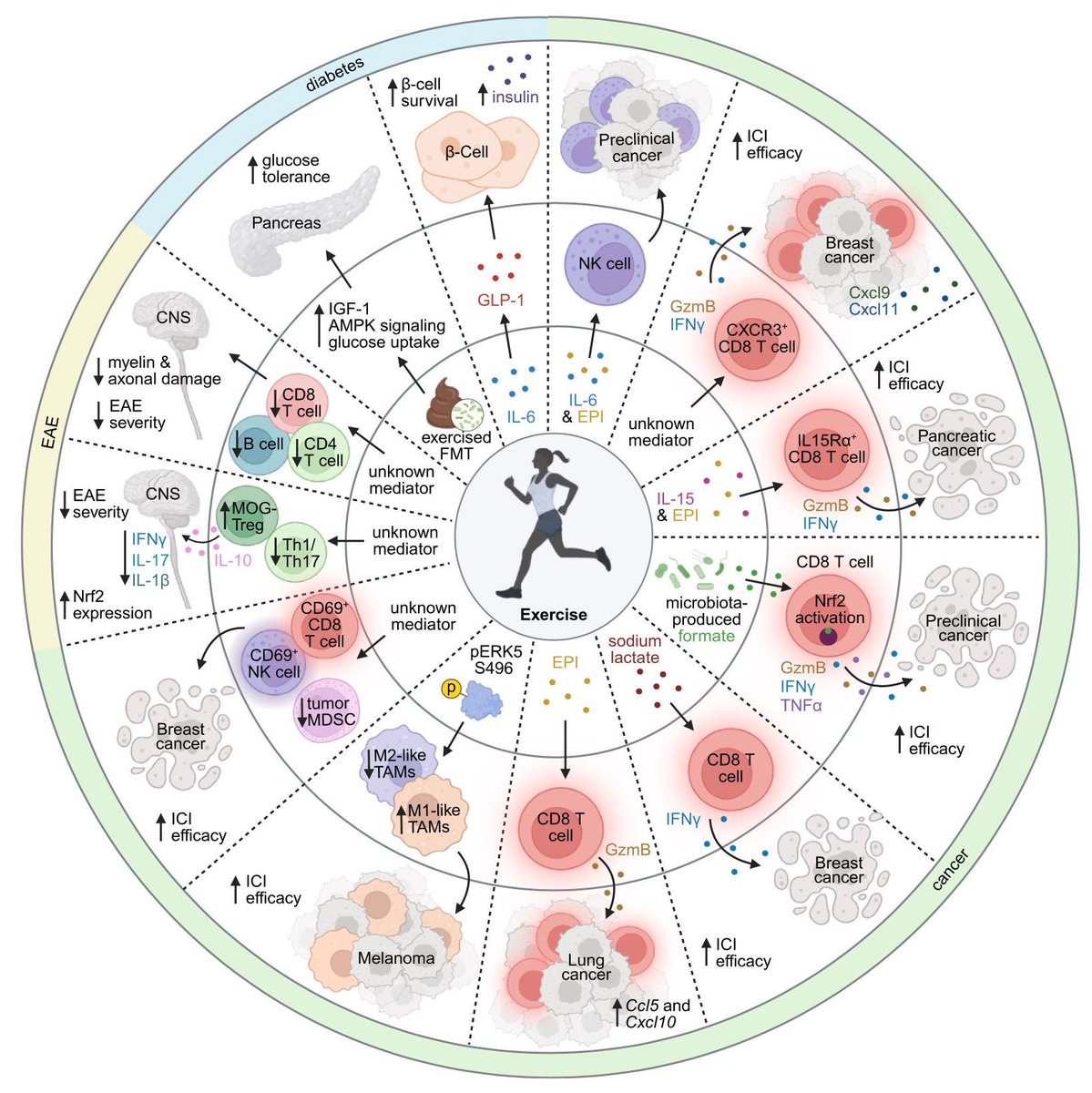
Exercise is not improving your immune system. It is reprogramming it.
Every training session mobilizes immune cells, inflammatory mediators, metabolites, and stress signals that reshape how the body detects threats, repairs tissue, and suppresses disease.
Skeletal muscle functions as an endocrine organ. The biology of performance is immunological before it is physical.
Premature menopause (age <40 years) was associated with a 40% higher lifetime risk of #CoronaryHeartDisease in both Black and White women, supporting its use as a risk-enhancing factor in preventive care. https://t.co/CEoV8jFMU9
This diagram illustrates the multi-targeted, pleiotropic therapeutic effects of Telmisartan across the four primary interconnected components of metabolic syndrome:
🫀 1. HypertensionAs an angiotensin II receptor blocker (ARB), telmisartan binds selectively to the AT1 receptor.
This mechanism prevents blood vessel constriction, directly lowers systemic blood pressure, reduces oxidative stress, and increases beneficial signaling molecules like nitric oxide and prostacyclin to protect endothelial function.
🩸 2.Hyperlipidemia.
Telmisartan helps manage abnormal blood lipids by modulating crucial lipid-metabolic pathways.
It regulates apolipoproteins (such as APO-CIII) and enhances lipoprotein lipase (LPL) and hormone-sensitive lipase (HSL) activity, leading to better breakdown and clearance of circulating triglycerides and low-density lipoproteins (LDL).
🩸 3. Diabetes & Insulin Resistance.
Beyond standard blood pressure management, telmisartan acts as a unique partial agonist of PPAR.
This action stimulates AMPK pathways and boosts adiponectin secretion, which significantly enhances peripheral insulin sensitivity, lowers fasting blood glucose levels, and alleviates pancreatic cell oxidative stress.
⚖️ 4. Obesity.
The medication influences adipose tissue function and distribution, particularly focusing on visceral and perirenal fat depots.
By lowering leptin overproduction and modifying adipocyte differentiation through PPAR and PPAR delta pathways, telmisartan assists in lowering harmful fat accumulation and systemic low-grade inflammation.
https://t.co/MNMXygBs5O
Pressure and Volume Changes in the Cardiac Cycle. Few people know that this is the Wiggers diagram. This classic integrated map of the cardiac cycle aligns, over time, the electrical events of the ECG, valve movements, ventricular and atrial pressures, ventricular volume, and heart sounds. Its value is that it shows the heart not as separate facts, but as a coordinated mechanical sequence.
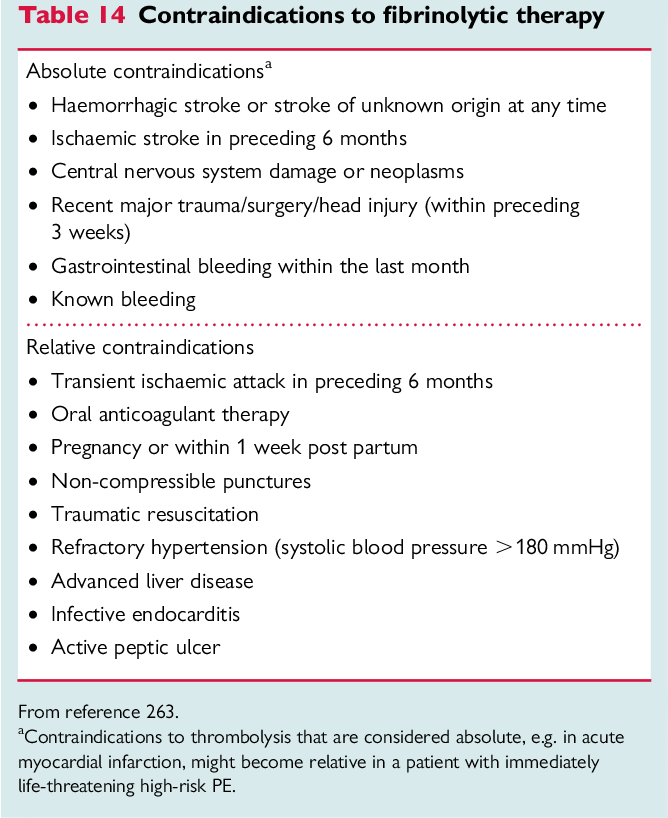
Answer: a) Thrombolysis
This patient with acute MI, grade IV dyspnea, severe HTN (220/120 mmHg) has CXR findings consistent with acute pulmonary edema (bat-wing appearance).
Management considerations:
🔴 Thrombolysis is NOT indicated because SBP >180 mmHg is a contraindication due to increased risk of hemorrhagic stroke.
🟢 Morphine is useful for reducing dyspnea and distress in acute pulmonary edema.
🟢 Aspirin helps reduce clot propagation.
🟢 Furosemide helps relieve cardiogenic pulmonary edema.