50 Years of The Selfish Gene. In my experience, its main message has not sunk in half a century later, even among scientists: one often reads an ingenuous "adaptive explanation" of this or that trait (music, rituals, religion) as "bonding the group," without any awareness that this is not what the theory of natural selection is about or that it is in any way problematic. Dawkins began The Selfish Gene by awakening readers to this fallacy, but it's as if he never wrote it. https://t.co/tobvjYktJ4 via @freethinkermag
Influenced by the book 'Visual Differential Geometry and Forms' , I will recommend to you on this Sunday, the primer 'A Visual Introduction to Curved Geometry for Physicists' by Urbanski, a visual introduction to the basics of differential geometry, publicly available on arXiv.
Few requirements are necessary, other than (very) basic vector calculus and special relativity.
🔗👇
A beautiful example of an "optimal stopping problem" – Feynman's restaurant problem – with a great backstory behind it. This is a fun, well written article, and a fun math problem too.
https://t.co/0Nng9KLDHa
This terrific article by @sioroberts will help elevate the public discussion of AI in mathematics. The interview about the Leiden Declaration is especially helpful. https://t.co/u4SYxQVXZ2
"A tribute to Euler" -- I loved this funny, fascinating lecture by the great William Dunham, one of the world's best math expositors for people who actually like math. https://t.co/ncKOrUZ8Dj via @YouTube
Coffee is one of the only drinks with strong evidence that benefits the liver. Here's what decades of research actually says about how to drink it right:
Coffee genuinely lowers liver disease risk.
Meta-analyses show regular drinkers have about 35% lower risk of significant liver fibrosis and nearly 50% lower risk of liver cancer compared with non-drinkers.
Aim for 2–3 cups a day, minimum.
The effect is dose-dependent. The Hepatology socities such as AASLD and EASL says 3 or more cups daily is reasonable for liver benefit, if you tolerate it.
Caffeinated works better than decaf.
But decaf still helps.
Caffeine blocks adenosine receptors that drive liver scarring. Decaf lowers chronic liver disease risk too, just by a smaller margin (UK Biobank, n=494,585).
The target dose: ~300 mg caffeine/day, or 3 cups.
Fibrosis protection kicks in around the 75th percentile of intake, roughly 308 mg caffeine, or 2.25 cup equivalents, per day - the AASLD 2023 advises 3+ cups for liver benefit.
What a "cup" actually means
One standard cup = 240 ml (8 oz), not a 60 ml tiny Indian "cup." A 240 ml filter coffee has ~95–165 mg caffeine. A single espresso shot (30 ml) has only ~60–75 mg.
Coffee-to-water ratio: 1:15 to 1:17.
For filter/drip/pour-over: 15 g of ground coffee to 250 ml water. This is the standard brewing ratio and gives clean extraction of chlorogenic acids and caffeine.
Choose medium roast, not dark.
Medium roast has significantly higher chlorogenic acid (CGAs) content than dark roast. Dark roasting thermally degrades CGAs, the main antioxidant doing liver work.
Arabica beats Robusta.
Arabica beans are richer in CGAs and polyphenols, the antioxidants doing most of the liver-protective work.
A note here:
Arabica for polyphenols, Robusta for caffeine.
Arabica (1.5% caffeine) has more CGAs and polyphenols. Robusta (2.7% caffeine) has more caffeine but a cruder phenolic profile. A 70:30 Arabica-Robusta blend is a reasonable compromise.
Water temperature: 92–96°C.
Just off a rolling boil. Too hot (>96°C) burns the grounds and extracts bitter compounds; too cool (<90°C) under-extracts CGAs and caffeine.
Grind size matters.
Medium grind (table-salt texture) for filter/drip. Coarse for French press. Fine for espresso. Brew time: 3–4 minutes for pour-over, 4 minutes for French press, 25–30 seconds for espresso.
Filtered coffee is the safest daily choice.
Paper filters trap cafestol and kahweol, naturally present plant diterpenes that raise LDL cholesterol if consumed daily in large amounts. Pour-over (V60, Kalita, Melitta) or drip machines with paper filters give you CGAs and caffeine without the cholesterol penalty.
Espresso and French press: fine, but not unlimited.
They retain more polyphenols but also more diterpenes (so more chances of increased lipids). Great occasionally; don't make them your 5-cups-a-day default if you have high cholesterol or heart disease.
South Indian filter coffee: acceptable, with caveats. The metal filter does not remove diterpenes as well as paper, so limit to 1–2 cups/day if you have dyslipidemia. The decoction itself is rich in CGAs. Use less sugar. Skip condensed milk.
BUT ULTIMATE: Drink it black. Or close to it.
Sugar, syrups, flavored creamers and whipped cream cancel the liver benefit, especially if you already have fatty liver, diabetes, or obesity. Skim milk or unsweetened plant milk is fine.
Instant coffee: still works.
UK Biobank (n=494,585) showed instant coffee drinkers had similar reductions in chronic liver disease as ground coffee drinkers. Not as potent, but far better than no coffee.
Cold brew: underrated for the liver.
Medium roast + coarse grind + 6–7 hours at room temperature extracts CGAs and caffeine efficiently with lower bitterness. pH and CGA content are comparable to hot brew.
Timing.
Spread across the day. one at breakfast, one mid-morning, one early afternoon. Stop by 2 pm if you have insomnia.
It helps across almost every major liver disease.
Evidence supports benefit in fatty liver (MASLD), alcohol-related liver disease, hepatitis B and C, cirrhosis, and liver cancer.
The mechanism isn't magic, it's chemistry.
Chlorogenic acid cuts oxidative stress and liver fat. Caffeine inhibits stellate cell activation (that promotes scarring or fibrosis). Melanoidins and polyphenols reduce inflammation.
Who should go easy.
Pregnancy, children, those with uncontrolled heart rate and rhythmn issues (arrhythmias), panic disorder, or insomnia.
And no, coffee does not undo a bad diet or bad choice - such as alcohol, herbal supplement or that Ayurvedic "liver tonic."
Sources: Modi et al., Hepatology 2010; Kennedy et al., BMC Public Health 2021 (UK Biobank); Fuller & Rao, Sci Rep 2017; AASLD MASLD Clinical Care Pathway 2023; EASL 2016 CPG, Frontiers in Nutrition 2026 (Italian coffee cohort).
Today is World Liver Day 2026.
Here are 8 things your liver actually wants you to know.
1
There is no such thing as a "liver detox."
Your liver runs phase I and II detoxification 24/7 on its own.
No juice cleanse, no milk thistle, no herbal detox speeds this up.
In fact several have caused liver injury - the opposite of the claim.
2
Alcohol has no safe dose.
Liver harm begins from the first drink.
The old "moderate drinking is protective" myth came from flawed studies contaminated by abstainer bias - now debunked by Mendelian randomization.
Zero ml is best.
3
"Natural" supplements are now a leading cause of acute liver failure.
Ashwagandha. Green tea extract. Garcinia. Kratom. High-dose turmeric. Giloy/Tinospora.
They dominate drug-induced liver injury registries across India, the US, and Europe.
Natural ≠ safe.
4
Coffee is genuinely liver-protective.
2–3 cups/day (caffeinated or decaf) lowers the risk of fibrosis, cirrhosis, and liver cancer.
One of the very few dietary interventions with real, replicated evidence.
5
Fatty liver (MASLD) now affects ~1 in 3 adults worldwide.
A 7–10% body-weight loss:
• clears Liver fat
• reduces inflammation
• can regress early fibrosis
No approved drug currently beats this. Your plate and feet are the first-line therapy.
6
Sugar-sweetened drinks independently cause fatty liver.
Fructose is metabolized almost entirely by the liver - straight into fat.
One daily soda raises MASLD risk even after adjusting for total calories.
Lesser is better.
7
Get vaccinated against hepatitis B. Get screened for HBV and HCV at least once in your lifetime.
HBV vaccine prevents >95% of chronic infection, cirrhosis, and liver cancer.
Hepatitis C is curable in 8-12 weeks with >95% success - but most carriers don't know they have it.
8
Exercise protects the liver independent of weight loss.
150 min/week moderate OR 75 min vigorous activity reduces liver fat and stiffness - even when the scale doesn't move.
Movement is "medicine".
🫂
PS: we also need a liver emoji
Murray Gell-Mann on Henry Margenau’s teaching strategy. Margenau was a great teacher and this is a great teaching strategy, although it will probably work only for the brightest students:
“Good teachers are so very rare that it's worth mentioning one. This was Henry Margenau, who died only very recently. He lived to be 97 or something like that. And he was a very good teacher. He taught a course that was called something like Philosophical Foundations of Physics or something of that sort, I forget the exact name, but...*through calling it philosophy he was able to present very advanced material*, which otherwise might not have been considered suitable for sophomores or juniors or whatever.
The way the course went was the following: he would say, ‘Now, we’re going to do… right at the beginning… we're going to do Lagrangian and Hamiltonian mechanics. Now, you all know the calculus of variations, don't you?’ And everybody looked blank. And he said, ‘Well, they haven't taught you the calculus of variations? What do they do in your math classes? They must waste your time with epsilons and deltas. Why don't they teach you the calculus of variations? I can't understand’. Well’, he said, ‘It's not a problem. On Tuesday we will learn the calculus of variations, and on Thursday we will begin Lagrangian and Hamiltonian mechanics, and we'll do it on Thursday, Saturday and the following Tuesday’.
Then he went on to the next subject, which was… well, I don't know, he covered many subjects, but one of them was special relativity which took, I think, two days, and then general relativity. And when he got to general relativity, he asked the same question, he said, ‘You all know tensor analysis, I assume’. We said, no, we don't. He said, ‘Well, what do they do in those math classes? Why don't they teach you tensor analysis instead of all those stupid epsilons and deltas?’ And he said, ‘Well, that’s not a problem. Tuesday and Thursday we'll do tensor analysis and then we'll do general relativity’. And that's exactly the way it worked, and general relativity took only a few days, and he made some wise philosophical remarks about general relativity as well, while teaching us the actual stuff, the actual equations.
And then he went on to quantum mechanics and he did the same thing with quantum mechanics. He said, ‘I assume you know Sturm-Liouville theory?’ We said no. He said, ‘Well, what do they teach you in those math classes?’ Then he said, ‘No problem, we'll do Sturm-Liousville theory, and then we'll do vector spaces and then we'll do quantum mechanics’. And that's what he did, and he showed us wave mechanics and matrix mechanics and how they're equivalent and so on, which was very nice.
So he gave a complete survey basically, of all of the advanced ideas of modern physics.”
https://t.co/Fupoc4kanW
John Preskill points out how, out of Steven Weinberg‘s 50 best known papers, 42 are single author. Weinberg was among a few great physicists like Einstein, Feynman and Dirac who largely did their best work alone.
https://t.co/oOOD3W6EfQ
Someone published a collection of math and science courses, including video lectures, from Stanford, MIT, Berkeley & others in one place, covering:
- Quantum Mechanics, General Relativity, String Theory - Complex Analysis, Algebraic Geometry, Topology
- Astrophysics, Quantum Field Theory, Statistical Mechanics
Overall there are more than 600 courses, many with full video lectures, available for everyone:
Pain on the outside of your hip is one of the most common problems I see in my practice.
Walkers get it. Runners get it. People who've never been to a gym get it.
For decades, we called it bursitis and injected it. We were treating the wrong thing.
I'd watch pretty much any presentation given by the legendary Mikhail ''Misha'' Gromov, bit if I had to choose one, I'd recommend you this gem titled 'What is scalar curvature, really?' which was given at Stony Brooks.
Anyone with an interest in mathematics or physics will want to watch this one carefully. He also gave a longer presentation on the topic, in four parts, at the IHES.
🔗👇👇👇
New video! Memorable for its delightfully absurd name, the Hairy Ball Theorem is extremely beautiful and has some surprising applications.
Full video here: https://t.co/dbfi7yXaOD
If you’re an engineer, physicist, or CS person and you’ve been telling yourself that Pure Mathematics is optional, and you’re anywhere between an ambitious undergrad and a beginning PhD, gravity is usually where that story ends.
Not because mathematicians are trying to show off, but because the basic object in the theory is Spacetime, and Spacetime is already a pure mathematical structure. It’s a Manifold with Topology built in.
Sure you can get pretty far by memorising formulas, but at some point you realise you’re no longer reading the theory, you’re just reciting it.
In 2015, during the 100th anniversary of general relativity and the International Year of Light, the Scientific Organizing Committee released a central set of 24 lectures by Frederic P. Schuller. The series is titled:
A thorough introduction to the theory of general relativity.
It builds the subject carefully from first principles, step by step, across 24 self-contained lectures.
#GeneralRelativity #Spacetime #MathematicalPhysics #DifferentialGeometry #PhysicsEducation #Relativity
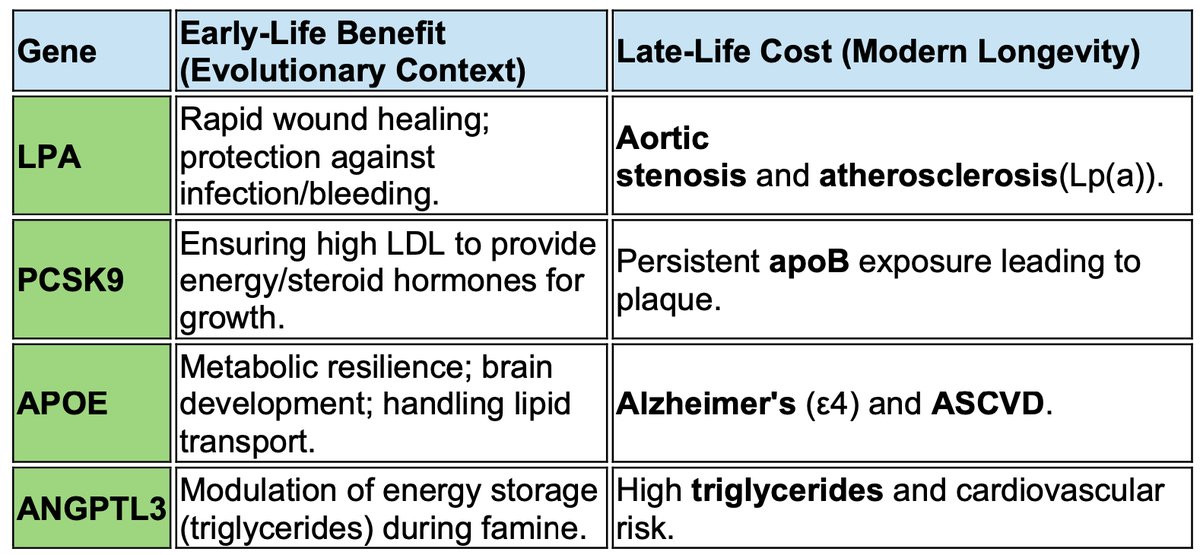
🧬 Antagonistic Pleiotropy
📍 Cholesterol genes were never meant to keep us alive at 80.
They were selected to get us to reproduction.
📍 Evolution did not optimize human biology for cardiovascular longevity.
It optimized it for early survival, fertility, and metabolic resilience.
Genes such as APOE, LPA, PCSK9, and ANGPTL3 exemplify antagonistic pleiotropy:
👉 Early-life advantage (energy handling, immunity, tissue repair)
👉 Late-life cost (atherosclerosis, ASCVD, valvular disease)
📍 High LDL-C and elevated Lp(a) are not physiological defaults.
They are evolutionary trade-offs, tolerated because their toxicity manifests after reproductive age.
What modern preventive cardiology does is unprecedented in evolutionary terms:
👉 we intervene upstream, against genes that natural selection had no incentive to fix.
📍 This is where gene-editing therapies change the paradigm.
CRISPR-based and other gene-editing approaches targeting:
1️⃣ PCSK9
2️⃣ ANGPTL3
3️⃣ LPA
do not merely lower cholesterol. They rewrite evolutionary compromises.
For the first time, medicine is not compensating for biology —
it is correcting it at its genetic root.
The real question is no longer whether lifelong exposure to apoB is causal.
🤔 The question is:
How far are we willing to go in editing genes that evolution deliberately left imperfect?
1️⃣ Cardiovascular disease is not a failure of medicine.
2️⃣ It is the price of evolutionary success — and of unprecedented human longevity.
3️⃣ Gene editing may finally allow us to stop paying that price.
@society_eas@nationallipid@skathire@amitvkhera@JohnKastelein@Drlipid@EricTopol@PeterAttiaMD
There's been a ton of discussion about the recent @BMJMedicine paper on exercise variety and longevity. I have some thoughts, including on why statistically adjusting for BMI, blood pressure, cholesterol, etc. creates the illusion of a plateau:
https://t.co/SjPsUDE17P