🆕🆕Atrial Cardiomyopathy Revisited - Evolution of a Concept
A Clinical Consensus Statement of the EHRA HRS APHRS and LAHRS
#LAHRSconsensus#EUROPACE
https://t.co/hOx8iGLhJJ
RBBP (right bundle branch pacing) is here! The picture of conduction system pacing gets more complete. Heart Rhythm: Right bundle branch pacing: criteria, characteristics and outcomes. DOI: 10.1016/j.hrthm.2023.01.017 #dontdisthehis#EPeeps@curilakarol@drpmoskal@Hisdoc1
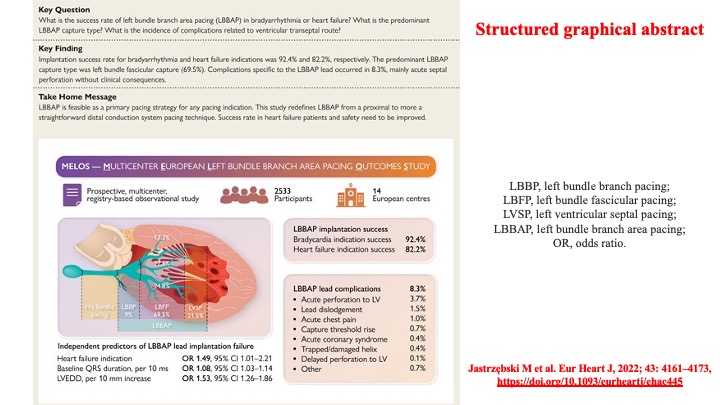
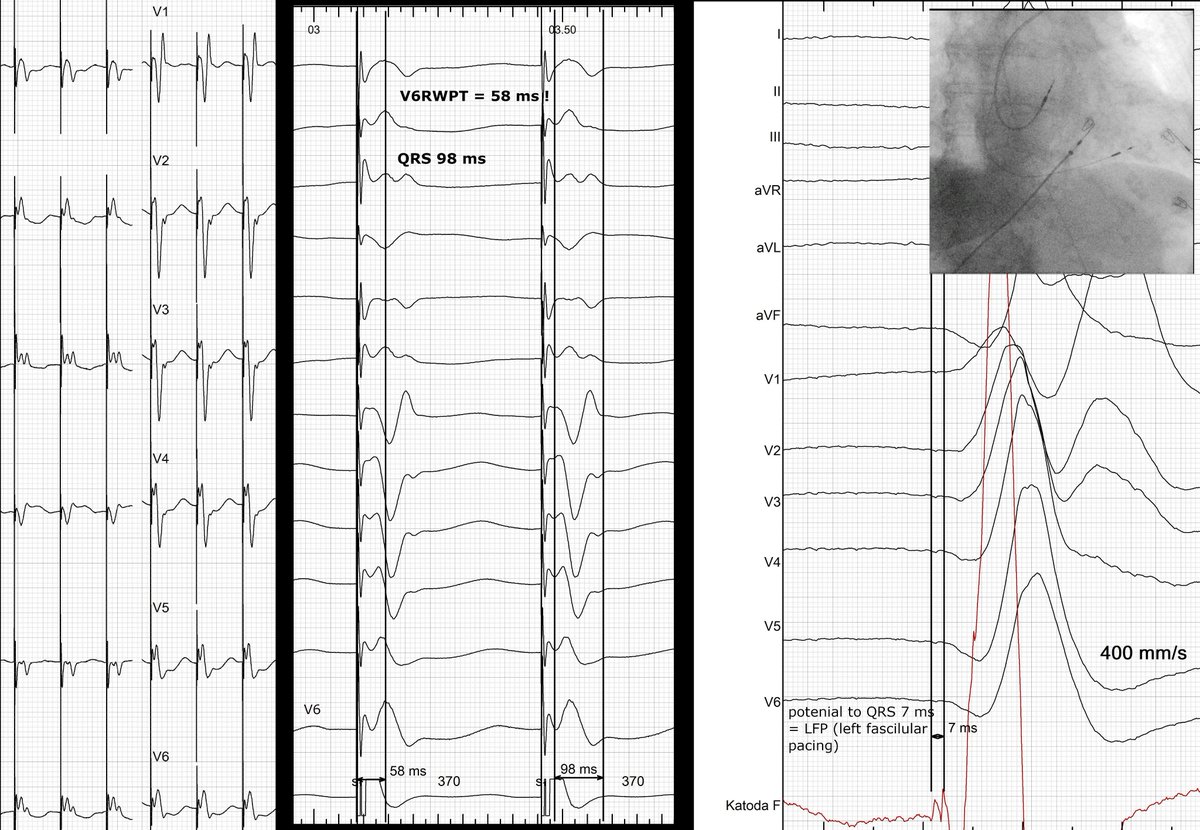
LFP - left fascicular pacing = wide pacing target on midseptum; just 7 ms potential to QRS = less latency = narrower QRS, shorter V6 RWPT (R-peak time). Predominat LBBAP modality in Europe per MELOS results. #dontdisthehis#EPeeps@curilakarol@drpmoskal@shunmug_his_mdu@Hisdoc1
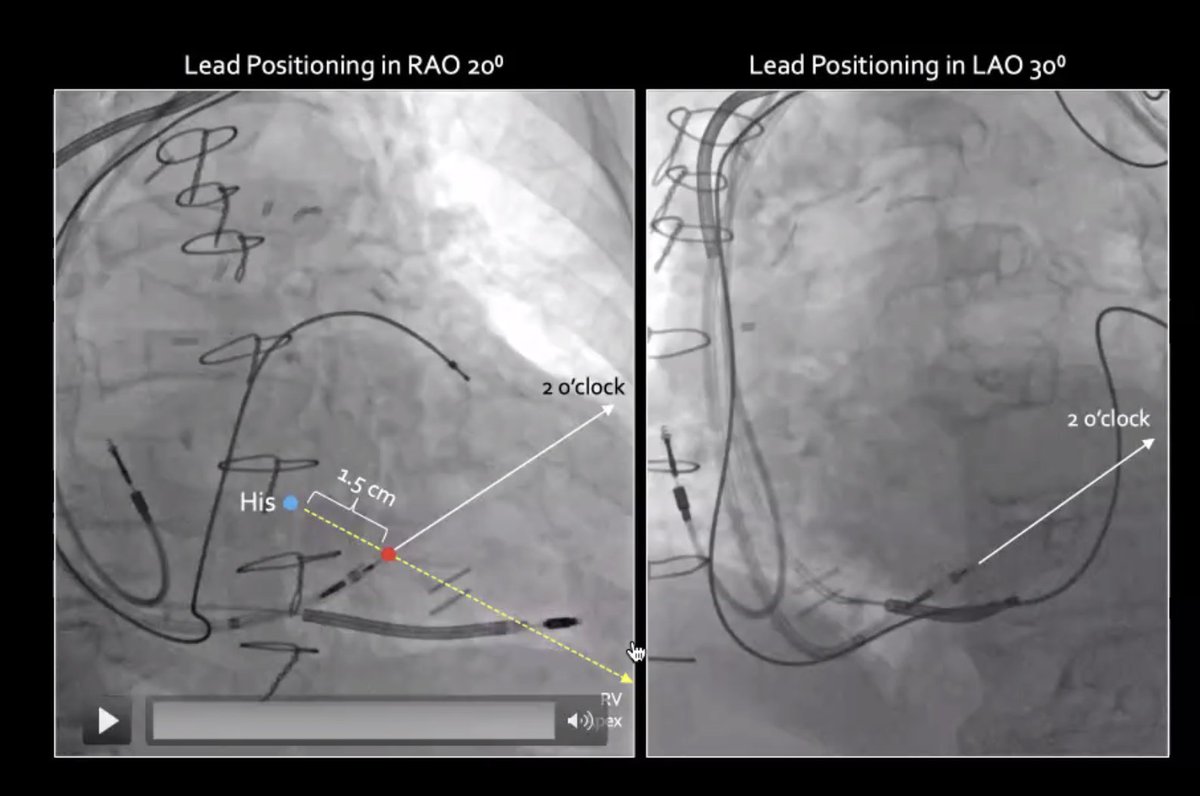
Pearls on LBBA pacing fr @rdschaller on @MDT_Cardiac
webinar
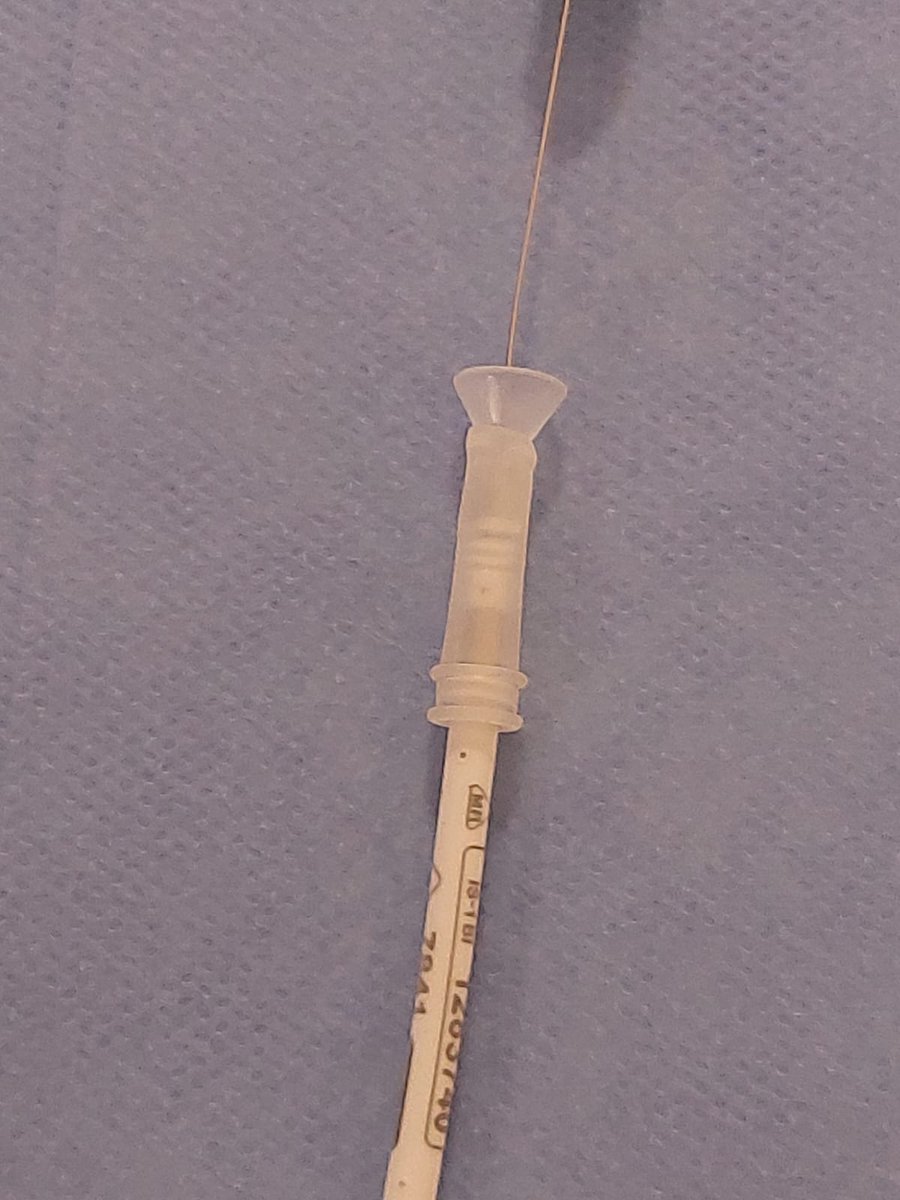
✳️ Point sheath 2 o'clock in RAO/LAO
✳️ Use 1 pair of gloves during lead spin
✳️ If lead goes off axis or torque builds, remove & start over
✳️ Don't confuse anodal capture with non-selective
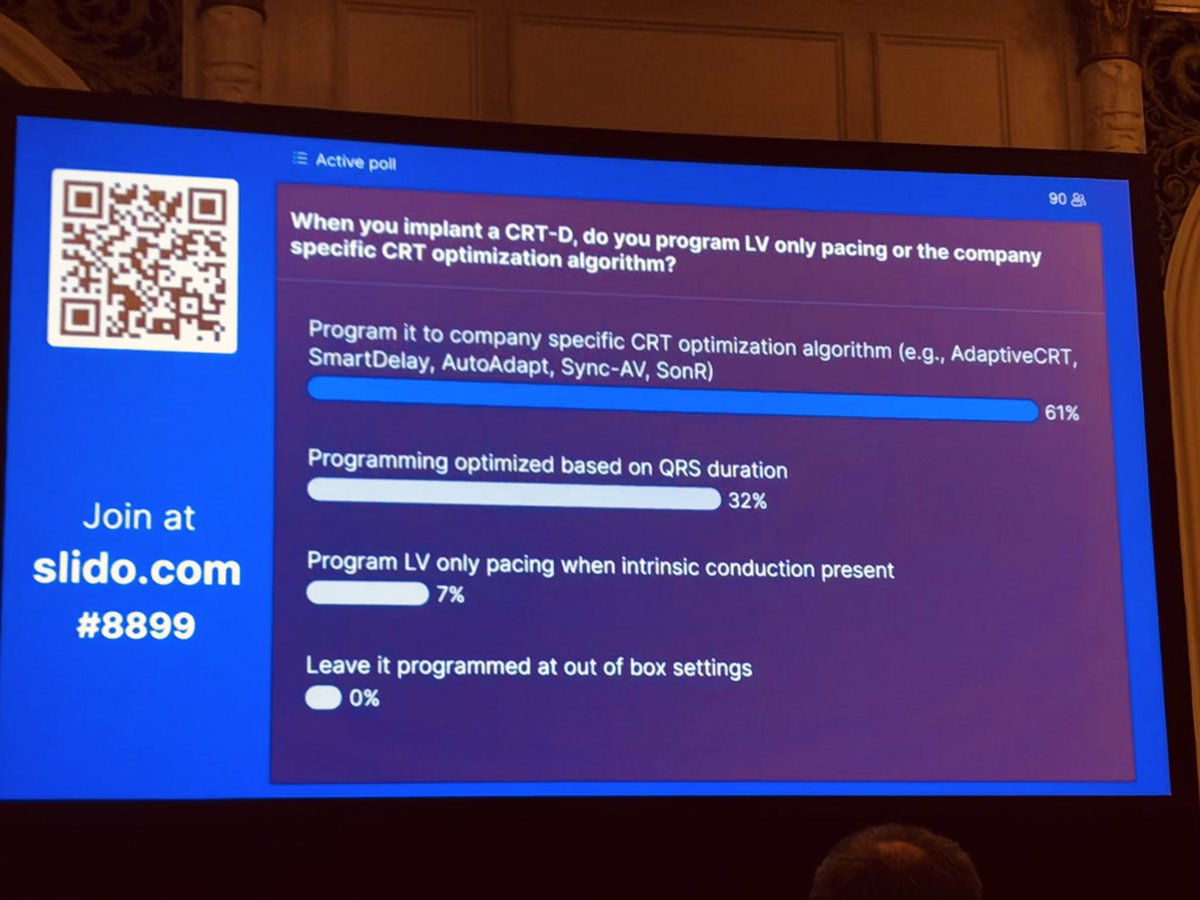
- Conduction system pacing: looking for a narrow QRS #EPeeps
- BiVP: only 32% looking for the best QRS… (BEST Trial by Trucco et al JACCEP… FOI method evidence)
Why?
Could we compare CSP vs BIVP -without QRS optimization? #PPS6
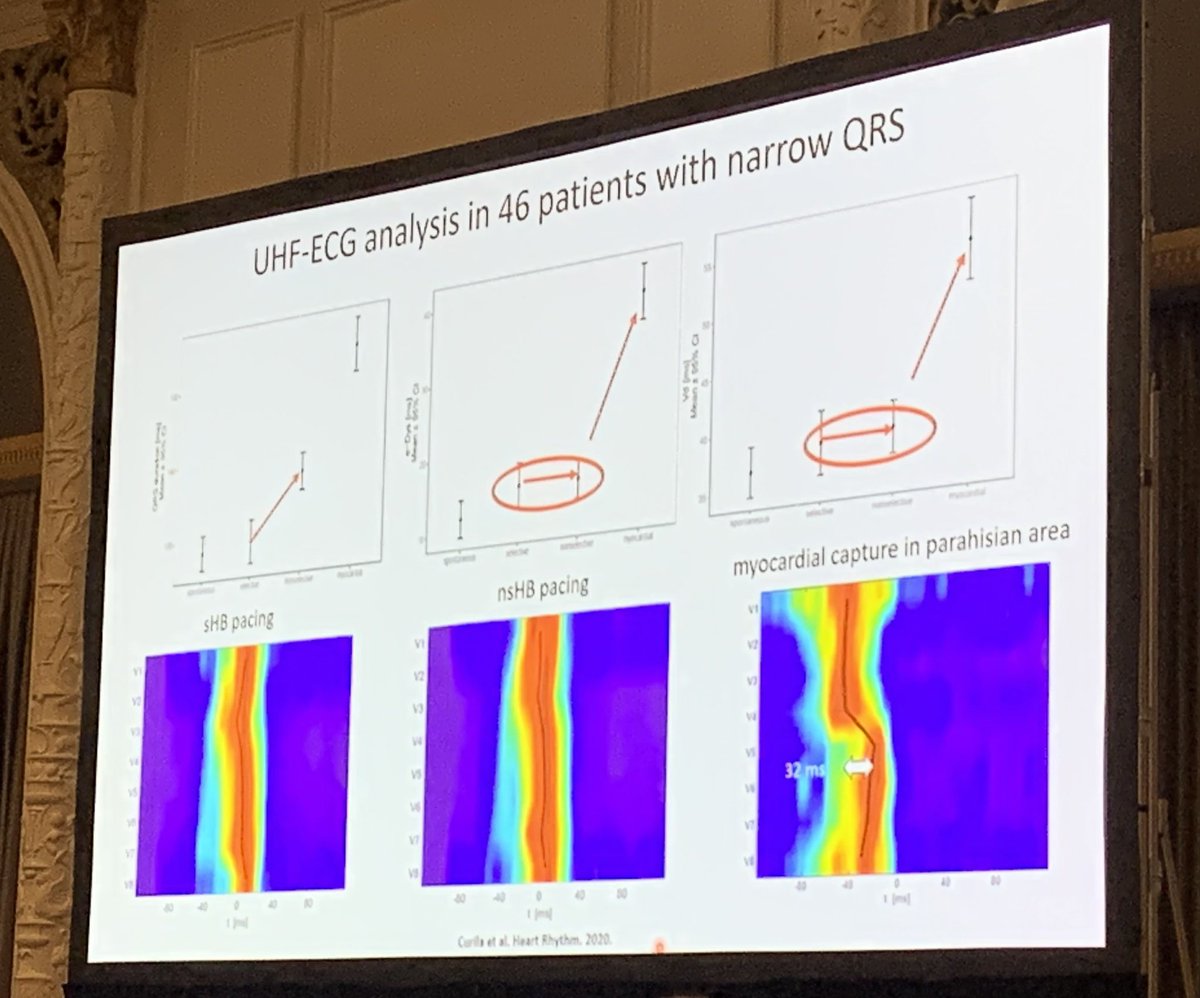
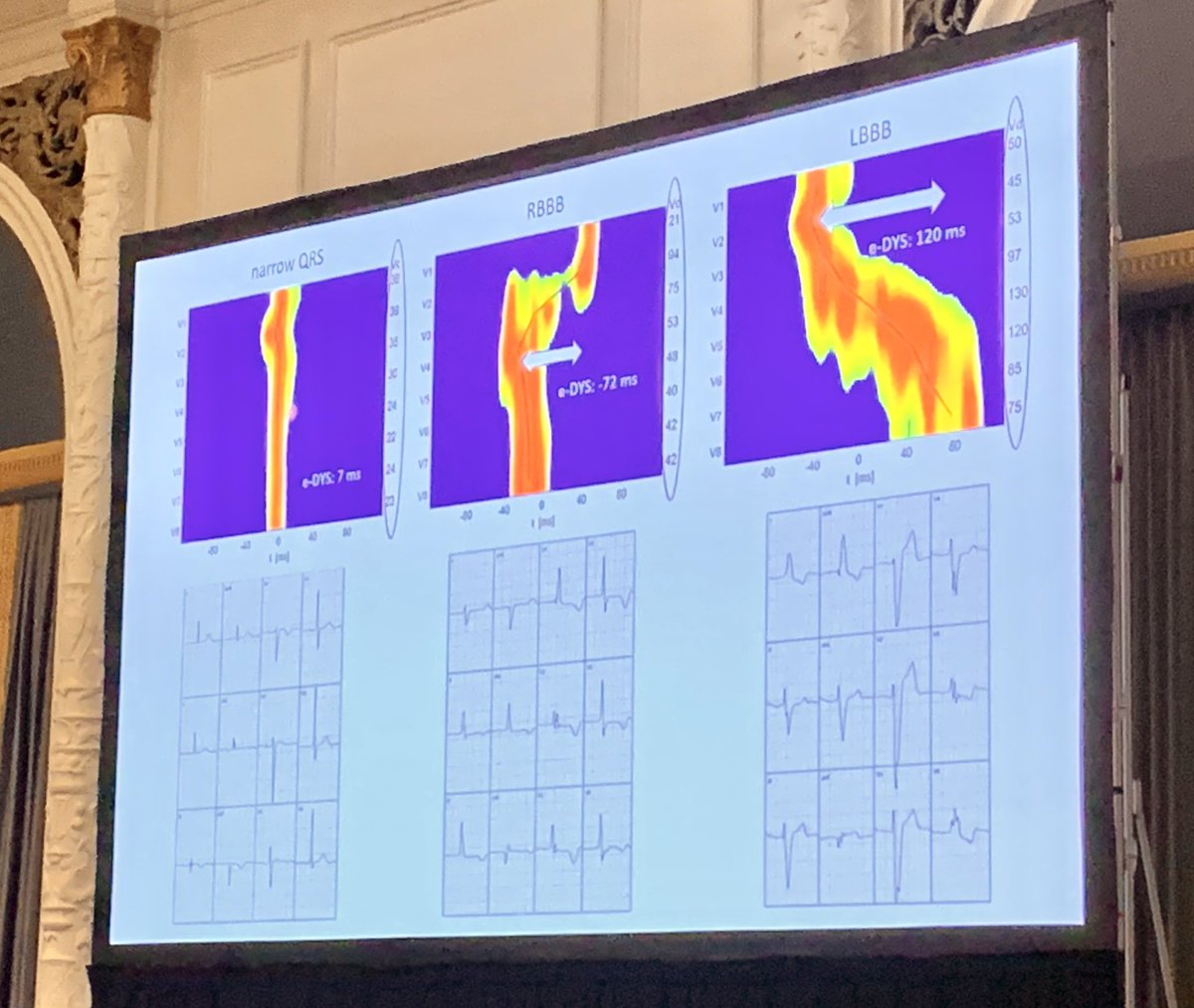
Nice study from @curilakarol using Ultra-High Frequency ECG to better understand activation & electrical synchrony / dyssychrony
Here is the paper in @hrs_journal:
https://t.co/0ABK0e8oMu
#PPS6@kvernooy
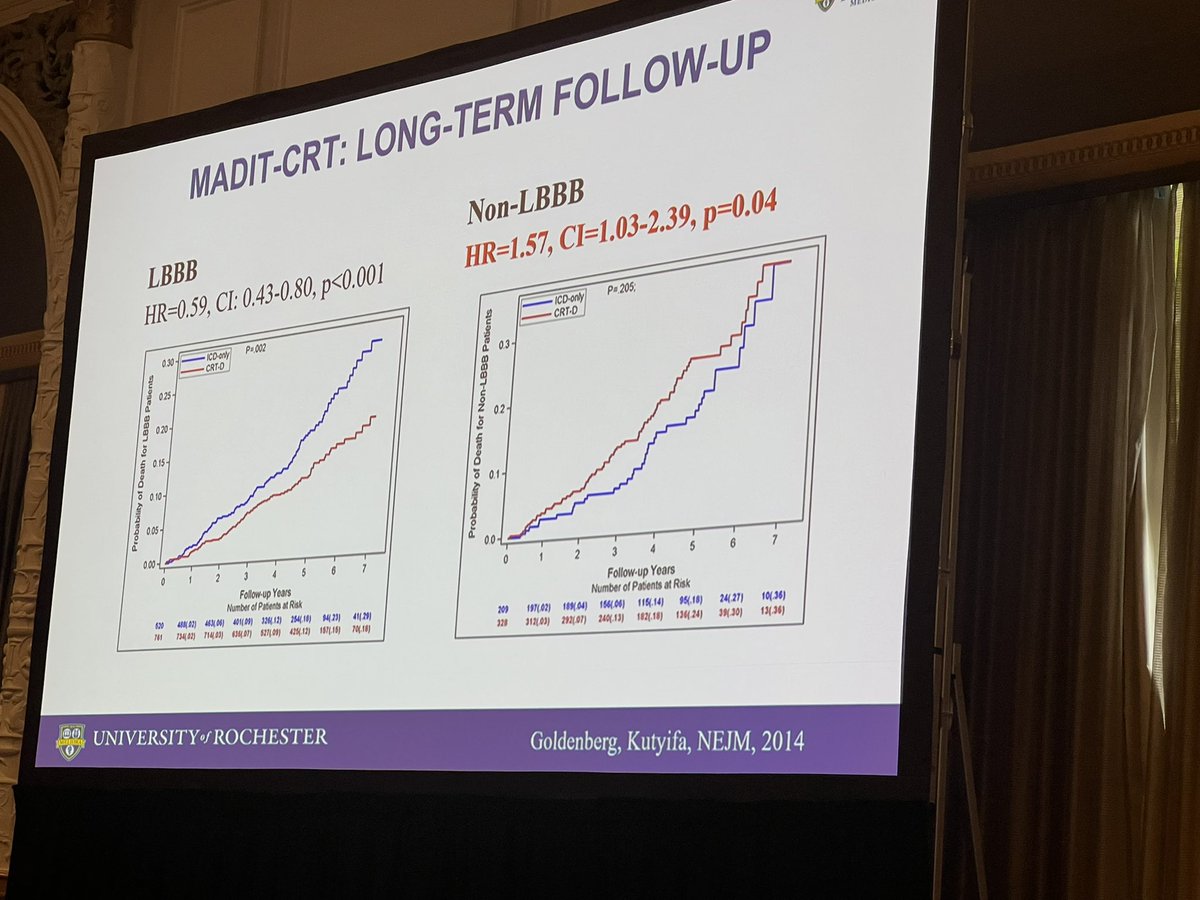
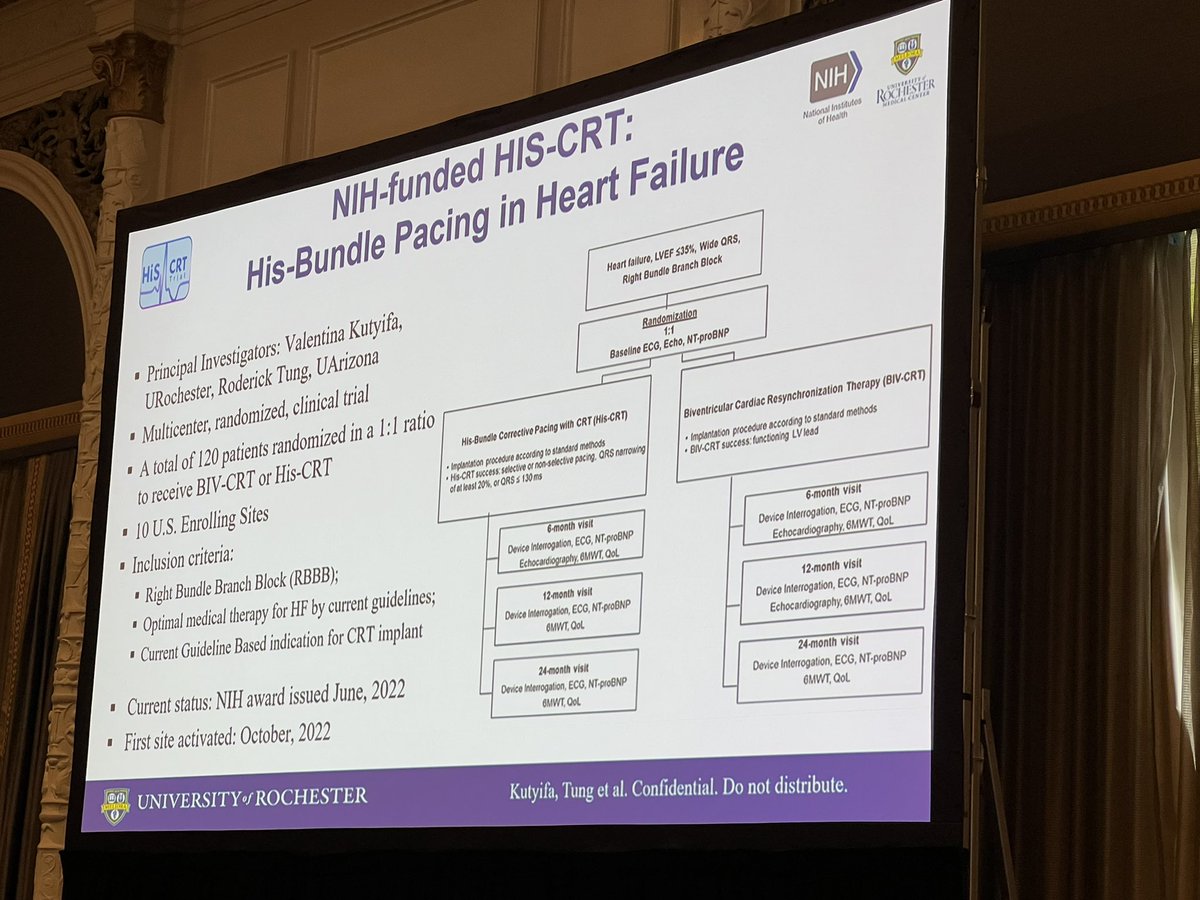
Great summary @VKutyifa with clear rationale for His bundle pacing in RBBB as there is clear potential to do harm with CRT in nonLBBB. @nih_nhlbi #PPS6
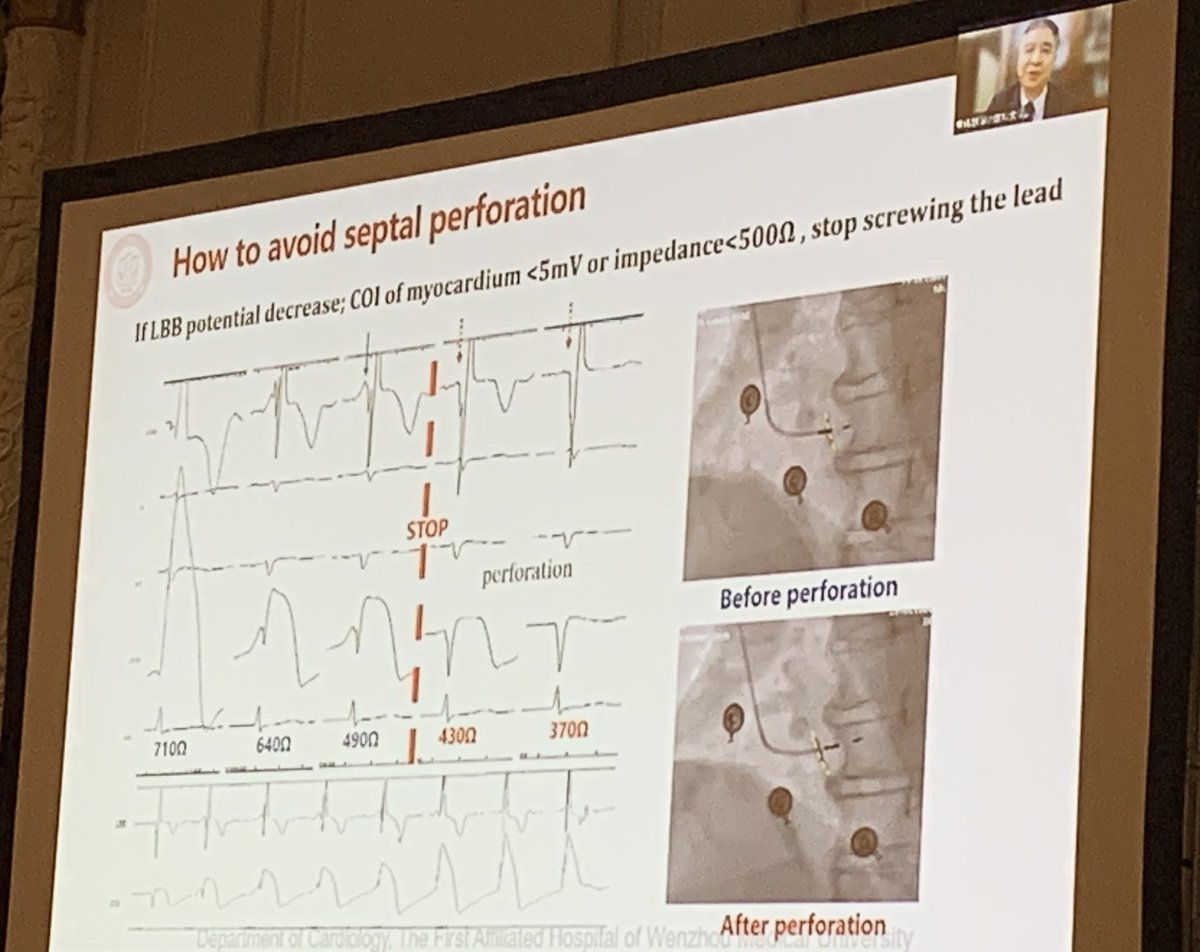
Very practical pearls to know when to continue vs stop screwing in lead when doing #LBBBAP from @MdHuang
Importantly STOP when:
* LBB potential not growing
* + LBB COI
* typical RBBB fusion beats
* COI <3mV
* Impedance ⬇️ <500 Ohms
#PPS6
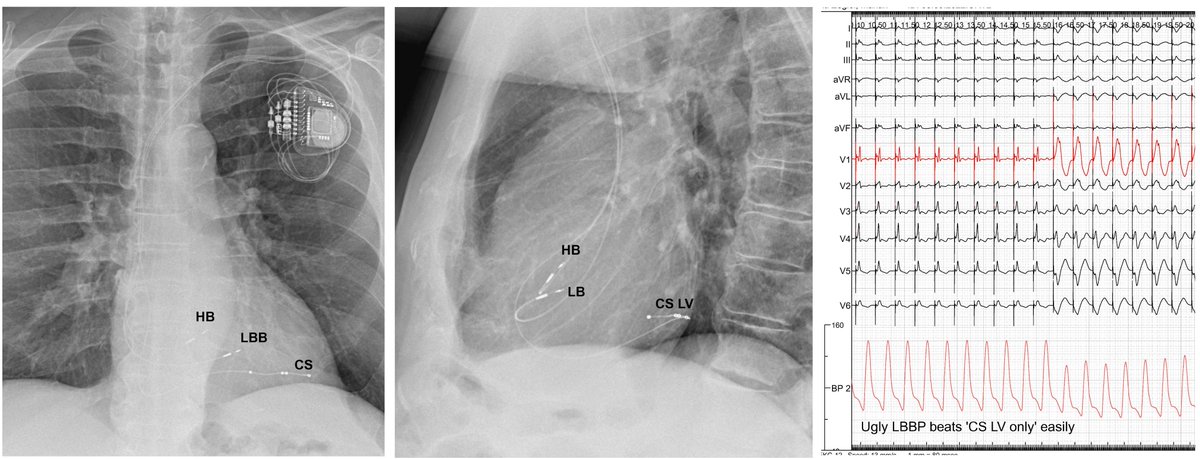
Three 'physiological' leads - which one is the worst? Where did the myth "CS LV only is as good as BiV" came from? Epicardial lateral LV pacing seems the worst imaginable pacing site, terrible intraLV & RV-LV asychrony. #dontdisthehis@curilakarol@drpmoskal@Hisdoc1@OCanoPerez
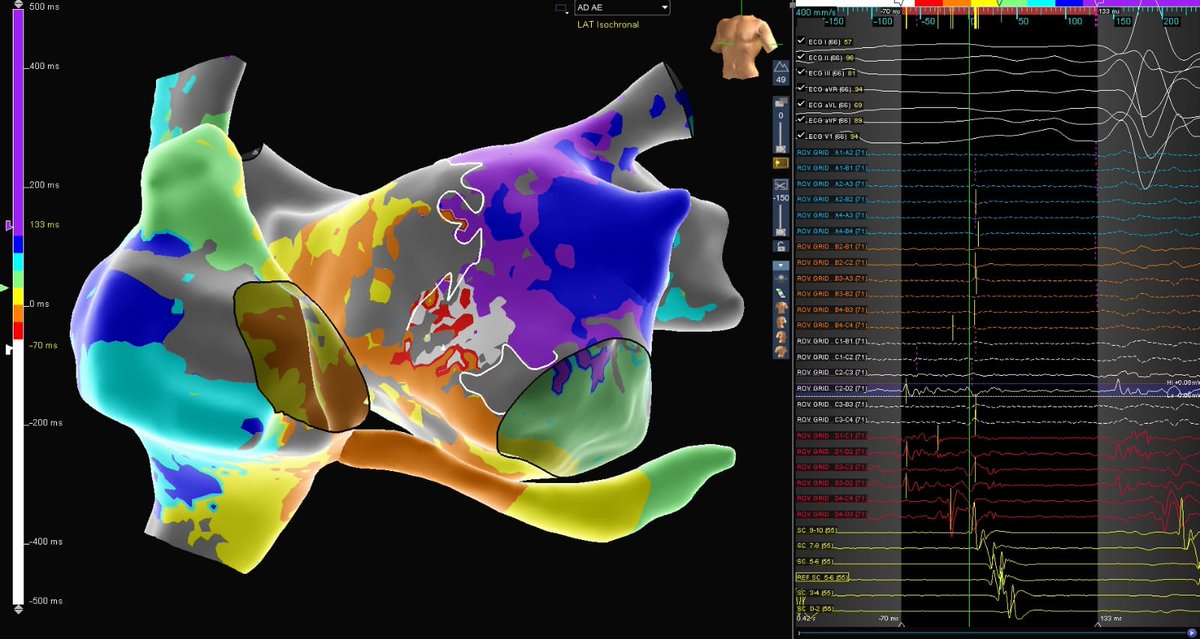
PACEMAPPING for LBBP: lead II, III discord & V1 notch, OK. But what about narrow QRS as criterion to screw the lead? Here exceptional QRS 78 ms V6RWPT on RV septum during pacemapping. Just 3 lead turns to LBB capture.
#dontdisthehis@curilakarol@drpmoskal@Hisdoc1@OCanoPerez
@Marek_Jastrz_EP@curilakarol@drpmoskal@Hisdoc1@OCanoPerez I found a similar situation: Paced QRS in RV septum was identical to LBB capture (narrow, qR in V1 and LVAT < 85). 3-4 turns and we got LBB capture. I would like to see a UHF-EKG in this position before screwing.
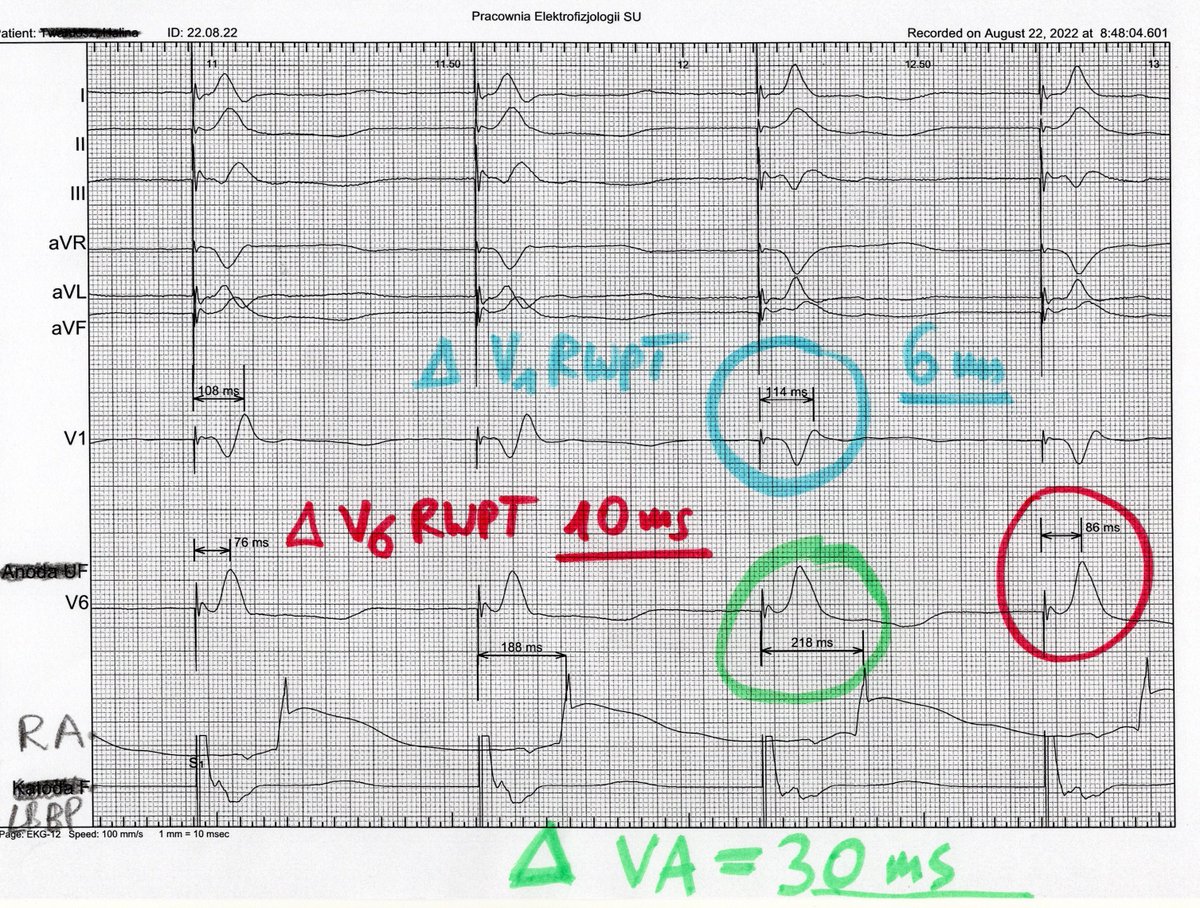
QRS transition @ threshold test for LBB capture diag deserves precise criteria. Here delta V6RWPT > delta V1RWPT + decrease R V1 amplitude argues for transition nsLBBP to LVSP. But delta VA interval is the lifesaver. #dontdisthehis@curilakarol@drpmoskal@Hisdoc1@OCanoPerez