If you've been experiencing severe neck/back pain especially for a long time (chronic). I recommend looking into physical therapy.
Trust me, it's a life changer to such lifetime pain
If you’re experiencing severe neck/back pain, I recommend looking into a disc replacement.
If you do, err on the side of a disc with limited movement. A simple hinge is more likely to be effective than a high mobility artificial disc that can translate, as well as rotate.
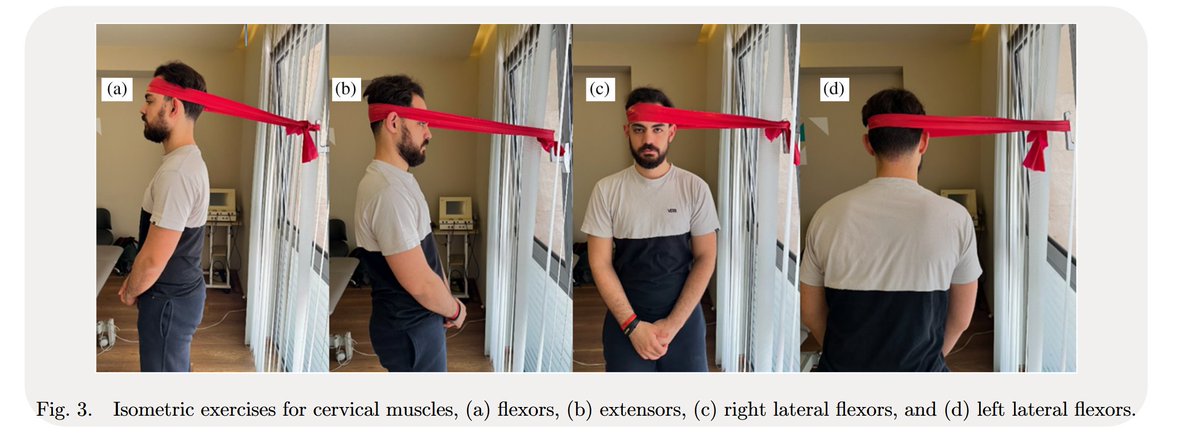
Comparison of the short-term effects of Mulligan and Maitland mobilisation techniques combined with home-based exercise for non-specific neck pain: A RCT
https://t.co/atHhk0XH8T
TOP REMINDERS
PNEUMONIA IS NOT CAUSED BY COLD
HUNGER IS NOT THE MAIN CAUSE OF STOMACH ULCER
YOU CAN HAVE HYPERTENSION AS A YOUNG PERSON
AMPICLOX BEECHAM DOES NOT REMOVE PREGNANCY
PEOPLE WITH PCOS AND FIBROIDS CAN STILL GIVE BIRTH
75 Must-Know Medical Terms, Abbreviations and Acronyms
Medical terms
1. Abrasion: A cut or scrape that typically isn’t serious.
2. Abscess: A tender, fluid-filled pocket that forms in tissue, usually due to infection.
3. Acute: Signifies a condition that begins abruptly and is sometimes severe, but the duration is short.
4. Benign: Not cancerous.
5. Biopsy: A small sample of tissue that’s taken for testing.
6. Chronic: Signifies a recurring, persistent condition like heart disease.
7. Contusion: A bruise.
8. Defibrillator: A medical device that uses electric shocks to restore normal heartbeat.
9. Edema: Swelling caused by fluid accumulation.
10. Embolism: An arterial blockage, often caused by a blood clot.
11. Epidermis: The outer layer of the skin.
12. Fracture: Broken bone or cartilage.
13. Gland: An organ or tissue that produces and secretes fluids that serve a specific function.
14. Hypertension: High blood pressure.
15. Inpatient: A patient who requires hospitalization.
16. Intravenous: Indicates medication or fluid that’s delivered by vein.
17. Malignant: Indicates the presence of cancerous cells.
18. Outpatient: A patient who receives care without being admitted to a hospital.
19. Prognosis: The predicated outcome of disease progression and treatment.
20. Relapse: Return of disease or symptoms after a patient has recovered.
21. Sutures: Stitches, which are used to join tissues together as they heal.
22. Transplant: The removal of an organ or tissue from one body that is implanted into another.
23. Vaccine: A substance that stimulates antibody production to provide immunity against disease.
24. Zoonotic disease: A disease that is transmissible from animals to humans. 1/n
When you can't remember NSAID side effects but then you realize it's in the name...
N - Nephrotoxicity
S - Stomach ulcers
A - Anti-prostaglandin
I - Increased bleeding
D - Decreased renal perfusion
One mistake can cost your son his fertility
• If your son ever has sudden testicular pain, go straight to A&E. Do not wait
There is a 4–6 hour window to save the testicle
• Teach him early to report testicular pain, swelling, or lumps immediately
Delay is one of the biggest causes of permanent damage
• Do not skip routine childhood vaccines.
• If he develops jaw swelling with fever, get him checked urgently. This could be mumps
• After any groin injury, monitor for swelling or ongoing pain. If it persists, get medical help
• Keep baths warm, not hot. If it feels too hot for your wrist, it’s too hot for their testicles
• Use groin protection during sports
A direct hit can cause permanent damage
• If one or both testicles never come down, get it treated early
After a heart attack or heart failure diagnosis, the heart muscle itself can show remarkable plasticity. Guided, progressive exercise prescribed by physiotherapists can improve left ventricular ejection fraction by 10–25 % in many patients, sometimes matching or exceeding what certain medications achieve alone.
The old “rest completely” advice is outdated. Early supervised mobilisation + breathing techniques + strength training literally helps the heart remodel and pump more efficiently. The body is far more resilient than we once thought! 💪🫀
I am a licensed, professional, guideline-oriented, knowledgeable, and experienced physiotherapy based in Lagos.
Kindly reach out if you need the service of a physiotherapist. I also run online consultation. 🙌🏽
This story stopped me in my tracks.
Michael DeBakey invented the classification system for aortic dissection.
He pioneered the surgery to repair it and trained hundreds of surgeons to perform it.
At 97, when it happened to him, he refused the operation.
He knew what the recovery would do to his body as he had seen it destroy patients.
He signed a DNR and went home to die on his own terms, but the condition worsened.
His wife overruled him.
The ethics committee approved surgery after a long back and forth.
The anaesthesia team refused to participate as he had been clear about his wishes, so another team was brought in.
His own students operated on him using the grafts he invented, followed techniques he'd taught them, and they saved him anyway.
He lived two more years.
Went back to work, lectured, trained, delivered speeches, and received the Congressional Gold Medal.
The man who taught the world to fight for every heartbeat had to be convinced at the end that his own was still worth fighting for.
Sometimes, the hardest patient to save is yourself.
(Credit: Lovely USA)
As a physician, I want to explain why we intubate patients.
Endotracheal intubation consists of placing a tube through the mouth into the trachea to ensure that air reaches the lungs adequately. It is not done routinely or “preventively”; it is performed when a patient’s life depends on maintaining a secure airway and effective breathing.
Why is intubation necessary?
We intubate when a person cannot breathe on their own, cannot protect their airway, or when oxygen exchange is insufficient. The most common situations include:
Severe respiratory failure (severe pneumonia, acute respiratory distress syndrome).
Altered level of consciousness (trauma, neurological events, intoxications).
Major surgeries requiring general anesthesia.
Cardiac arrest or imminent risk of aspiration.
What is achieved with intubation?
Keeping the airway open and protected.
Allowing connection to a mechanical ventilator to control breathing.
Ensuring that oxygen reaches the lungs and, from there, the rest of the body through the bloodstream.
Preventing secretions or gastric contents from entering the lungs.
What you should know
Intubation is not a punishment nor a delayed decision. It is a critical medical measure to gain time, stabilize the patient, and treat the underlying cause that put their breathing at risk. It is always performed after weighing risks and benefits, and by trained personnel.
Although visually striking, this procedure is one of the most important tools in modern medicine to save lives when the body cannot do so on its own.
---
Essential reminder: The information presented is for academic and educational purposes only. It does not constitute medical advice and should not be used for self-treatment. If you have symptoms or concerns, consult your trusted physician.
#Medtwitter #FOAMed @dr_manish_ydv@Dr_Shiv_kumar_ @DrAkhilX @DrArslan480@DrArslan480@IhabFathiSulima
"The most useless thing in University Education is Project"
The frustration is quite understandable. Many Nigerian students can relate to the stress of formatting rules, repeated corrections, printing multiple copies, and sometimes difficult supervisory relationships. However, it is important to respectfully disagree with the idea that a research project is “the most useless thing” in university education.
Research projects in Nigerian universities are not designed to frustrate students; they are meant to build capacity. The compulsory research project serves as a foundational training ground. It teaches students how to think critically, identify problems, review existing literature, analyze data, and communicate findings in a structured way. These are lifelong skills that extend far beyond the classroom.
Most individuals who have made significant contributions in academia, science, healthcare, engineering, and technology were shaped by the foundational research exposure they received during their undergraduate years. That early experience, however stressful, often ignites curiosity, discipline, and independent thinking. For those who eventually pursue postgraduate studies or research-focused careers, the undergraduate project becomes the bedrock upon which advanced research skills are built.
It is true that many Nigerian students dislike research, and for valid reasons; heavy academic workload, poor funding, lack of research infrastructure, strained relationships with supervisors, financial burden of printing, and data collection. These systemic challenges can make the process discouraging. However, the existence of these problems does not invalidate the purpose or value of research training itself. Rather, it highlights areas that need reform and better institutional support.
Regarding the discarded hard copies, it raises an important question about value perception. If students truly appreciate the work they did, many would consider refining and publishing it, working collaboratively with their supervisors. While authorship dynamics can sometimes be contentious, the broader goal remains contributing to the body of knowledge. Once published, that research could be accessed by someone in Jamaica, Australia, the USA, China, or elsewhere. Another researcher may build upon it, refine it, or apply it to solve a real-world problem. That is how global knowledge grows, incrementally.
Nigeria indeed struggles with inadequate research funding. Many students and researchers finance projects from personal resources, and this has contributed to slow scientific and technological advancement. Underfunding is a serious structural problem that deserves attention. But abandoning research is not the solution. Improving funding, mentorship, infrastructure, and research culture is.
Finally, the undergraduate research project is not useless. It is imperfectly implemented in many cases, yes, but it remains a powerful academic foundation. When properly supported and valued, it can shape innovators, scholars, and problem-solvers who contribute meaningfully to national and global development.
International Day of Women and Girls in Science.
The Alphabet of Women in Science
Yesterday in class, we were asked to share our career role models. I chose Thomas Edison.
A classmate laughed. “I bet you chose a male scientist because there are no female scientists.”
“There are,” I replied. “Marie Curie was—”
“She’s probably the only one,” he interrupted.
I took a deep breath. “If I can list 25 women in science and their contributions, you concede. If I can’t, I will.”
Our teacher smiled. “Deal.”
The next morning, I stood before the class.
“Good morning. Today, I honor women who have shaped science across centuries and continents. This list is not exhaustive.”
I began.
A – Annie Easley
Computer scientist and mathematician at NASA who worked on energy conversion systems and the Centaur rocket program.
B – Barbara McClintock
Geneticist who discovered transposable elements (“jumping genes”) and won the Nobel Prize.
C – Caroline Herschel
Astronomer who discovered several comets and contributed to star cataloguing.
D – Dora Akunyili
Pharmacist and former Director-General of NAFDAC who fought counterfeit drugs in Nigeria.
E – Elizabeth Garrett Anderson
The first woman to qualify as a physician and surgeon in Britain.
F – Françoise Barré-Sinoussi
Virologist and co-discoverer of HIV; Nobel Prize laureate.
G – Gerty Cori
Biochemist who co-discovered the Cori cycle explaining glycogen metabolism; Nobel Prize laureate.
H – Harriet Brooks
Nuclear physicist who made early discoveries in atomic recoil and radioactive decay.
I – Ida Henrietta Hyde
Physiologist who developed one of the first microelectrodes for cellular research.
J – Juanita Merchant
Gastroenterologist whose research advanced understanding of gastric disease and inflammation.
K – Katherine Johnson
Mathematician whose orbital calculations were critical to early U.S. space missions.
L – Lynn Margulis
Evolutionary biologist known for the endosymbiotic theory of cell evolution.
M – Mae Jemison
Engineer, physician, and the first African-American woman in space.
N – Noreen Murray
Molecular geneticist who helped pioneer recombinant DNA technology.
O – Olga Ladyzhenskaya
Mathematician known for foundational work on the Navier–Stokes equations.
P – Patsy O’Connell Sherman
Chemist and co-inventor of Scotchgard.
R – Rosalind Franklin
Chemist and X-ray crystallographer whose work was crucial to understanding DNA’s structure.
S – Stella Adadevoh
Physician who helped contain the Ebola outbreak in Nigeria in 2014.
T – Thelma Estrin
Computer scientist who helped design early biomedical computing systems.
U – Uta Frith
Psychologist whose research advanced understanding of autism and theory of mind.
V – Virginia Apgar
Physician who created the Apgar score for assessing newborn health.
W – Wangari Maathai
Environmental scientist and founder of the Green Belt Movement; Nobel Peace Prize laureate.
X – Xia Peisu
Xia Peisu, pioneer of computer science in China.
Y – Yvonne Barr
Virologist and co-discoverer of the Epstein–Barr virus.
Z – Zeng Fanyi
Stem cell scientist who demonstrated mammalian generation from induced pluripotent stem cells.
When I finished, the room was quiet.
“Women have always been in science,” I said. “History just doesn’t always amplify them.”
My classmate slowly stood up and applauded.
The class followed.
This man had 4 minutes to live. No one was in the room. He survived because he knew something 95% of the world doesn’t.
Choking kills over 365,000 people globally every year, according to the WHO.
95% of these choking episodes share one variable: the person was alone. Not because the obstruction was worse. Because no one was there to help, and the victim didn’t know how to help themselves.
Without oxygen, brain damage begins in as little as 4 to 6 minutes. Average ambulance response time globally? Eight minutes or more. In many countries, they don’t arrive at all. The math is unforgiving.
You either know what to do in the first 60 seconds, or you don’t survive long enough for help to arrive.
This man survived for one reason, he’s a medical worker. He knew the self-Heimlich exists. He knew to use the back of a chair to generate subdiaphragmatic thrust against his own epigastrium.
That’s not his instinct. It’s training.
Now think about who doesn’t have that training. Elderly people eating alone. Toddlers. Anyone living by themselves who has never been shown that a chair, a countertop, or even your own fist can substitute for another person’s hands.
The Heimlich maneuver was invented in 1974. Fifty years later, most people on Earth still don’t know it exists, let alone that you can perform it on yourself.
112K+ people watched this video. Almost none of them would have thought of actually learning the technique. They watched a man almost die and just felt relieved.
Here’s what the video should have taught you:
In case you’re alone and choking:
Step 1: Make a fist. Place the thumb side just below your rib cage, above your navel.
Step 2: Grasp it with your other hand. Thrust sharply inward and upward.
Step 3: If that doesn’t work, lean over any firm surface. A chair back. A countertop edge. A railing
Step 4: Drive your upper abdomen against it. Hard. Repeat until the airway clears.
That’s 15 seconds of knowledge. Don’t forget that. Save this post.
Many children are quickly labelled stubborn, difficult, or disrespectful.
But often, what we’re seeing is a child who doesn’t feel heard.
When children feel ignored, misunderstood, or constantly corrected without being listened to, they express it through behaviour.
Behaviour is communication.
This doesn’t mean there should be no boundaries. It means listening should come before correction.
When parents slow down to understand their child’s feelings and thoughts, resistance often reduces.
If you’re constantly clashing with your child and nothing seems to work, the issue may not be stubbornness but a communication gap.
Just to quickly put this out there:
IF you ever see anyone having a seizure that does NOT stop within 5minutes, please lie that person down on their left side and call an ambulance ASAP.
Do NOT pour water on them.
Do NOT put anything in their mouth.
Just lie them down and call an ambulance. If no ambulance, take them to hospital in a car ASAP.
Any seizure more than 5mins;
The person’s brain and heart is under attack. If that seizure isn’t terminated, the person will die.
This is NOT a joke.
Save this tweet. You may need it one day to save someone. Pls share it everywhere. Help save someone’s life.
HAPPY INTERNATIONAL EPILEPSY DAY.
Physiotherapy students on the timeline!!!
I genuinely love the enthusiasm I see from many of you, and I look forward to welcoming you into a profession I am deeply proud of.
That said, a gentle but important reminder.
While this is your personal page and you are free to share opinions or general advice, problems arise when advice is presented under the banner of physiotherapy by someone who is not yet qualified. At that point, there is a real risk of giving inappropriate or misleading information, even if the intention is good. That line sits uncomfortably close to misinformation.
Physiotherapy is a protected and highly regulated profession. Until you are fully qualified and registered, you are not entitled to present advice as physiotherapy advice or speak on behalf of the profession.
By all means, share thoughts, experiences, or general wellbeing tips. Just avoid framing them as physiotherapy guidance until you are actually a physiotherapist.
Before one of you comes and say something unwise to me, know that I am not gatekeeping. It is about protecting the profession, the public, and your future professional credibility.