Pulmonary vein perforation causing life-threatening pulmonary hemorrhage during pulsed field ablation for atrial fibrillation using a J-shaped radiofrequency transseptal puncture wire
@yoshitake_3
https://t.co/m56joXSk0z
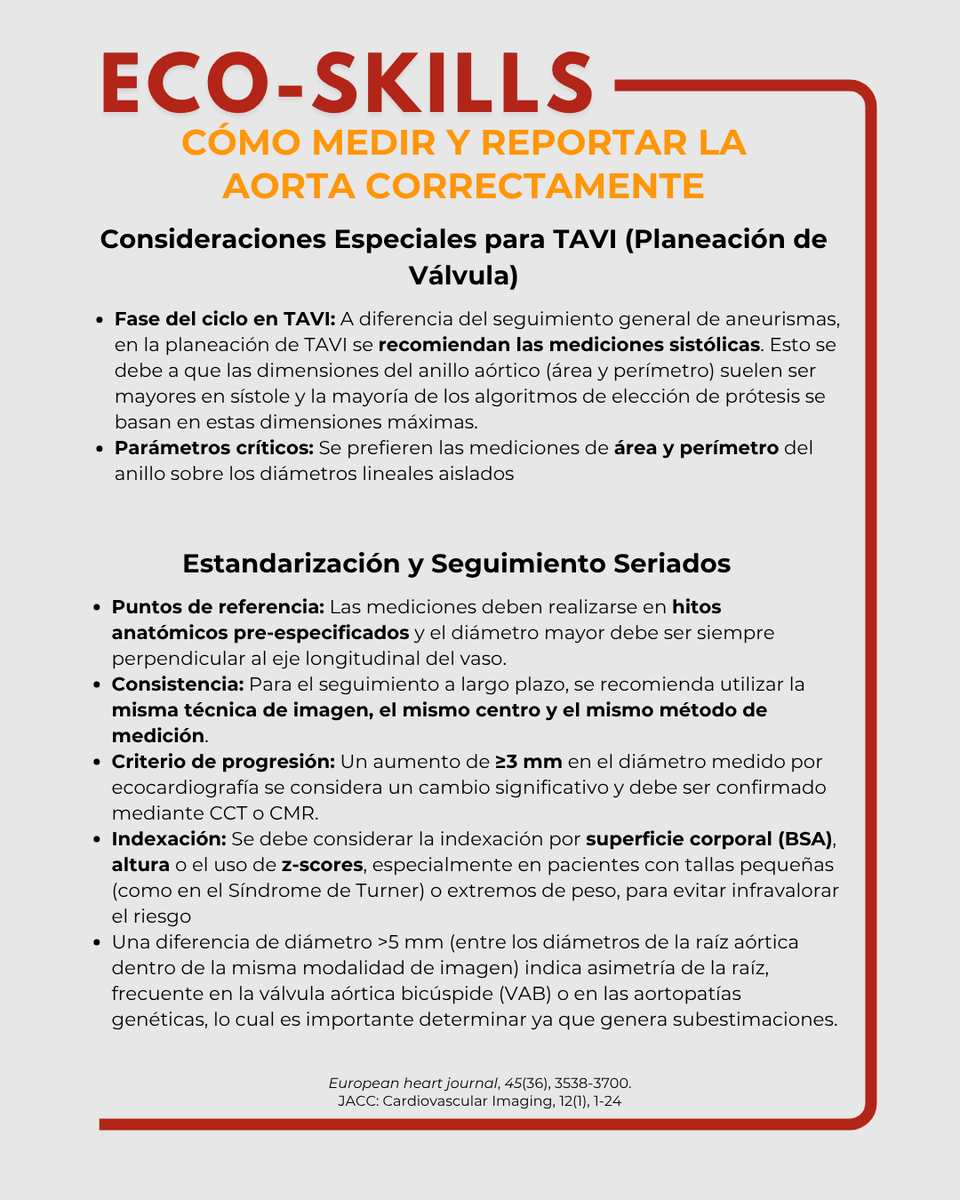
🛠️ ECO SKILLS | Medición de la aorta
Las guías ESC 2024 y recomendaciones TAVI/TAVR enfatizan la estandarización para lograr mediciones reproducibles y precisas.
📏 Medir bien = mejores decisiones clínicas.
#SONECOM#ECOSKILLS#Aorta#Ecocardiografía
🫀 This paper is quietly dangerous. Not because it’s wrong— but because it can be misunderstood.
Let’s go straight to the core.
What the study actually shows
In 479 CCS patients undergoing CCTA:
👉 Lower LDL-C (<70 mg/dL)
was associated with
👉 MORE severe CAD and higher plaque burden
Even more interesting:
👉 These patients had
- more diabetes / pre-diabetes
- more metabolic syndrome
- worse glucose metabolism markers
And:
👉 Diabetes (OR ~6.1) and pre-diabetes remained strong independent predictors of CAD risk
The uncomfortable observation
👉 The “best treated” patients (low LDL) had the worst arteries
Before anyone panics:
This is NOT saying LDL reduction is harmful.
This is saying something much more subtle—and more important.
What is really happening?
1. Reverse causality (the elephant in the room)
Patients with:
👉 prior events
👉 higher baseline risk
👉 more aggressive treatment
→ end up with lower LDL
So:
👉 Low LDL is a marker of treated high-risk patients
Not the cause of disease.
2. Metabolic risk is the real signal
The study shows very clearly:
👉 Glucose dysregulation dominates residual risk
- Diabetes
- Pre-diabetes
- Insulin resistance
- Metabolic syndrome
→ strongly associated with plaque burden and Leiden score
This is the key shift
For years, we simplified CAD risk to:
👉 LDL = bad → lower is better
That’s still true.
But incomplete.
What this paper actually teaches
👉 You can have “perfect LDL” and still have high atherosclerotic risk
Because:
👉 Atherosclerosis ≠ cholesterol alone
👉 It is a metabolic + inflammatory + vascular disease
The imaging angle (the real gold here)
CCTA shows:
👉 more non-calcified plaques in low LDL group
👉 higher plaque burden (SIS)
👉 higher Leiden risk scores
This is exactly where imaging becomes decisive:
👉 Biology > numbers
Clinical implication (the part guidelines are still catching up with)
Treating LDL alone:
❌ does NOT eliminate risk
Because:
👉 residual risk = metabolic + inflammatory + phenotypic
My take
This paper reinforces a concept that is still underused clinically:
👉 CAD is an atheroma disease, not a cholesterol disease
The real mistake to avoid
A superficial reading would lead to:
❌ “Low LDL is associated with more disease → LDL doesn’t matter”
That would be wrong.
The correct interpretation
👉 LDL lowering works
👉 BUT it does not address the whole disease
Where this goes next
This is exactly where:
👉 advanced CCTA (plaque quantification, phenotype)
👉 PCCT (microstructure, composition)
👉 AI-QCT
will redefine risk stratification.
Bottom line
👉 LDL reduction is necessary
👉 but absolutely not sufficient
And if you only track LDL:
👉 you are managing a number
👉 not the disease
The current physical activity guidelines are too low.
I've been saying this for a while. And a new study confirms it.
Meeting the standard 150 minutes/week was associated with only a modest ~8–9% lower cardiovascular risk.
The biggest protection occurred at roughly 560–610 minutes/week, about 3–4× higher, where cardiovascular risk was 30% lower.
We need to distinguish between the minimal activity volume required for basic protection, and the substantially higher volumes required for optimal resilience.
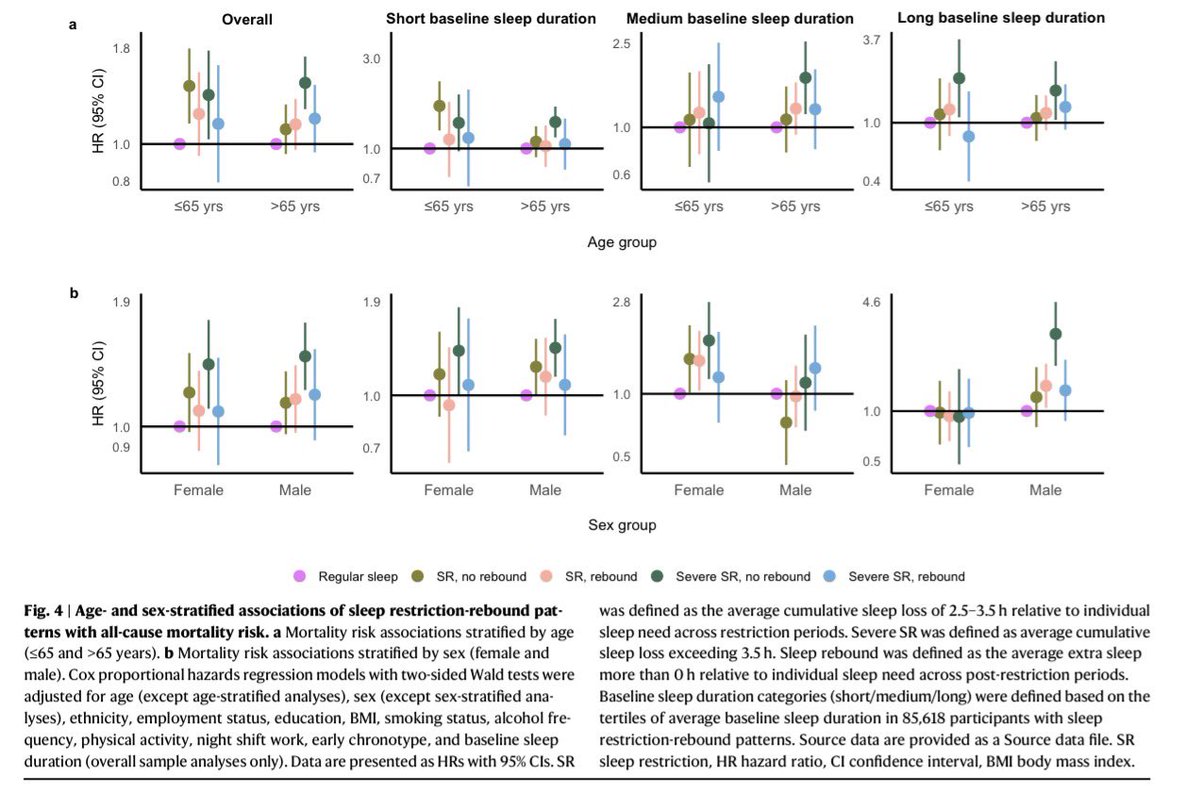
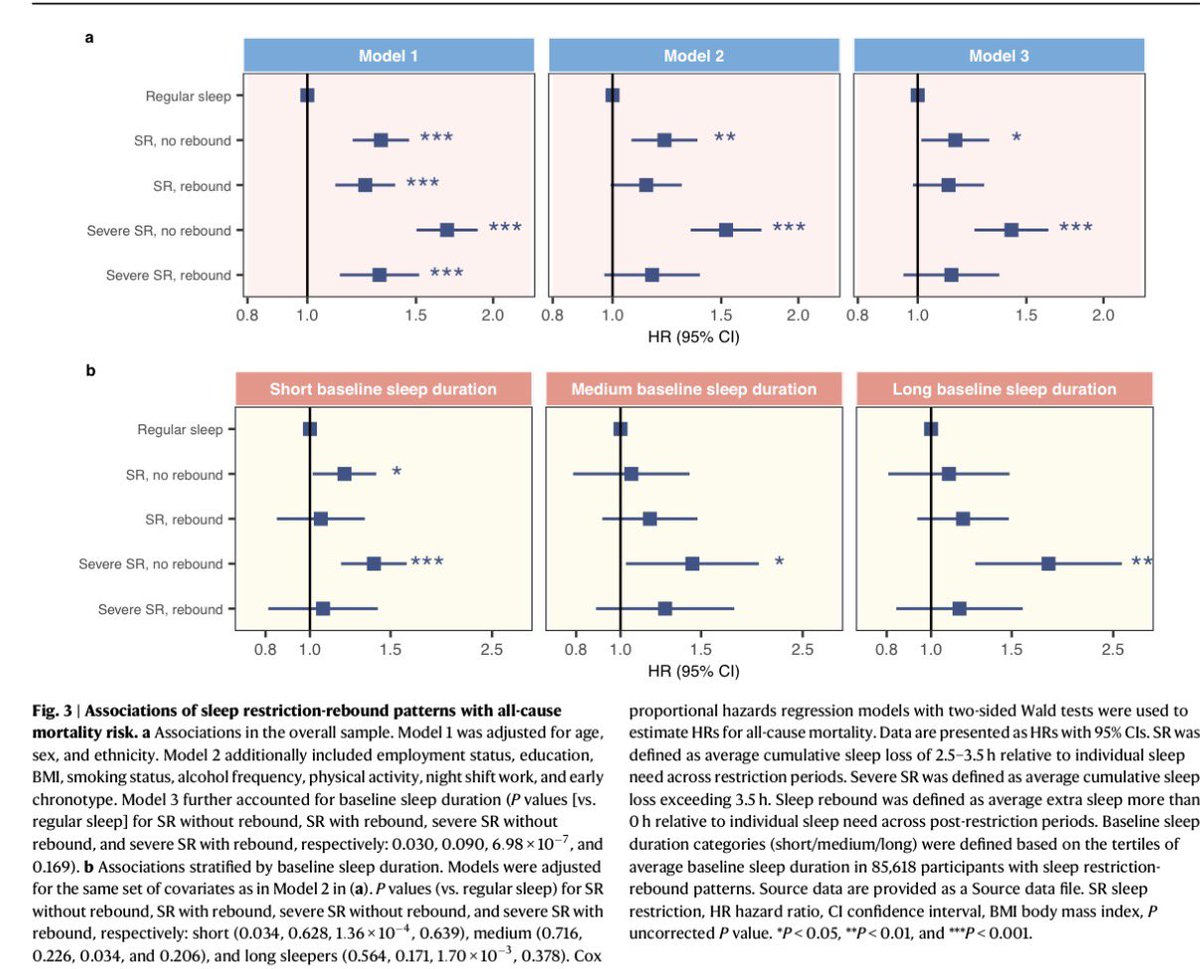
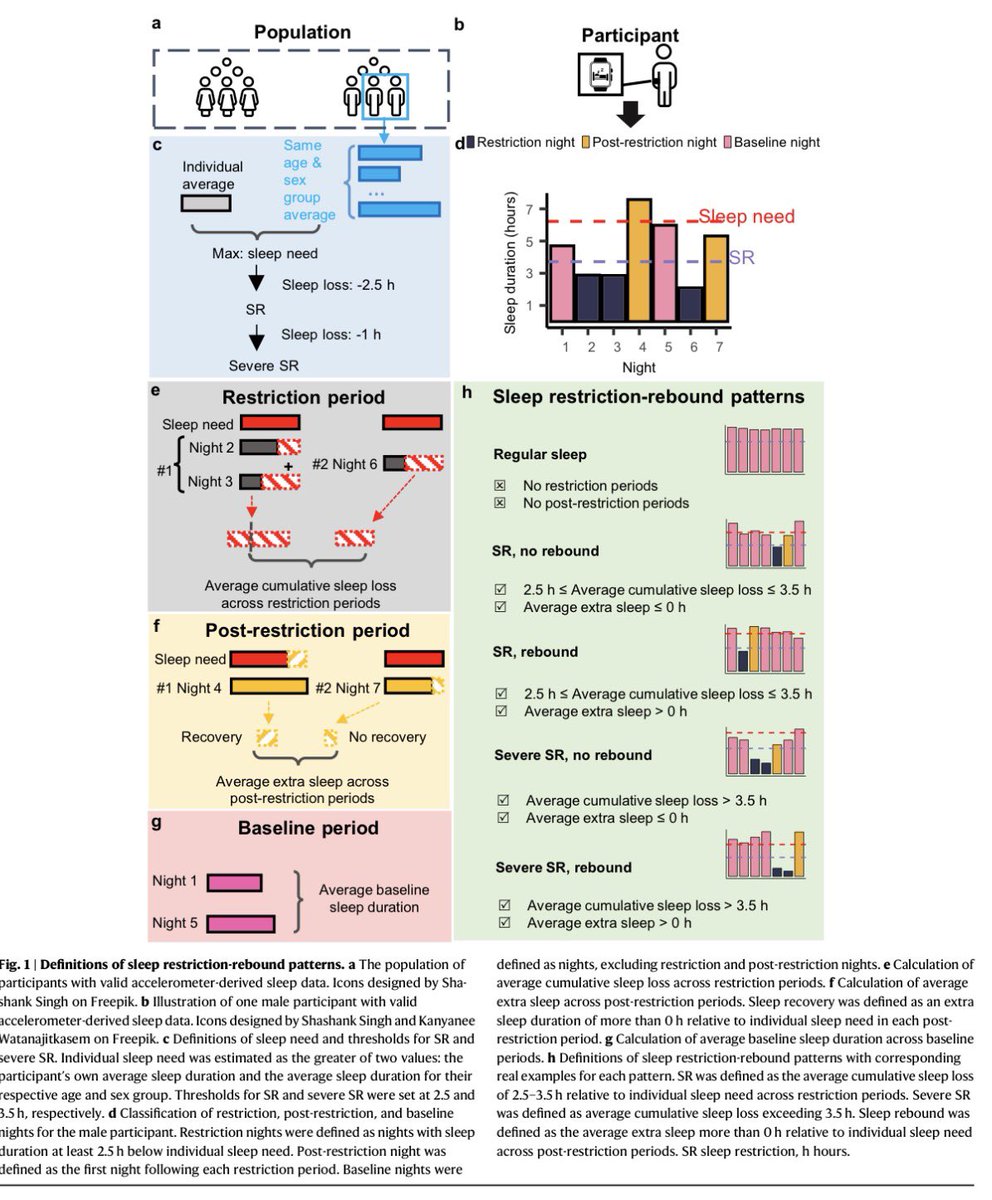
Dormir de más al día siguiente SÍ importa.
📍85,618 personas, 8 años de seguimiento: privarte de sueño sin recuperarte después aumenta mortalidad hasta 42%. Pero si duermes y repones el sueño la noche siguiente, el riesgo desaparece.
La deuda de sueño crónica sin reponerlo sigue siendo dañina.
By @Nature
🔗Descarga:
https://t.co/nPANmbzMrl
DOI:
https://t.co/WgKo5xMdHv
His claim is correct. We have a fertility crisis.
> 62% sperm count drop globally 1973 - 2018
> 23% drop in just 16 years
> rate of decline accelerating
> dropping 2.64% per year since 2000
I explain below how to improve yours.
I've been working on improving my fertility markers for the past two years.
They are elite for a early 20 something (I'm 48).
Total motile count: 411 million
Motility: 64%
Morphology: 12%
Concentration: 212 million
Count: 642 million
To put these numbers into perspective: the WHO considers a motile count above 42 million as normal, mine is 411 million, nearly 10x.
And a normal concentration is 16 million (mL), mine is 212 million (mL).
These personal-best fertility markers coincided with my first-in-human test result showing zero microplastics in my semen. Studies have shown 100% of men have microplastics in their semen.
Microplastics hurt sperm.
Human studies show the impact of various types of plastic, associated chemicals, and other toxins on male fertility:
+ 60% fewer normal shaped sperm (from PFAS)
+ 5x higher odds of low sperm count (from PTFE)
+ 10% lower sperm concentration (from PTFE)
+ 15% lower swimming ability (from PTFE)
+ 41% lower swimming ability (from PET)
+ 12% lower sperm swimming ability (from BPA)
+ 3x higher odds of low sperm count (from Phthalates)
+ 2x higher odds of poor swimming (from Phthalates)
How to improve your fertility:
> 7 to 9 hours of sleep, consistent bed and wake times
> exercise: cardio fitness, strength, and muscle
> reducing body fat and build lean mass
> avoid alcohol, tobacco, and cannabis; each independently reduces sperm concentration, motility, and morphology, with cannabis also affecting sperm methylation.
> cut junk food, added sugars, and excessive saturated fats
> eat an anti-inflammatory, anti-oxidant diet (Mediterranean and green-Mediterranean): polyphenols, fiber, olive oil and other MUFAs, omega-3s (algal, fish, walnuts), plant protein, fresh veggies.
> get full micronutrient coverage: zinc, selenium, folate, vitamins C, E, and D (blueprint solves this).
> manage stress and cortisol load; chronic stress lowers testosterone and impairs spermatogenesis.
Things I'm doing:
1. Sauna (dry). My toxin blood panel confirms sauna clears plastic related chemicals: BPA, phthalates, PFAS, flame retardants, pesticides. The plastic particles themselves are too big to sweat out directly. Heat may activate other clearance routes: bile flow through the liver, the cell's internal cleanup system, and the gut barrier. Humans have almost no enzymes that can break plastic apart, so the body has to physically push it out.
2. Reverse osmosis water filter. Drinking water is likely a major source of microplastic getting into your body. A reverse osmosis filter pushes water through a very tight membrane and strains the particles out. I filter everything I drink.
3. Trying to rid my environment of the big plastic items: cutting boards, cups, plates, food storage containers, non-stick pans, cling wrap, tea bags, water bottles, kitchen utensils, kettles, and synthetic clothing. Note, as hard as I try, I'm always finding new plastic things in my life. This can be all-consuming thing so try to just knock out the big ones.
The studies:
> meta-analysis with total 42,935 men; significant decline in both sperm concentration and total sperm count among men from Western countries, with total sperm count by about 59%, between 1973 and 2011.
> A follow-up global meta-analysis, expanded the dataset to 223 studies and 57,168 men found the drop in sperm count was not only a Western phenomenon
> total sperm count dropped by 62% globally between 1973 and 2018, including in men from South America and Asia. The rate of decline has also accelerated since 2000, reaching approximately 2.64% per year.
> CDC data also showed US fertility rates peaking at the replacement level of 2.12 births per woman in 2007, then taking a sharp downward turn by 23% down to 1.62 in 2023.
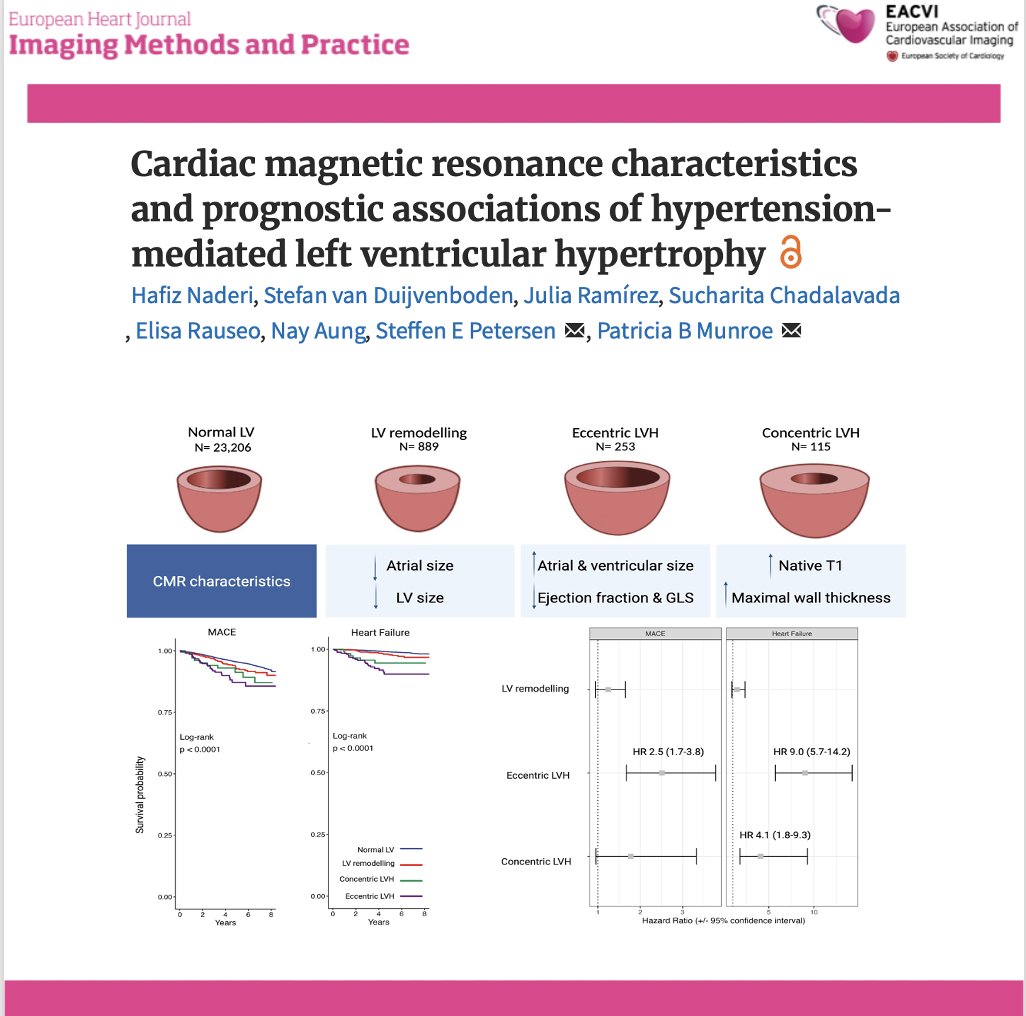
📄 Hypertension-related LVH: not all phenotypes carry the same risk
🔗 DOI: https://t.co/W1SFC0ZCz6
🫀 Hypertension is the most common cause of LV hypertrophy—but its cardiac expression is far from uniform.
This large UK Biobank CMR study (n >24,000) provides a comprehensive look at LVH phenotypes and their prognostic impact.
✨ Four CMR-defined phenotypes:
👉 Normal LV
👉 LV remodelling
👉 Eccentric LVH
👉 Concentric LVH
📊 As shown in the graphical abstract (page 2):
➡️ each phenotype has distinct structural and functional signatures
✨ Key findings:
🔹 Eccentric LVH = worst phenotype
➡️ Most impaired LV function (EF + strain)
➡️ Largest chambers
➡️ Highest risk:
MACE → HR 2.5
Heart failure → HR 9.0
🔹 Concentric LVH:
➡️ Highest wall thickness and native T1 (fibrosis)
➡️ ↑ Heart failure risk (HR 4.1)
➡️ No significant MACE association
🔹 LV remodelling:
➡️ Intermediate phenotype
➡️ Smaller chambers, milder changes
📊 Key pathophysiological insight:
👉 LVH is not a binary condition—but a spectrum of myocardial adaptation
➡️ From remodelling → concentric or eccentric hypertrophy
➡️ Driven by pressure load, volume load, and myocardial response
💡 Clinical take-home message:
👉 Not all LVH is equal
✔ Eccentric LVH → high-risk phenotype
✔ Concentric LVH → fibrotic, HF-prone phenotype
👉 CMR enables:
precise phenotyping
improved risk stratification
potential tailored treatment strategies
🚨 Bottom line:
In hypertension, LV geometry matters—because different phenotypes carry very different prognoses.
#Cardiology #CMR #Hypertension #LVH #CardiacImaging #HeartFailure #RiskStratification #PrecisionMedicine #UKBiobank 🫀📊
Fruits & vegetables likely account for a majority of people's dietary microplastic and PFAS intake.
What’s frustrating is that this isn’t something you can just rinse off. In many cases, the contamination appears to be taken up into the food itself.
Organic may reduce some of that exposure, but even organic farms can be affected when they’re near contaminated land or water.
Should you stop eating produce? No. We should be much more upset about how widespread these chemicals have become, especially when children are being exposed through foods we otherwise consider healthy.
One practical thing I think is worth considering is beta-glucan. There’s some evidence it may help support the excretion of PFAS, and given how unavoidable these exposures are becoming, that may be a useful tool, especially for families who can’t realistically eliminate every source.
🫀 Myocardial perfusion imaging (MPI) is routinely used to assess ischaemia in CTO patients—but does it actually predict outcomes after PCI?
This large registry study provides an important answer.
✨ Study at a glance:
🔹 319 patients undergoing CTO-PCI
🔹 65% had moderate–severe ischaemia (≥10% LV)
🔹 Follow-up: 90 days + 5 years
✨ Key findings:
🔹 No difference in hard outcomes between groups:
➡️ all-cause mortality
➡️ MACCE (MI, stroke, HF, CV death)
🔹 At both 90 days and 5 years:
👉 ischaemia burden did NOT predict prognosis
📊 But here’s the nuance:
🔹 Patients with higher ischaemic burden had:
➡️ lower risk of angina hospitalisation at 5 years
👉 Suggesting a greater symptomatic benefit from CTO-PCI
⚠️ Important considerations:
👉 Ischaemia defined globally (≥10% LV), not vessel-specific
👉 Mix of SPECT and PET imaging
👉 No comparison with medical therapy alone
💡 Clinical take-home message:
👉 Ischaemia is not a prognostic marker after CTO-PCI
👉 But it may help identify patients:
✔ more likely to benefit symptomatically
✔ with greater improvement in quality of life
🧠 This reinforces a growing concept:
👉 CTO-PCI should be:
symptom-driven, not ischaemia-driven
👉 Imaging should guide selection—but not dictate it
🚨 Bottom line:
More ischaemia ≠ better outcomes—only better symptom relief.
#Cardiology #CTO #PCI #Ischaemia #CardiacImaging #PET #SPECT #CoronaryArteryDisease #InterventionalCardiology #QualityOfLife 🫀📊
#EHJCVI 🫀 Time to refine #echofirst quantification of aortic regurgitation? 🔍 Using #whyCMR as reference, a 2-step TTE algorithm (RegVol≥45 mL + LVEDVi≥93 mL/m²) outperformed traditional criteria for severe AR definition‼️ #VHD ⏩Read more: https://t.co/g7xUAkbhOM
Se rompió lo imposible: un humano baja de las 2 horas en maratón
No es historia del deporte. Es historia de la humanidad.
El keniano Sabastian Sawe acaba de lograr lo que durante décadas se consideró inalcanzable: correr una maratón en menos de dos horas en Maratón de Londres.
Con un tiempo de 1:59:30, Sawe rompe la barrera más simbólica del atletismo y redefine el límite físico del ser humano.
Durante años, el sub-2 fue una obsesión para atletas, científicos y marcas. Muchos lo intentaron. Nadie lo había logrado en competencia oficial… hasta hoy.
Este no es solo un récord. Es un punto de quiebre.
Hoy, la humanidad es un poco más rápida.
#Maratón #Running #Historia #Atletismo #LondonMarathon #BreakingLimits