The architecture for America's current dominance in biotech was crafted by bipartisan consensus in Hatch-Waxman.
To sustain American leadership, we must continue to innovate, both in the lab and in Congress.
https://t.co/drgAZQRjJF
Expediting the drug approval process and reforming the FDA are critical to speeding innovation and providing Americans with invaluable treatments.
We need more proposals like this one from @RepAuchincloss, regardless of what side of the aisle they come from, that advance American biotech and ensure our continued leadership.
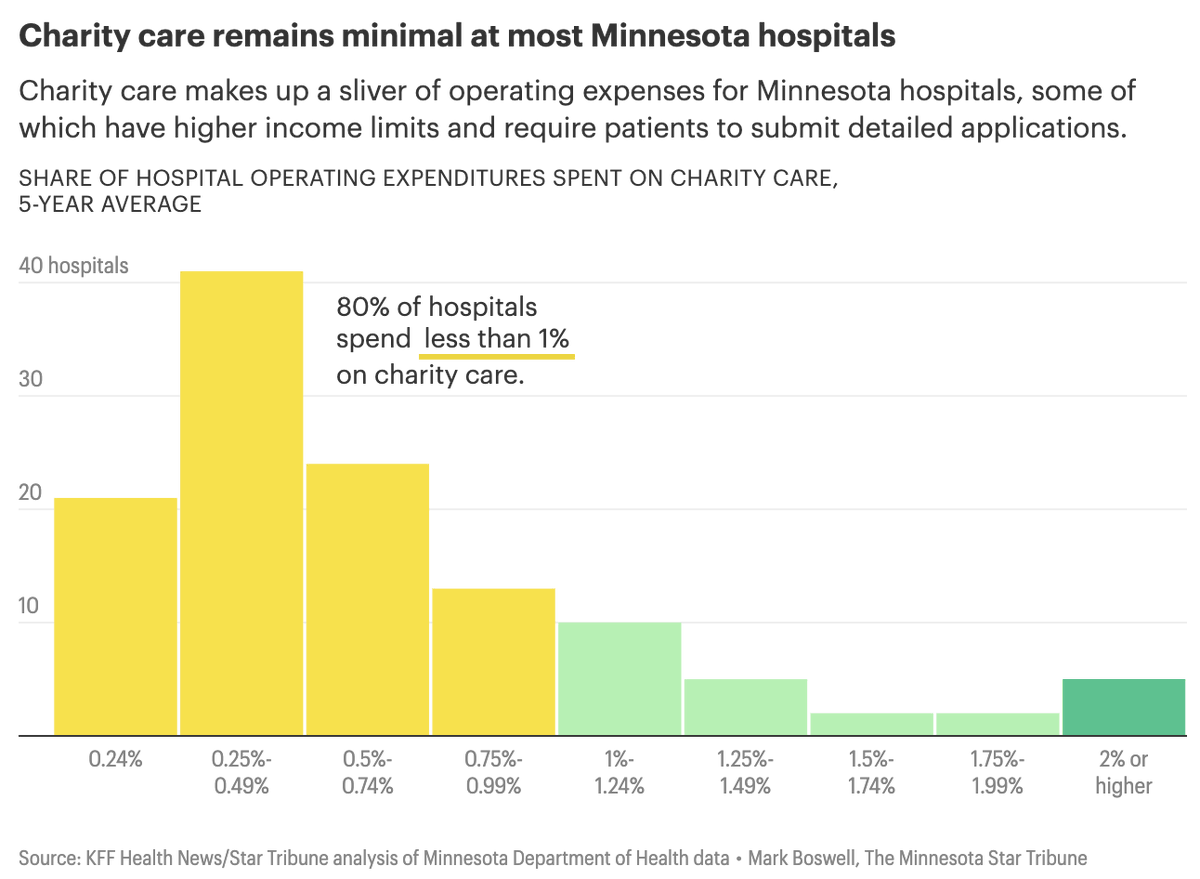
�� Minnesota hospitals are receiving major tax breaks as “nonprofits” while spending far less on charity care than hospitals almost anywhere else in the country.
80% spend less than 1% of operating expenses on charity care.
Vulnerable patients are left with higher bills, debt collectors, and lawsuits.
These lawsuits merely weaken incentives for medical breakthroughs and penalize companies that are crucial for America's biotech leadership.
https://t.co/XwvHdAnTl4
As @WSJ said of the lawsuit against Gilead, “If the state high court lets this ruling stand, it won’t merely distort product-liability law; it will punish medical progress.”
Biopharma companies should not face liability for innovation timeframes.
.@sallypipes is right: The notion that pharmaceutical firms should be sued for not “innovating quickly enough” is ludicrous.
The lawsuit against Gilead could set a dangerous precedent.
The ACA, DEI initiatives, and 340B have contributed to skyrocketing healthcare costs in recent years.
As a recent report from @Paragon_Inst highlights, endless taxpayer subsidies to hospitals don't fix the problems; they exacerbate a broken system. 👇
https://t.co/Cpr2R9NCQk
.@alexberenson rightly notes that hospital prices are exploding, “due to the costly bureaucratic and health information software requirements that the federal government imposes and Obamacare has worsened… and managing diversity, equity, and inclusion programs.”
https://t.co/eUdwDsO8G9
.@RepJasonSmith exposes the 340B grift and explains how wealthy hospitals rake in taxpayer dollars:
“Profit-seeking health systems view struggling rural hospitals as nothing more than a gateway to more patient referrals.”
340B burdens patients and rural hospitals.
Paul Avelar for @IJ compares suppression of DTC ads to censorship in the past:
“Sorrell was about suppressing raw information because the government didn’t like that drug companies could use it to inform doctors…”
Disliking information does not justify censoring it.
NEW REPORT: Paragon says federal policies like provider taxes, state-directed payments, higher reimbursements for hospital-owned outpatient sites, and 340B loopholes are supercharging hospital consolidation and driving up health care costs.
If Washington is serious about affordability, site-neutral payments, transparency, and real 340B accountability should be on the table.
https://t.co/qXSLaxLPkz
.@RealJoeGrogan explains that 340B has strayed from its original purpose of helping low-income patients:
“This program has expanded — not through congressional action — but through congressional inaction, approval, and even encouragement on the part of the bureaucrats at HRSA…”
.@rclong1997 highlights an underlying issue with 340B:
“340B hospitals that have large amounts of commercially-insured patients and small amounts of uninsured patients are going to end up getting vastly more from the program than those [hospitals] that are struggling…”
WATCH: @rclong1997 details how 340B has expanded over the years, citing the addition of 340B-eligible entities, Medicaid expansion for able-bodied adults, and contract pharmacy:
A clearer definition of who qualifies as a 340B patient is long overdue.
When the rules are vague, the program becomes harder to oversee and easier to stretch beyond its original safety-net purpose. More clarity would help protect accountability and ensure discounts are tied to actual patient care.