🧠🫀 When cardiology forgets to ask “why”: a timely wake-up call
This 2025 Open Heart viewpoint by Francesco Tona is not an attack on modern cardiology—but a deeply reasoned warning about what we risk losing amid unprecedented technological power .
⚙️ The paradox
Cardiology has never been more capable. We replace valves percutaneously, map anatomy in exquisite detail, and deploy AI to predict risk. Yet, the author argues, capability is increasingly replacing curiosity. Decisions are often driven by what can be done, not whether it should be done.
🧠 From “why” to “can”
Historically, cardiology advanced through physiologic questions and clinical reasoning. Today, the sequence is reversed:
- A device appears
- Anatomy fits
- The procedure proceeds
- Reflection, appropriateness, and patient-centred benefit too often come after execution—if at all.
🩺 When feasibility replaces judgement
Tona highlights a subtle but dangerous shift:
- Anatomical suitability eclipses clinical appropriateness
- Procedural success is mistaken for patient benefit
- Futility becomes “well-executed” rather than questioned
This is not failure of skill—but failure of restraint.
💼 The silent drivers
Industry influence, guideline structures, and training environments normalize interventionist reflexes. Research increasingly validates existing technologies using surrogate endpoints, while negative or null results fade into obscurity.
🤖 AI: help or shortcut?
AI can augment care—but risks outsourcing thinking. When clinicians validate algorithmic outputs instead of interrogating them, clinical reasoning atrophies. Precision without purpose is not progress.
🔮 The real message
This is not anti-innovation. It’s a call to reclaim the “why”:
Teach restraint as a clinical skill
Design guidelines around meaningful patient benefit
Prioritize outcomes that matter to patients, not systems
🧭 Bottom line
When cardiology stops asking why, it doesn’t become more efficient—it becomes less human.
Technology should serve judgement, not replace it.
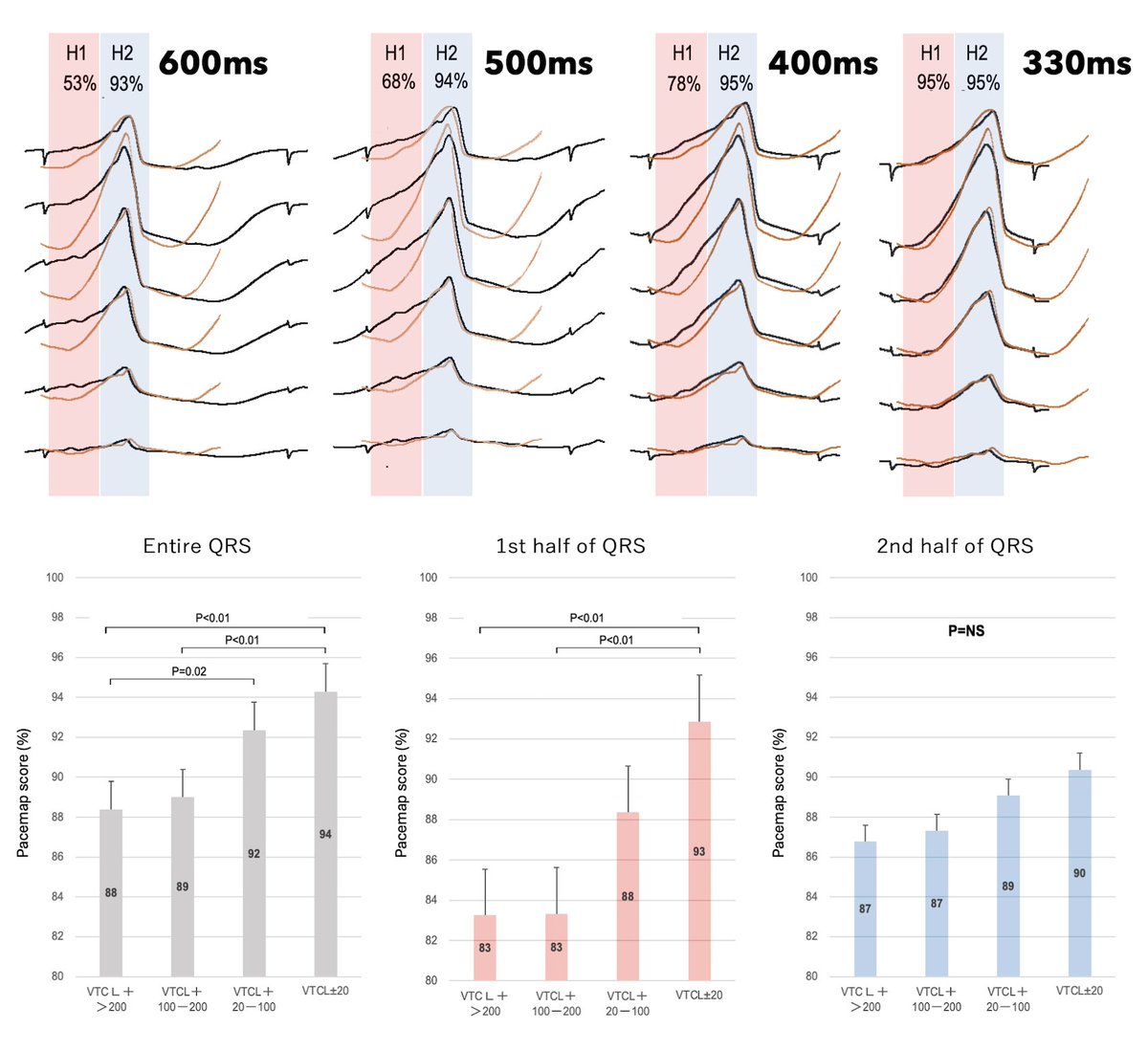
How many #EPeeps pacemap at the rate of VT?
Pacing faster creates more "TR fusion", making all pacemaps look more "epicardial".
Congrats to @yasushinoda1029@ZJameria on this work that should make us all question determination of initial slurring/ pseudodelta waves. #QSQ
""Rate-Dependent Pacemap Matching in Scar-Related Ventricular Tachycardia: TR Fusion Phenomenon"
https://t.co/xJtHiwwPiO
This is what we are building in Phoenix.☀️🌵
Ceiling and Visibility Unlimited.🚀
This is the new Banner – University Medicine Phoenix Heart Institute https://t.co/iN13npT8SF
United Healthcare is enforcing peer to peer for pacemaker implant for symptomatic sick sinus syndrome. @UHC won’t even approve a dual pacemaker implant without a peer to peer. Is there a different definition of “harassment” @HRSonline@ACCinTouch#epeeps
Had to share! Students at Dixie Bee Elementary raised money for those impacted by Tornado in Sullivan. They raised $1,610. How about kindergartner Arnab Jameria "I brought 200 from my piggy bank. So they can get their homes back and their things and their houses back"
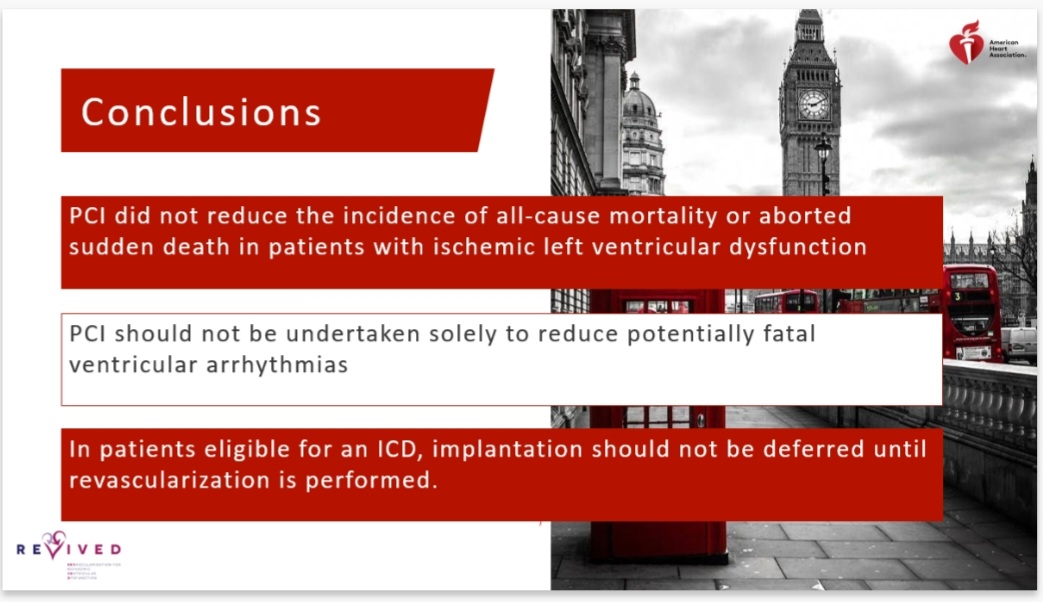
Packed room this morning at #AHA22 for the @REVIVED_BCIS2 arrhythmia results!
No difference seen in the primary outcome of death or aborted sudden death between PCI and OMT @divaka_perera@AHAScience
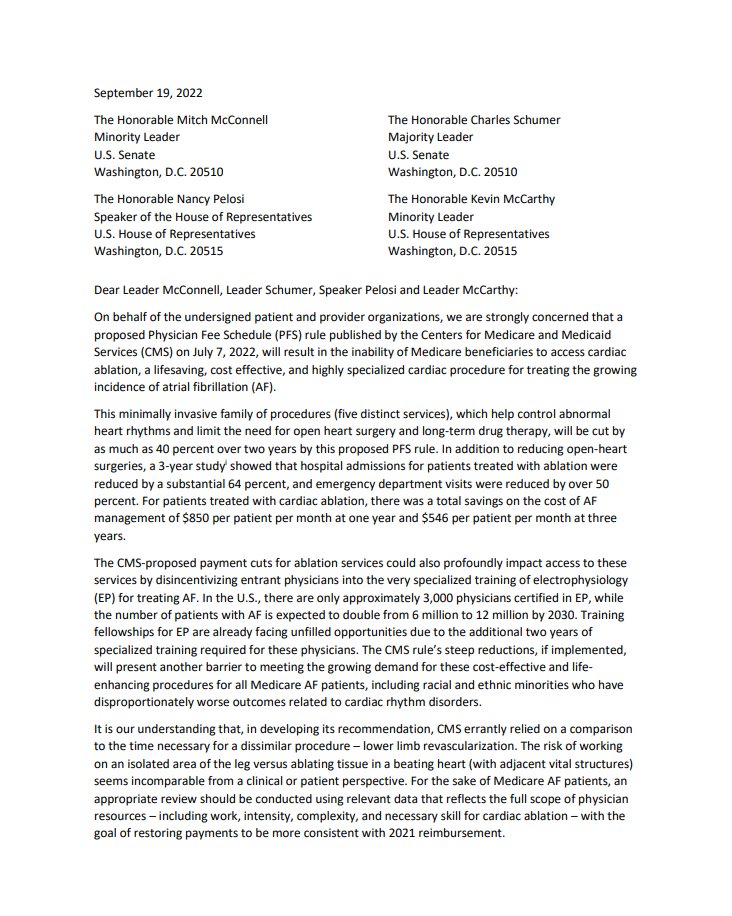
https://t.co/PrIhZgfC2D - please visit our newly launched advocacy platform to save the field of cardiac electrophysiology. This will allow you to directly email all of your congressmen/congresswomen about the devastating CMS cuts that threaten to destroy EP! @ep_advocacy#epeeps
If you’re at #ESCCongress2022, stop by the Wisepress stand J570 and preview the groundbreaking Atlas of Cardiac Anatomy by Drs. Shumpei Mori and Kalyanam Shivkumar @shivkumarmd Take a look at the stunning images https://t.co/HYndUn46J6
AF 93656 from 19.77 wRVUs to 15.8 wRVUs
SVT 93653 from 14.75 to 13.8 wRVUs
VT 93654 from 19.75 to 16.9 wRVUs
Why did 93654 drop? Because the RUC wanted to maintain a 3.10 wRVU difference between 93653 and 93654. Unreal!
I have started meeting with a psychologist to get some help.
I share this to encourage others who may benefit from the same.
Honestly, I think everyone needs it.
And we need to be more open about the challenges we face as healthcare workers having experienced moral injury.
Reading this letter made me upset again. BEP denied for testicular cancer. Fortunately, the patient has already started treatment after a successful appeal. But why is the system like this? #physicianburnout#priorauth