Una grandísima revisión de "Manejo de falla cardíaca descompensada" en JACC 2026. Puntos importantes actualizados:
🟠 Se añaden umbrales confirmatorios de falla: BNP >400 ng/L o NT-proBNP ajustado por edad (>450 ng/L en <50 años; >900 ng/L en 50-75 años)
🟠 Dosis inicial de furosemida — antes: 1-2.5 veces la dosis oral previa. Ahora: 40 mg IV en pacientes sin diurético, y si ya usaba: ≥80 mg IV o dos veces la dosis oral.
🟠 Ahora se sugiere valorar a las 2 horas buscando: uresis ≥300 mL o Na urinario ≥70–80 mmol/L.
🟠 Si hay resistencia ahora se sugiere duplicar el bolo hasta 250 mg de furosemida, considerar acetazolamida o tiazida.
🟠 Ahora se sugiere secuenciación temprana para usar iSGLT-2, ARM (como Espironolactona), ARNI, betabloqueador antes del alta.
Completo en el canal (https://t.co/3O93s10lns).
🫀Hypertension in 2026: Five practice changing updates every clinician should know
Hypertension remains the leading modifiable risk factor for cardiovascular disease worldwide, yet recent evidence suggests that many patients continue to be undertreated.
The updated Annals of Internal Medicine "In the Clinic" review summarizes the most important changes introduced by the 2025 AHA/ACC guideline and highlights how hypertension management is evolving.
The first major change is that blood pressure should no longer be judged solely in the clinic.
Out of office blood pressure monitoring is now strongly recommended not only to confirm the diagnosis, but also to detect white coat hypertension, masked hypertension and guide treatment titration. Ambulatory blood pressure monitoring remains the reference standard whenever available.
The second message is that lower targets matter.
For most patients, the recommended goal remains below 130/80 mmHg, with increasing evidence supporting systolic pressures below 120 mmHg in selected high cardiovascular risk patients when tolerated. Recent trials demonstrated reductions in major cardiovascular events without a significant increase in serious complications.
Third, lifestyle interventions continue to be the foundation of therapy.
Weight reduction, dietary sodium restriction, the DASH diet, regular exercise and potassium enriched salt substitutes remain among the most effective nonpharmacological interventions. Emerging evidence also supports meditation and yoga as useful adjunctive therapies for selected patients.
Fourth, treatment should become increasingly individualized.
The guideline incorporates overall cardiovascular risk into treatment decisions using the new PREVENT risk calculator instead of relying exclusively on blood pressure values. This approach better identifies patients who derive the greatest benefit from earlier pharmacological therapy.
Finally, resistant hypertension is no longer a therapeutic dead end.
Mineralocorticoid receptor antagonists remain central to treatment, while newer agents such as aprocitentan, a dual endothelin receptor antagonist, expand therapeutic options for carefully selected patients with resistant hypertension.
The most important lesson is simple.
Hypertension management is moving away from isolated office measurements toward precision cardiovascular prevention, integrating accurate blood pressure assessment, global cardiovascular risk, intensive lifestyle intervention and individualized pharmacotherapy.
Better blood pressure control is not simply about preventing myocardial infarction or stroke.
It is increasingly recognized as an investment in preserving kidney function, preventing heart failure and reducing cognitive decline throughout life.
Reference 📚
Taler SJ. In the Clinic: Hypertension. Annals of Internal Medicine. Published June 9, 2026. DOI: 10.7326/ANNALS-26-01311.
🚨 The most comprehensive head-to-head comparison of obesity drugs to date just published in The BMJ.
📊 262 randomized trials. 99,791 participants. 19 drugs. Mean weight change vs lifestyle alone at 1 year:
💉 Tirzepatide −14.9%
💉 CagriSema −14.8%
💊 Oral semaglutide −10.9%
💊 Orforglipron −9.9%
💉 Subcutaneous semaglutide −9.8%
💊 Phentermine-topiramate −8.1%
⚖️ Increased GI adverse events across the board.
Increased fatigue was notable most among orforglipron, CagriSema, and naltrexone-bupropion
No meaningful benefits in quality of life metrics were noted.
💉 The pipeline agents ecnoglutide, mazdutide, retatrutide land in the 13–15% range, but the data are early.
🔑 A network meta-analysis is not a substitute for direct comparisons, and cross-trial populations differ.
https://t.co/v2B9ZYCSS9
De hoy, la revisión de Fiebre de Origen Desconocido, de la IDSA (2026). Puntos clave:
🟢 Criterios (ambulatorios): fiebre mayor a 38.3°C en más de 3 ocasiones durante más de 3 semanas, más la confirmación de un set mínimo de pruebas de laboratorio e imagen con resultados negativos o inciertos. Descarta fiebres facticias.
🟢 La causa más común es infección - en Latinoamérica piensa tuberculosis o brucelosis.
🟢 No se recomienda antibióticos empíricos, a menos de que haya hemodinámica, neutropenia, o sospecha clínica de arteritis temporal (para evitar ceguera con esteroides).
🟢 Si no encuentras nada, considera 18FDG-PET/CT - es la herramienta de imagen de elección si está disponible. Tiene rendimiento de 84% a 98%
🟢 Si un abordaje exhaustivo y adecuado no revela la causa, el pronóstico suele ser favorable; la mortalidad es baja y hasta el 75% de los casos se resuelven de forma espontánea con el tiempo.
Léanlo completo (https://t.co/3O93s10Td0).
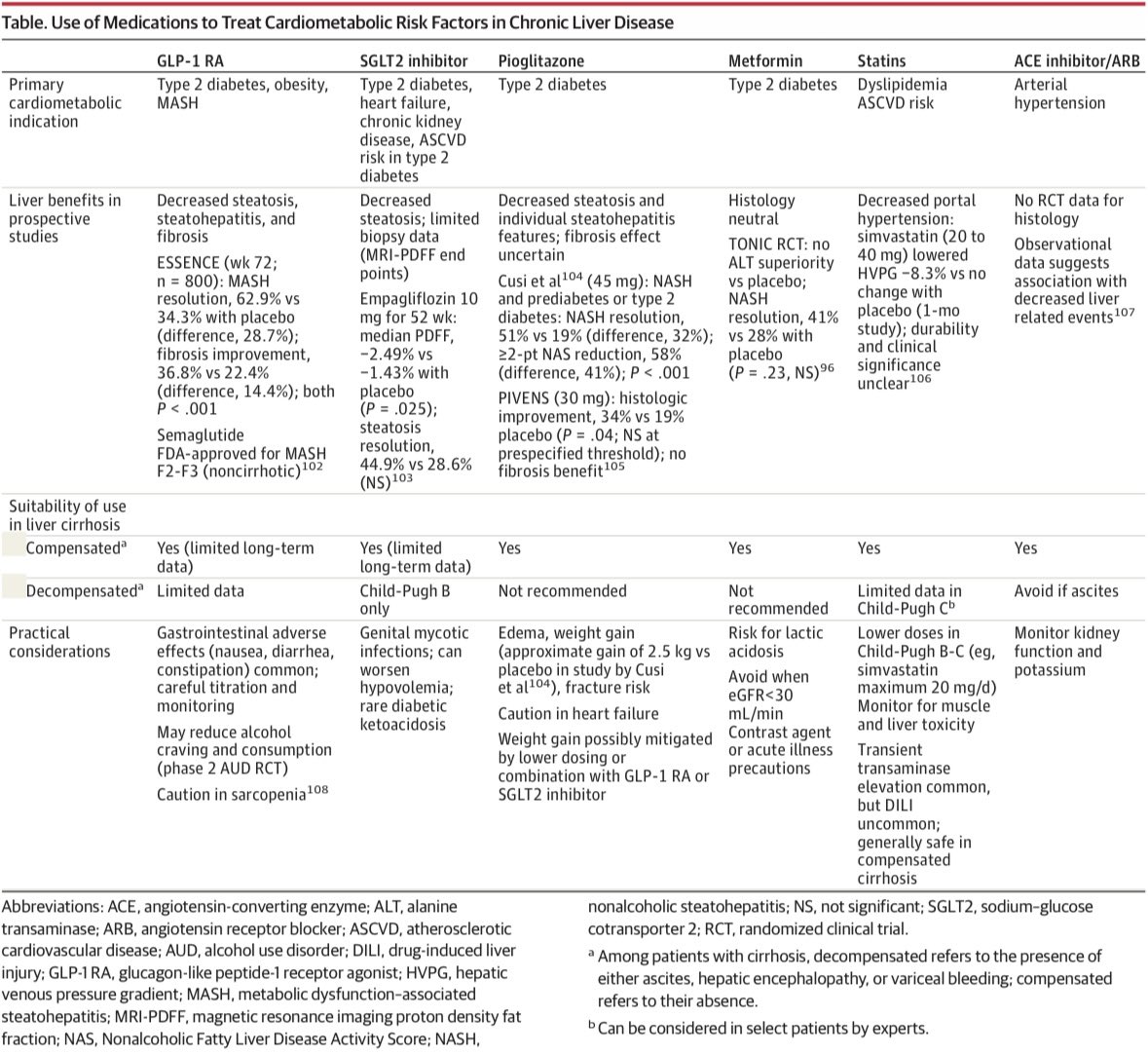
📝 JAMA Review: #AlcoholRelatedLiverDisease is the leading cause of #liver-related #mortality and the most common indication for liver #transplant in Europe and the US, with mortality rates rising over the past two decades.
ALD develops with chronic daily #alcohol consumption (>20 g/d for women, >30 g/d for men) and encompasses reversible #steatosis, #steatohepatitis, #fibrosis, #cirrhosis, and #hepatocellular #carcinoma.
🔗 https://t.co/07xMSfiB7y
🚩¿Vacaciones largas o varias vacaciones cortas?
Un estudio encontró que:
✅ El bienestar alcanza su pico en el día 8.
❌ Más días no aportan grandes beneficios adicionales.
📉 En menos de 7 días tras volver al trabajo, el efecto desaparece.
Por eso, hacer vacaciones más frecuentes podría ser una mejor estrategia para mantener el bienestar.
Multiple sclerosis, a common autoimmune disease of the central nervous system, affects the brain, optic nerves, and spinal cord. Its hallmark effects are inflammation, demyelination, and neurodegeneration. 🔗 https://t.co/McH5l7urUG
In traditional descriptions of the disease, the myelin sheaths surrounding nerve-cell axons are the main target; peripheral nerve myelin, although structurally similar, is unaffected.
The disease typically manifests with discrete focal attacks that affect vision, sensation, strength, and balance, and over time the frequency of attacks decreases and progressive worsening with prominent neuronal injury supervenes (seen in figure). In a minority of patients, symptoms are progressive from onset. Diagnosis rests on clinical criteria and magnetic resonance imaging (MRI) findings, supplemented by clonal expansions of immunoglobulin in cerebrospinal fluid and slowing in central nerve conduction velocities as measured by evoked potentials.
Learn more in the Review Article “Advances in Multiple Sclerosis” by Stephen L. Hauser, MD: https://t.co/McH5l7urUG
Con lesión renal aguda, guiar el manejo de fluidos acorde a POCUS seriados, comparado a lo habitual; fue factible y modificó tratamiento en 50%, pero no mejoró el volumen acumulado, los diuréticos, el empeoramiento renal o mortalidad
Ensayo clínico USE-the-FORCE
CJASN 2026
https://t.co/23l7ASAoxI
Al agrupar los resultados de los estudios FÍGARO, FIDELIO y FIND-CKD el análisis de condensación INFINITY demuestra el beneficio irrefutable de finerenona, al ↓24% el evento renal compuesto
The Lancet 2026
https://t.co/0Acsmm5Hu1