New dad, Dog lover, Radiation Oncologist, Brachytherapist. if you assume my opinions reflect those of my employer, you understand Twitter less than I do.
The #AUA26 advanced prostate cancer guidelines may be some of the clearest evidence of guidelines being influenced by bias and/or industry.
EAU and NCCN recommend with consensus the use of RT to the primary in M1. EAU is “strong” evidence. NCCN is 2A, which is where most RCT data lands. AUA not only gives it grade C, but also conditional. That is where RWD lands usually.
However, darolutamide doublet AUA gives grade A evidence despite only rPFS and no OS benefit. RT to primary showed OS benefit with or without docetaxel and an rPFS benefit with even triplet therapy in peace 1. STOPCAP confirmed robust PFS benefit of RT to primary.
Unfortunate when “guidelines” are ways to push AUA or society members beliefs rather than facts.
Not to mention the radonc on the AUA guidelines is amazing but Zietman is retired.
Was told from AUA guideline authors that this 2026 update didn’t even circulate to all authors 🤔🤔
@ChadTangMD@HimanshuNagarMD@ndesai2005@SbrtSean@Soum_Roy_RadOnc@TylerSbrt@PCaParker@jamesbyu@Prof_Nick_James@NehaVapiwala@fabiomoraesmd@aleberlin2@DrAndrewLoblaw@I_Migowski@DrOmarMian@Alejogom@BobTimmermanMD@ASTRO_org
@DriesDeveltere@JCO_ASCO@RicBertolo 80% of HYPO-RT-PC pt were treated with 3D CRT, an older RT tech. Larger ptv margins were used. The dose/fx and total dose approx. contemporary rt doses, but the tech used does not reflect modern practice. As such the toxicities were higher than seen in modern practice
@seanmmcbride But Sean, did you know that there are 313,000 new cases of prostate cancer diagnosed each year in the US and that the number is expected to rise?
@TonyFelefly@AmarUKishan@LuisAlberto3P Totally agree. We saw improvements in DM with DE-EBRT in RTOG 0126 for IR patients in the absence of ADT. Also seen in early hdr dose esclaation data sets, and Kishan’s work. Stands to reason this would be seen HR patients treated with out ADT with the higher eqd2 regimen.
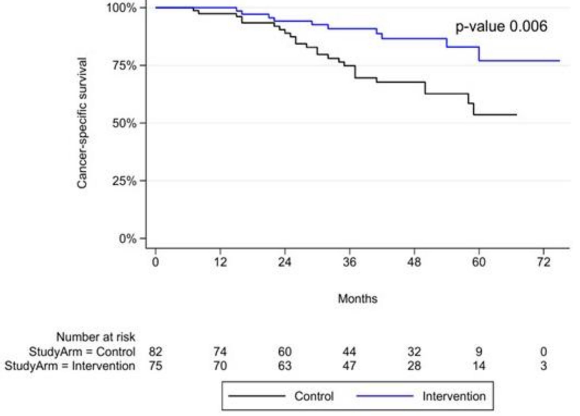
Does the addition of MDT to standard of care continuous ADT improve outcomes for oligomet prostate ca?
Happy to share the results of EXTEND evaluating this question alongside PI @ChadTangMD & many others
X-torial: Cleaning up the misinformation about @JoeBiden and #ProstateCancer that I am reading everywhere.
The purpose of this is to provide education from someone who treats and studies PCa for a living, lead the USA @NCCN PCa guidelines, hold leadership in @NRGonc@theNCI@US_FDA and dedicated my career to help men and their families suffering from PCa
@nytimes@WSJ@FoxNews@CNN@NBCNews@Reuters@ASCO@PCFnews @DeptofDefense
Many agree critical questions remain re: clinical value of treating #ProstateCancer seen only on PET. So let’s get some answers & prove that our treatments help #patients more than they hurt @ZEROCancer@urotoday
CTCAE GU tox G2+ was significantly worse in the two year analysis. Pts should know this. We chose to show tox plots over time as this shows it gets better, which is new information (no diff at 5 years). Cumulative graphs will be in the paper
Rectal Cancer Patients May Not Need Radiation, Study Finds - The New York Times
@nytimes feel free to DM me. As Chair of large Radiation Onc Department I would be happy to inform you of danger of the article for pts.
Easy fix. Worth it to fix. https://t.co/t1qrOVkHue
@alison_tree@Simon_Spohn This. Always wondered: MD1 gives flomax at low threshold - happier Pt but gr2 ctcae. MD2 gives less; Pt qol worse but gr1 ctcae. Which is the worse outcome? Composite endpoint of gr2 plus mcid needed? Phenomenal work once again!
A recent study indicated a 1.2% ⬆️ risk of second primary cancers among men treated with radiation therapy vs. surgery for prostate cancer. Background smoking history remained unaccounted for, so we posted a comment asking the authors to clarify. #radonc https://t.co/sz4kGvjDKZ
@SbrtSean Cefpodoxime or levaquin starting the day prior to the procedure and one day after. I hold anti-platelets/anti-coagulants aside from Aspirin 81mg. If patient is on warfarin, I ask for an INR the night before or the morning of the procedure. Goal <1.4
Over the last 3 years, we have had several communications detailing the mission of the ABS and the #300in10 initiative. We are happy to announce that we have 4 training sites that are now taking applications. https://t.co/3xtQncQ5o4 @daniel_petereit#ThisIsBrachytherapy#brachy
Thought provoking presentation by Dr. Steven Chmura at #ACRO22 on SBRT on oligomet. Tox from high-dose SBRT can happen late (BR001); no meaningful improvement in PFS in BR002 seen —>unlikely to proceed to phase III; and bell-shape curve of the utility of local therapy.