1/Having trouble remembering how to differentiate dementias on imaging?
Is looking at dementia PET scans one of your PET peeves?
Here’s a thread to show you how to remember the imaging findings in dementia & never forget!
Stuck between a rock & a hard place when it comes to brain calcifications?!
Calcification pattern is key to rocking the diagnosis!
Here's a quick guide to the most common entities associated w/different patterns
For the three most common patterns, I remember what you do when ROCK music plays:
I HeaR = Infection & Hematoma give a Rock pattern
I GYRate = Infarct give a GYRiform
And finally...
I Dab = Infection gives tiny Dabs or Dots everywhere
For the rest:
If they are grouped: think tumor or vascular
If they are diffusion: think metabolic
If they are along the ventricle: think TORCH
Now hopefully you can rock & roll when it comes to the diagnoses for intracranial calcifications!
Feeling bipolar about bilateral thalamic lesions?
Unfortunately, the differential for bilateral thalamic lesions isn’t binary!
But here’s an easy mnemonic to help: THALAMIC!
T = Tumor (glioma)
H = Hypoxic/ischemic encephalopathy
A = Artery of Percheron Infarct
L = Loss of thiamine (Wernicke’s)
A = ADEM
M = Metabolic/Toxic
I = Internal cerebral vein thrombosis. Infection (west nile)
C = Creutzfeld-Jacob
Now you’ll never bypass a bilateral thalamic diagnosis with this easy mnemonic!
1/Do radiologists sound like they are speaking a different language when they talk about MRI?
T1 shortening what? T2 prolongation who?
Here’s a translation w/an introductory thread to MRI.
Have MULTIPLE questions about MULTIPLE sclerosis?
Having trouble seeing neuromyelitis optica?
In a fog about MOG?
Here’s the cheat sheet you NEED to distinguish the demyelinating diseases!
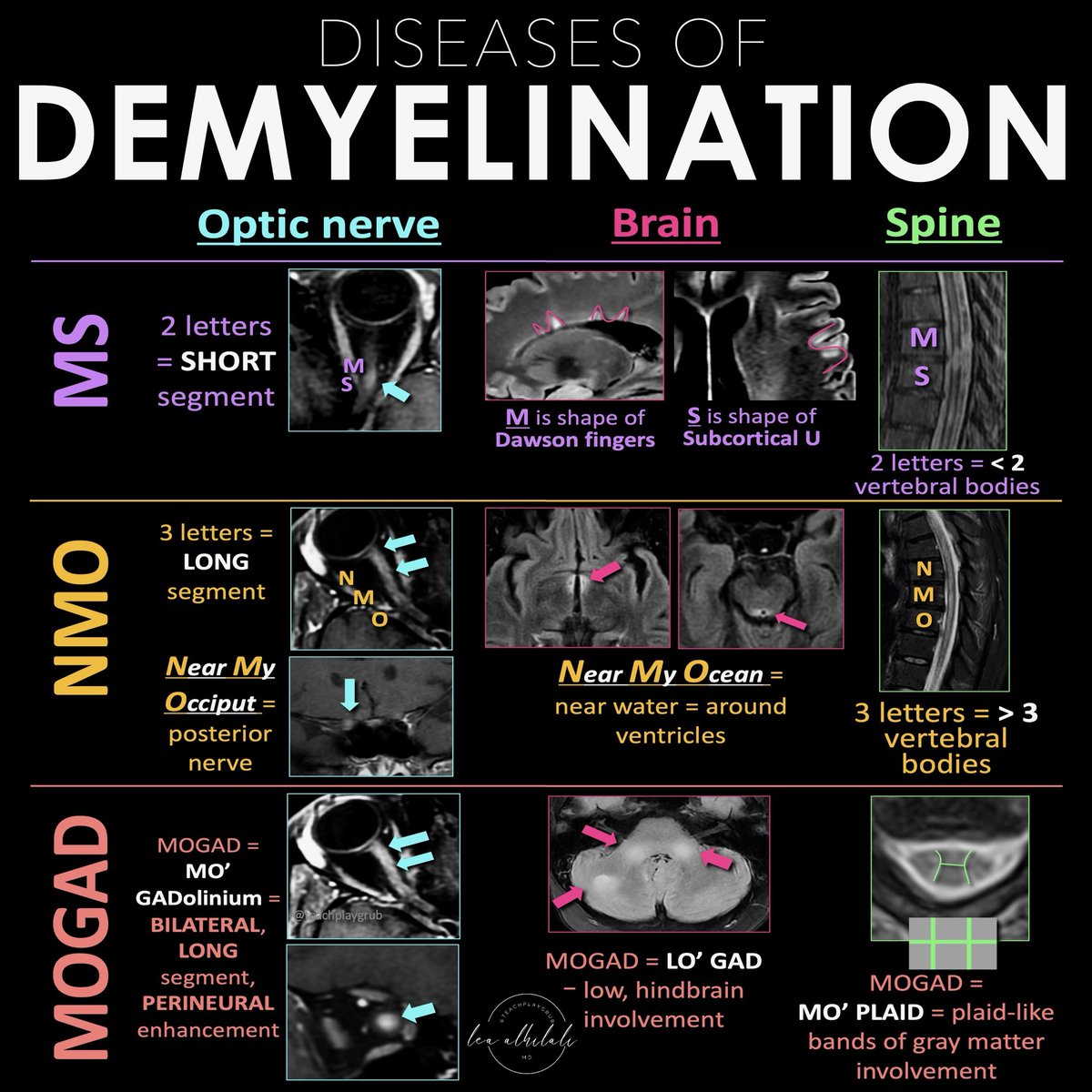
Demyelinating diseases predominantly involve the optic nerves, brain, & spine.
The three main chronic demyelinating diseases are Multiple sclerosis (most common), neuromyelitis optica (NMO), & myelin oligodendrocyte glycoprotein (MOG) antibody associated disease or MOGAD
Each has its own features in the optic nerve, brain, & spine. Here’s how to remember them!
MS
Optic nerve:
MS only has 2 letters, so MS involvement of the optic nerve tends to be short segment
Brain:
Letter M makes the shape of the perivascular distribution of lesions along the ventricles (Dawson’s fingers)
Letter S makes the shape of the subcortical U fiber involvement
Spine:
MS is only 2 letters, so lesions are usually less than 2 vertebral bodies in length
NMO
Optic nerve:
NMO is a longer abbreviation, three letters, so longer involvement
NMO can stand for Near My Occiput. Occiput is posterior, so more posterior nerve involvement
Brain:
NMO can stand for Near My Ocean. What is your brain’s ocean? The ventricles. NMO lesions are all periventricular
Spine:
NMO is 3 letters, so lesions usually more than 3 vertebral bodies in length
MOGAD
Optic Nerve:
Remember MO’ GAD-olinium. So things that cause more regions of enhancement. MOGAD lesions are commonly bilateral & long segment & enhancement can extend perineural
Brain:
Remember LO’ GAD. MOGAD typically involves the lower areas of the brain
Spine:
Remember MO’ PLAID. MOGAD can give a plaid-like H shape in the cord from predominantly gray matter involvement
Hopefully, this cheat sheet will help you remember how to distinguish the demyelinating diseases! It ain’t lyin’ about diseases of myelin!
Can't remember the types of craniotomies off the top of your head?
Do you need another thing to memorize like you need a hole in your head?
Here's a quick figure with a review of some common craniotomies to help you out!
Let’s dig deeper into these holes!
Frontal: For large midline anterior and sometimes middle skull base lesions
Temporal: For middle cranial fossa lesions, including intra-axial lesions in the mesial temporal lobe
Parietal: For mid to posterior cerebral hemisphere lesions while sparing the motor and sensory cortices.
Parietal interhemispheric approach for parafalcine, medial parietal, and splenial lesions. Parietal transcortical route for intra-axial lesions through the functionally “silent” superior parietal lobule
Pterional (frontotemporal): Access to the frontal lobe, temporal lobe, and Sylvian fissure and allow for direct visualization of the microvasculature surrounding lesions in the suprasellar cistern
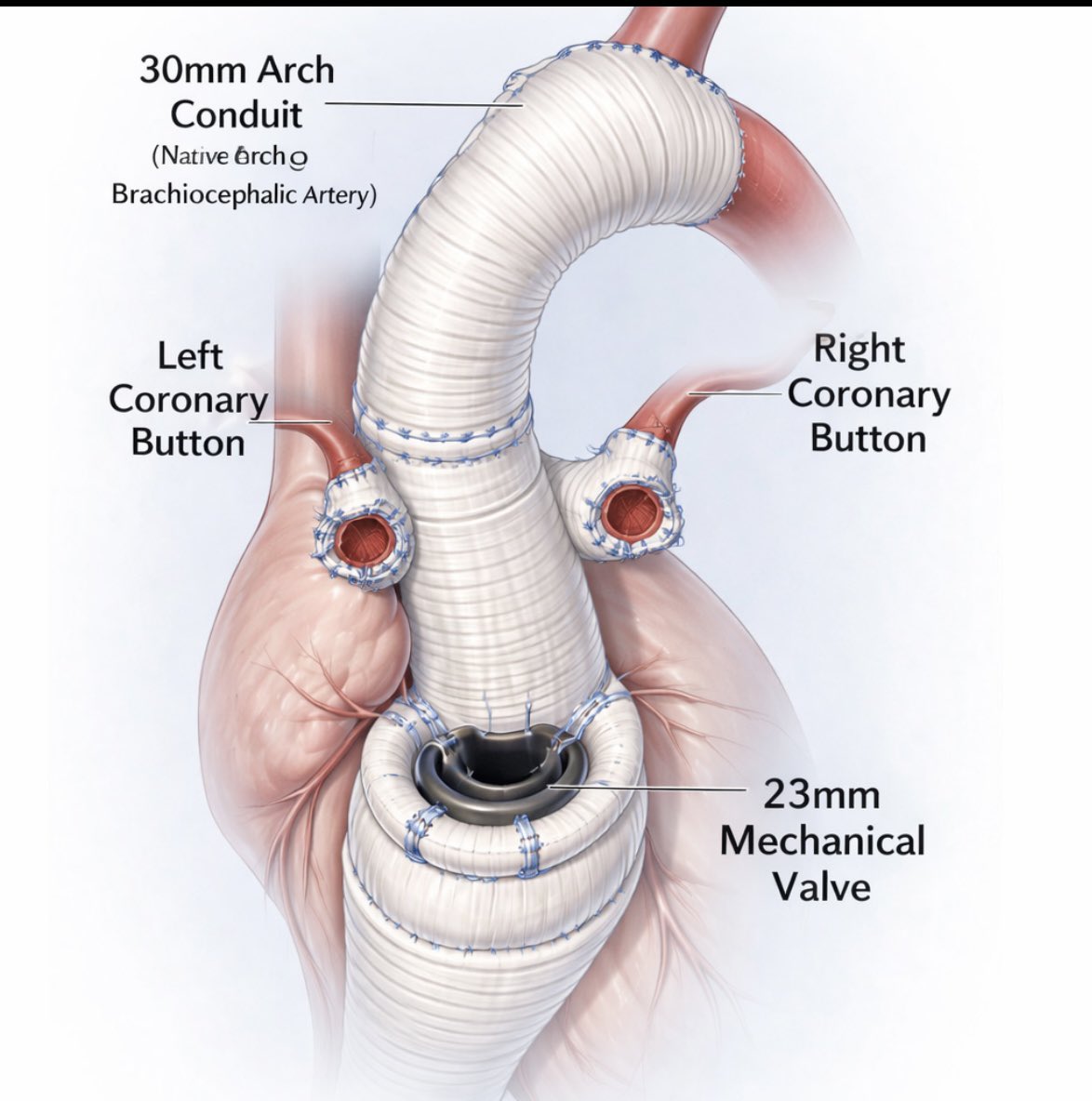
The Cardiac Center of Ethiopia successfully performed its first redo Bentall procedure with hemiarch replacement in a 14-hour long cardiac surgery. The procedure was carried out by a local cardiac team led by Dr. Fekede Agwar in a 25-year-old male patient.
🌍Live from IPNTN Season VII, Session 1🌍
Head and Neck Pathologies, Take 5! with @amyfjuliano
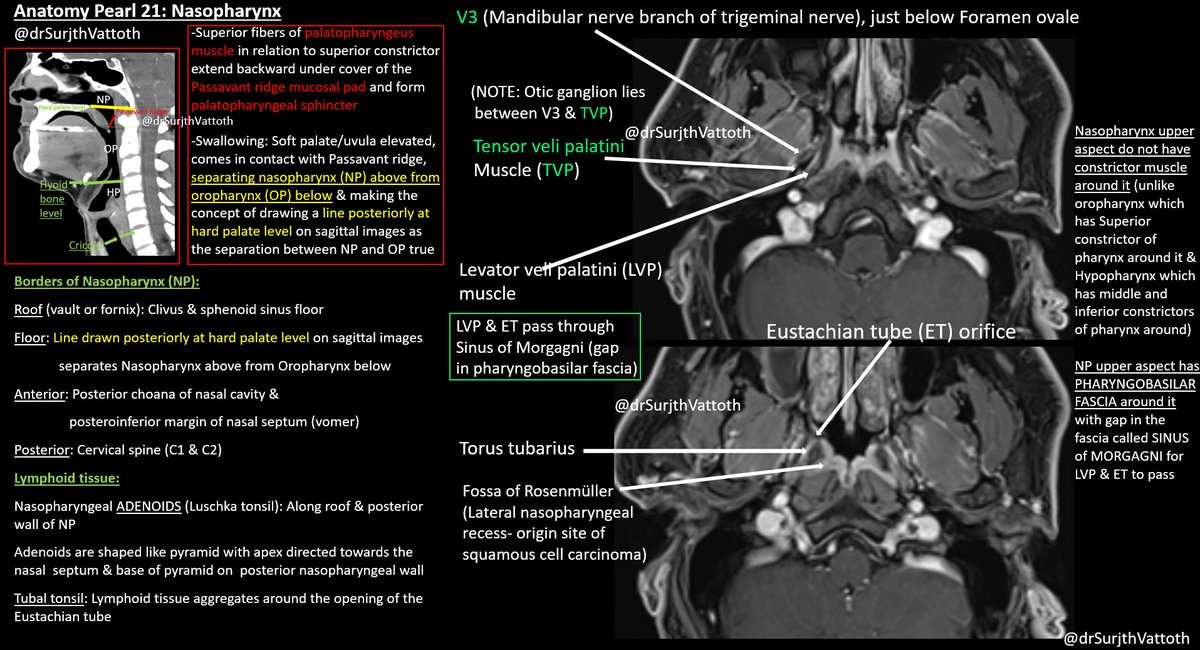
💡Think carefully about the wording of reports! Mastoiditis is a clinical diagnosis, coalescent mastoiditis and other complications of mastoiditis should be assessed by imaging. And remember, not all mastoid opacification is infectious.
Our study "The Rise of Deepfake Medical Imaging: Radiologists’ Diagnostic Accuracy in Detecting ChatGPT-generated Radiographs" was just published in Radiology!
https://t.co/9OGKsxn1Rc
Test yourself to differentiate ChatGPT-generated from real radiographs: https://t.co/uie4Eiw1LN
🍤The “shrimp sign” describes a cerebellar MRI pattern of progressive multifocal leukoencephalopathy
💡T2/FLAIR hyperintense white matter lesion that hugs but spares the dentate nucleus, giving it a shrimp-like shape
🧠It is thought to result from JC virus-driven demyelination
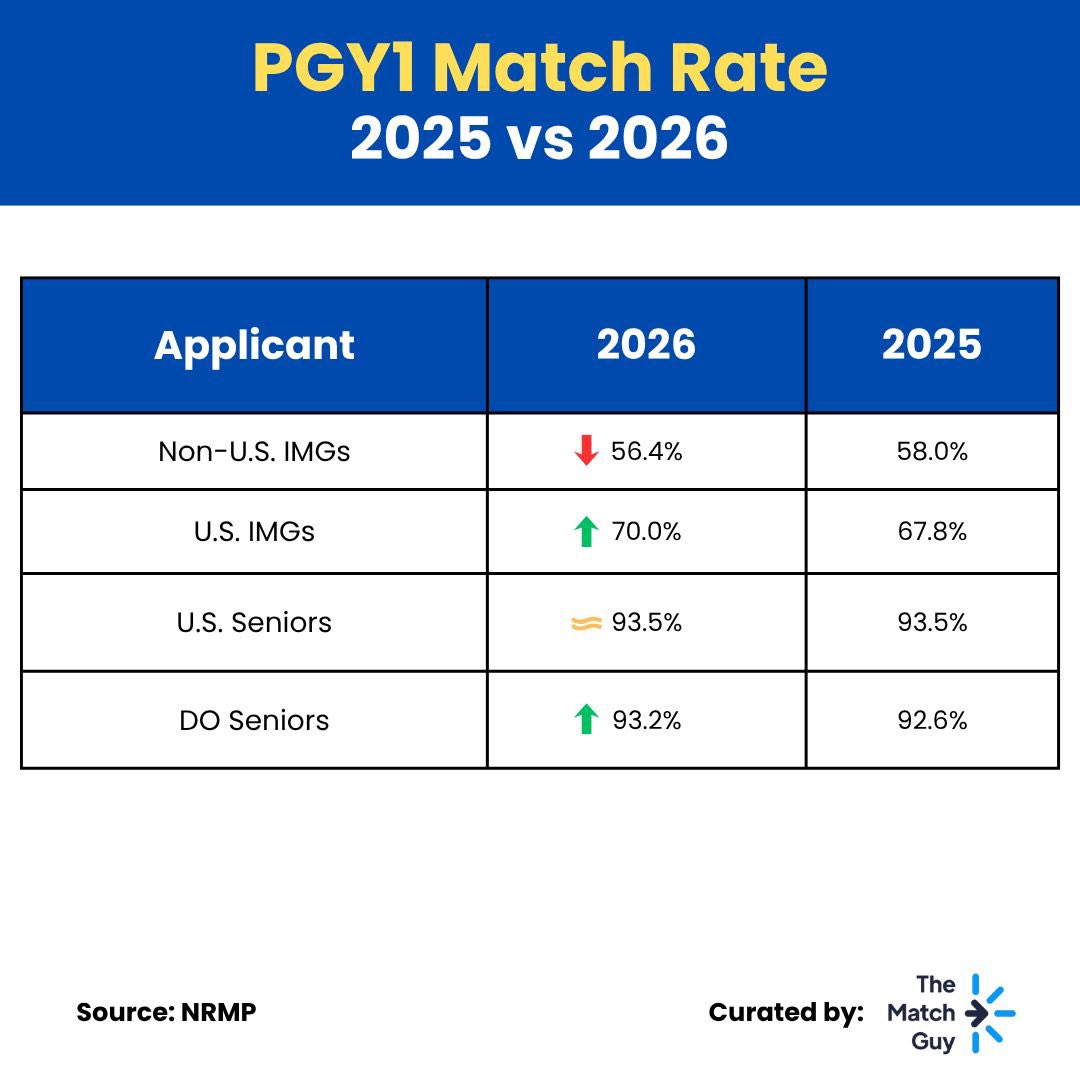
📉 Non-U.S. IMGs saw the biggest drop this year, with the lowest match rates in the past five years (2022–2026), likely driven by ongoing visa concerns.
Meanwhile, U.S. IMGs and DO seniors achieved their highest match rates in the past five years. This shift may partly reflect programs favoring applicants who do not require visa sponsorship, potentially at the expense of non-U.S. IMGs who historically filled some of those positions.
Read more below 👇