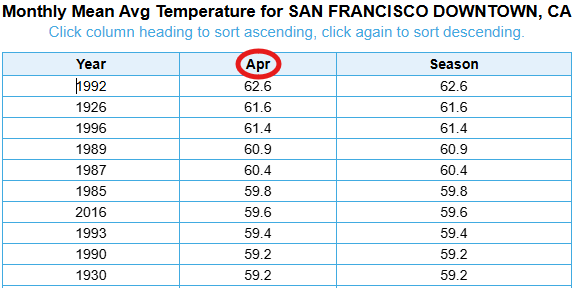
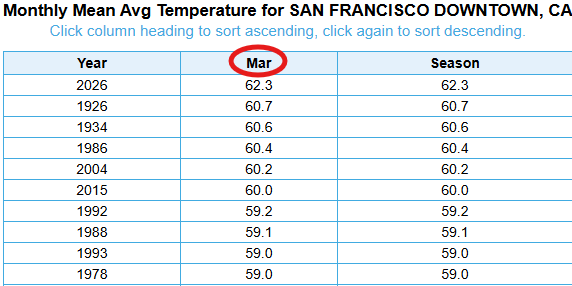
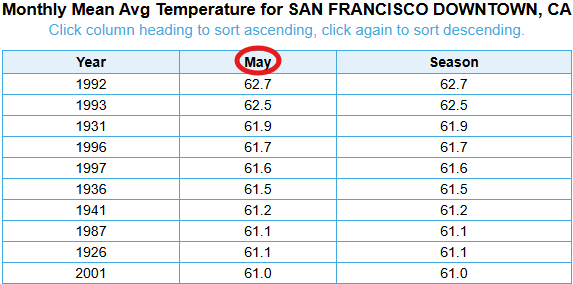
With only a few days left in March, this will undoubtedly be the warmest March on record for our area. To put in perspective just how impressive the heat was this month - it would be the 2nd warmest April on record, & 3rd warmest May! Cooler temps are on the way this week. #CAwx
Do you wonder why there are so few *serious* studies on COVID interventions?
The answer lies in how studies are reviewed.
1) Crony Studies. Sometimes a big monopoly is in charge of a lot of the funding. The people in charge of it are at "elite" universities and either have an impressive scientific history, or are small-p politically connected (mentees, collaborators) of those who do, sometimes almost no accomplishments to date. They may have had little to no vested interest in COVID as a grand-scale public health problem at any point, and often rarely after March 2022. They don't mask because they don't care about COVID much at all, and much less than other health issues. They have very little interest in what pwLC have to say. Since they don't view COVID as a serious problem, they devote little effort into trial design or even understanding basic issues like biomarkers, plausible mechanisms, or how to diagnose Long COVID in any reasonable way. There is very little oversight and no meaningful external review of said studies to determine whether they are worthwhile or how they should be improved to use funds responsibly. The studies inevitably fail. These studies should be high-risk, high-reward, so it's not all on them, but it seems like they are disproportionately set to fail.
2) Rigorous Science. Often, people submit rigorous studies to standard funders, where they undergo rigorous external review. What that looks like is that 2-5 reviewers read, score, and critique each application in detail, and then a larger group (who reviewed various other application on all sorts of topics) discuss each application, everyone scores them, and the top apps are funded. The problem is that just about any one of the 5 main reviewers can tank an application by giving it a bad score. Moreover, to get funded, an application needs a pretty good score from basically all 5 reviewers. If one reviewer is delusional (COVID is "over," etc.), the application will tank, and it's very rare to get 5 reviewers enthusiastic about COVID research. To be enthusiastic would mean admitting the scope of the problem, that they have made serious personal mistakes, that family members or co-workers or people in the community are dead or disabled because of their behavior, etc. Keep in mind, lots of lower-impact rare disease research with minimal quality-of-life impact commonly gets funded (good, fund it all!), so funding rigorous COVID research should not be a big deal, except people struggle to acknowledge it is even a small problem in 2026. Nobody can acknowledge COVID as a small problem, because it's a gigantic problem, and saying it's a gigantic problem mean people acknowledging many mistakes with mortal consequences.
3) Chuckle Studies. Often, people have no theoretical framework, no understanding of mechanisms, apathy toward scientific training. They submit "chuckle studies" testing whether random intervention X has any benefit in random population A. It could be a random supplement, nasal sprays, neti pots, magnet hats, yoga cures, whatever. These studies will often get rejected. BUT the interventions are arbitrary, so the scientists can submit a LOT of these types of applications. Often, there will be industry funding to prop these up to get them going, running pilots and paying for scientists' time so they can submit lots of funding apps. Just replace intervention X with intervention Y, population A with population B, and keep throwing spaghetti at the wall. There's no theoretical framework (sometimes celebrated as "it's a mystery"), no real supporting literature (maybe 1-3 deeply flawed studies), so easy to update the application. Do this enough, and it will get favorable peer review. The delusional peer reviewers will love it, because it poses no threat to their delusion (COVID as a non-issue). It lets the reviewer keep the mindset that COVID is a joke and warrants a joke solution. Everybody chuckles while they keep getting reinfected.
The end consequence is a lot of crony and chuckle studies, and various little rigorous research. A lot of us are fighting to push through rigorous studies, but it's an extremely uphill battle, and too few of us. Most of us who take COVID seriously are not in pharma. Lots of engineers, behavioral scientists, epidemiologists, etc. It's more of the prevention and population science lens. We can do helpful things to push forward the research agenda, but even that's against all these obstacles. The obstacles apply to manuscript reviews too, so often the rigorous pilot behavior, engineering, or epi work can't get published, and so the grant apps are weaker for that too. There are very few people doing pharma research from a serious COVID aware perspective. Sisyphus backed out, more content with his day job.
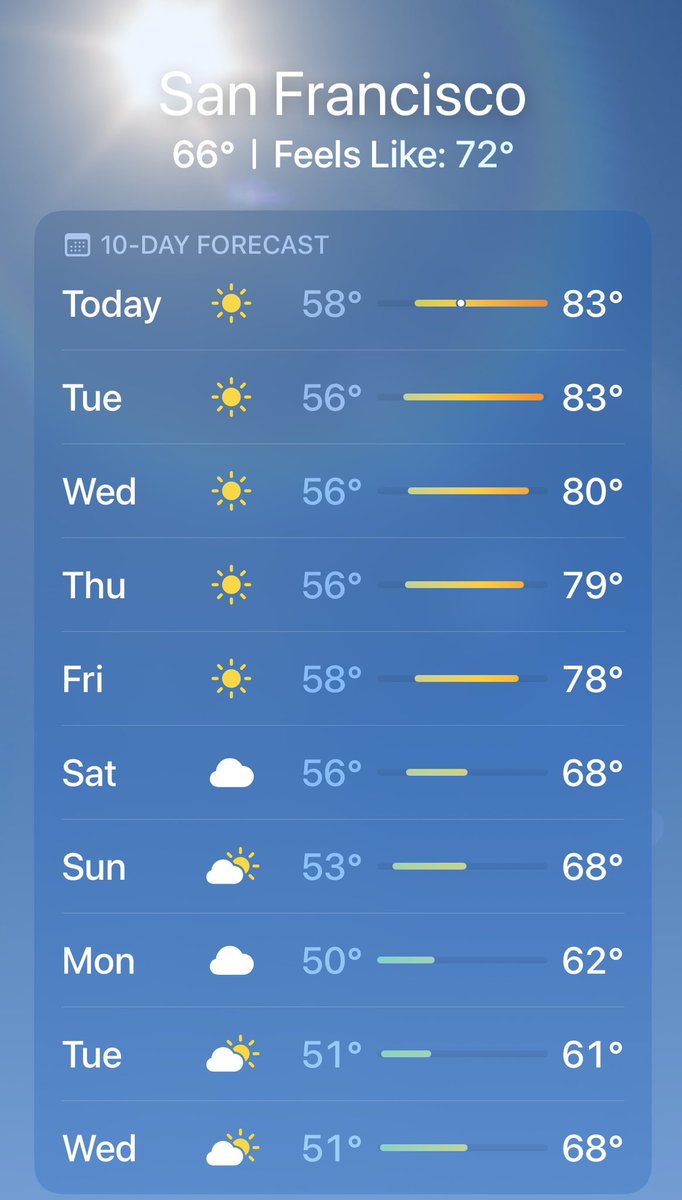
The Weather App on your iPhone is awful (sorry, Apple).
I’ve seen tons of screenshots of the upcoming heatwave forecast, and the Weather App is off by up to 5-10 degrees. National Weather Service forecasts are the most accurate source, but unfortunately its website looks like it was built in 2003. @EverythingWX (not an ad) is the only app I know of that displays NWS forecasts in a great user interface.
If you are wondering why the Weather App’s forecasts are so inaccurate, it’s because it only uses select raw weather data without any trained meteorologists reviewing it. There are over 120 NWS offices across the US that issue fantastic forecasts using far more models and tools, with real humans reviewing the data.
Take the Weather App’s forecast for San Francisco, it’s only forecasting a high of 83°F on Tuesday, while the NWS is forecasting 88°F.
The NWS also uses a point forecast system where each grid square covers a 2.5 km × 2.5 km area, which more accurately captures microclimates, perfect for a city like San Francisco.
Use the NWS forecast this week and ditch the Weather App.
4/ That morning, my patient had been at the beach with friends. By afternoon, he felt suddenly unwell — fevers, chills, a sense that something was very wrong. He lost consciousness, and someone called 911. He survived, but only after weeks in the ICU. He left the hospital with bilateral below-knee amputations and extensive scarring.
The meningococcal vaccine just got moved to "shared clinical decision-making" on the new CDC schedule. This is one of the infections I feared most during my training. Here's what it is, why it's often confused with "meningitis," and what this policy shift will mean in practice. 🧵
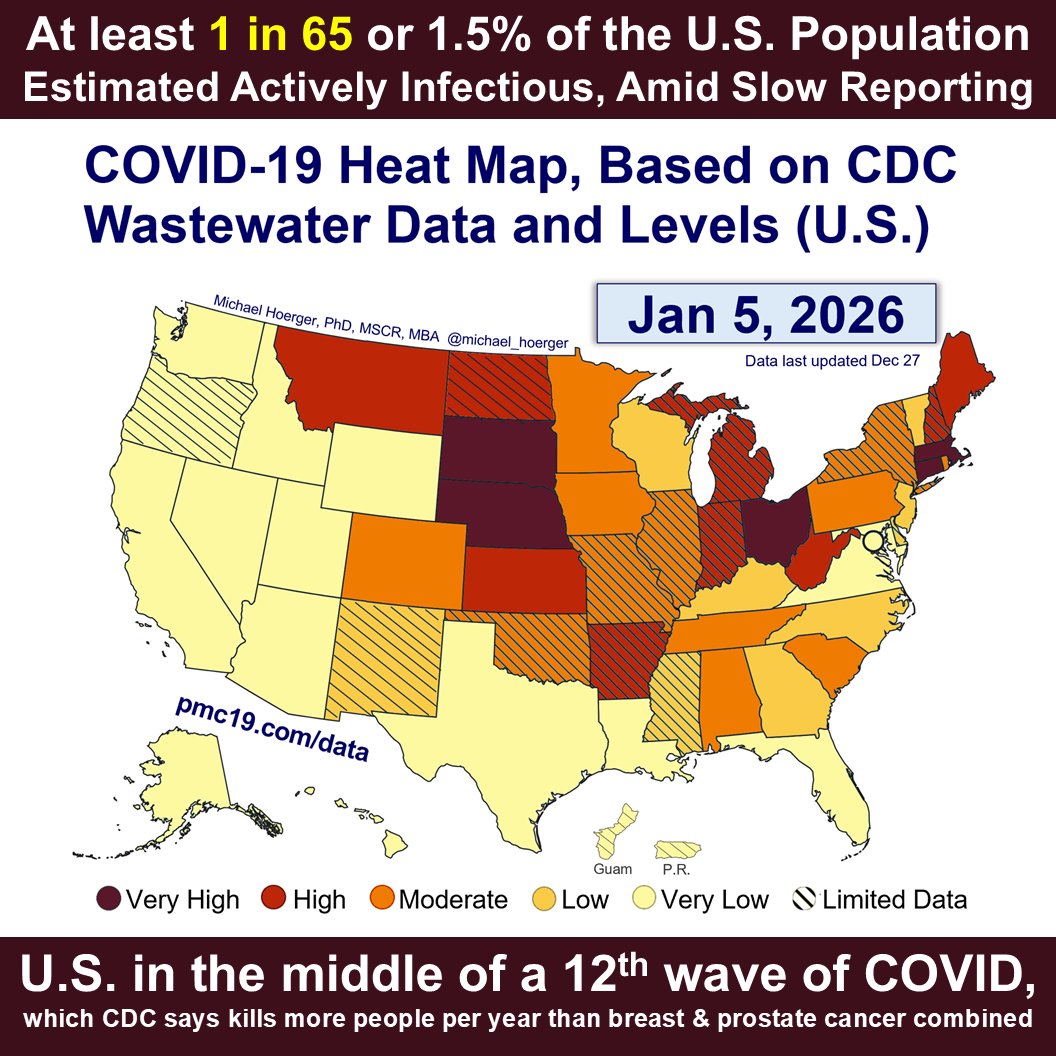
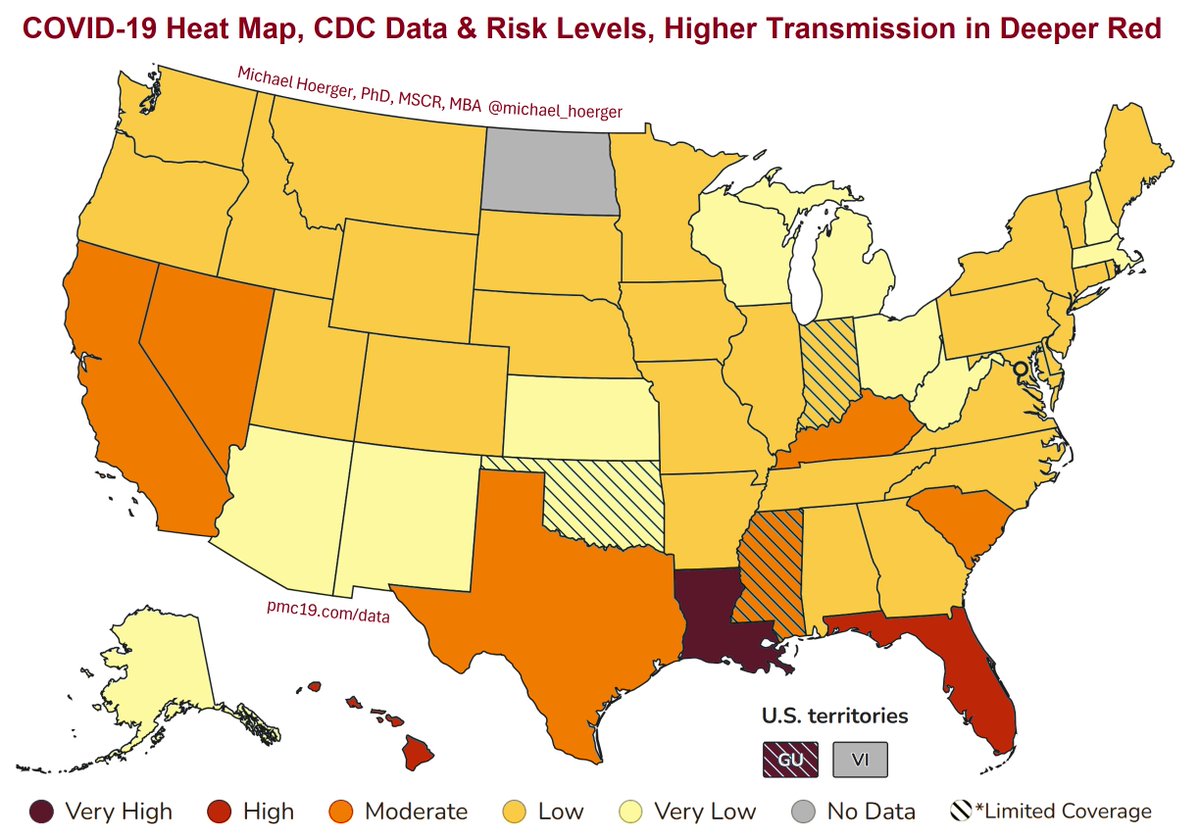
We're in the middle of a 12th COVlD wave in the U.S., with transmission particularly high in the Midwest and Northeast.
The CDC announced this week that COVlD continues to kill more Americans than breast and prostate cancer combined.
Get boosted & #MaskUp 💉💪😷
1/4🧵
🔴 Gaza’s health system is nearing total collapse, the Health Ministry warns, citing catastrophic shortages after two years of war and siege.
👉 The ministry says Israel is allowing less than 30% of needed medical aid trucks to enter Gaza and is calling for immediate international intervention to prevent full system collapse and mass loss of life.
▪️ Medicines: 321 essential drugs are completely out of stock (52% shortage).
▪️ Medical supplies: 710 items unavailable (71% shortage).
▪️ Labs & blood banks: 59% of essential tests unavailable.
▪️ Emergency & ICU: 38% shortfall, risking denial of care to 200,000 emergency patients, 100,000 surgical patients, and 700 ICU patients.
▪️ Dialysis: 650 patients affected, needing 7,823 sessions/month.
▪️ Cancer care: 70% of oncology drugs unavailable. 1,000 patients deprived of treatment. Some have already died. Even palliative pain relief is unavailable.
▪️ Primary care: 62% of medicines missing, placing 288,208 patients at risk of strokes and heart attacks with no treatment available.
▪️ Cardiac care: Cardiac catheterization and open-heart surgery completely halted.
▪️ Orthopedics: 99% of scheduled surgeries stopped.
▪️ Eye care: Specialized surgeries near shutdown. Basic exam drugs unavailable.
▪️ Labs: Life-saving tests like CBCs, electrolytes, blood typing, and cultures unavailable.
On the final, eighth night of Hanukkah, we honored the memory of our beloved Shatzi Weisberger (@peoplesbubbie) (1930-2022), Z’’L. Shatzi was a proud anti-Zionist, lesbian, activist, nurse, death educator, New Yorker, and member of JVP. 🧵
I can’t emphasize enough how much accessibility benefits everyone. Ramps, elevators, ventilated air, automatic doors. You caring about accessibility is caring about your future. You will become disabled unless you die young. Investing in disability is investing in yourself.
They have fired the staff of the CDC’s Morbidity and Mortality Weekly Report and 70 Epidemic Intelligence Service officers, who are disease detectives that respond to outbreaks.
I cannot emphasize enough how dangerous it is to dismantle our disease surveillance infrastructure.
Another horrifying loss of an @MSF colleague in #Gaza.
Omar Hayek was an occupational therapist. Other colleagues injured include a physiotherapist, and an orthopaedic surgeon among others.
I mention their professions because I spoke earlier today of the urgent need for this specialised care for the thousands of injured Gazans.
Every loss of a medical worker is a tragedy for their families, colleagues, and the people they will never be able to help.
Over the past two years, @WHO has verified over 1700 attacks on health care in Gaza and the West Bank, resulting in more than 1000 deaths and 1800 injuries.
The attacks on health MUST STOP. Ceasefire!
The point of vaccine mandates is herd immunity and protection of the people who actually cannot get vaccines. It seems tragic that the health officials in Florida cannot understand this.
🔥 95% of wildfires are caused by people.
That means almost every fire that has threatened communities could have been prevented.
Whether you're using equipment, towing a trailer, burning debris, or building a campfire—one mistake can spark disaster.
Help us reduce the risk:
🚫 Use spark arresters
🚗Check for dragging chains
🔥 Never leave fires unattended
♻ Burn only when and where it’s safe
One less spark = one less wildfire. Let’s all do our part.
#OneLessSpark #WildfirePrevention #CALFIRE #FireSafety #PreventWildfires #ReadyForWildfire
Dramatic changes to the Vaccine Injury Compensation Program could drive drugmakers from the market, threatening access to shots, experts say.
“If (Kennedy’s) unstated goal is to basically destroy the vaccine industry, that could do it.”
https://t.co/FfEiYl11jI