Glomerular crescents 🌙
❓What’s a crescent?
🔬Crescentic GN?
🧩 How are crescents formed?
🔬🗂 Types of crescents? ❗️Pseudo-crescents?
(1/6)
#renalpath#PathResidents#Pathbracket
BK virus infecting podocytes in a case of BK nephropathy. BK usually infects tubular epithelial cells and rarely parietal epithelial cells, podocyte involvement has not been described before.
https://t.co/YSS7h1QjVK
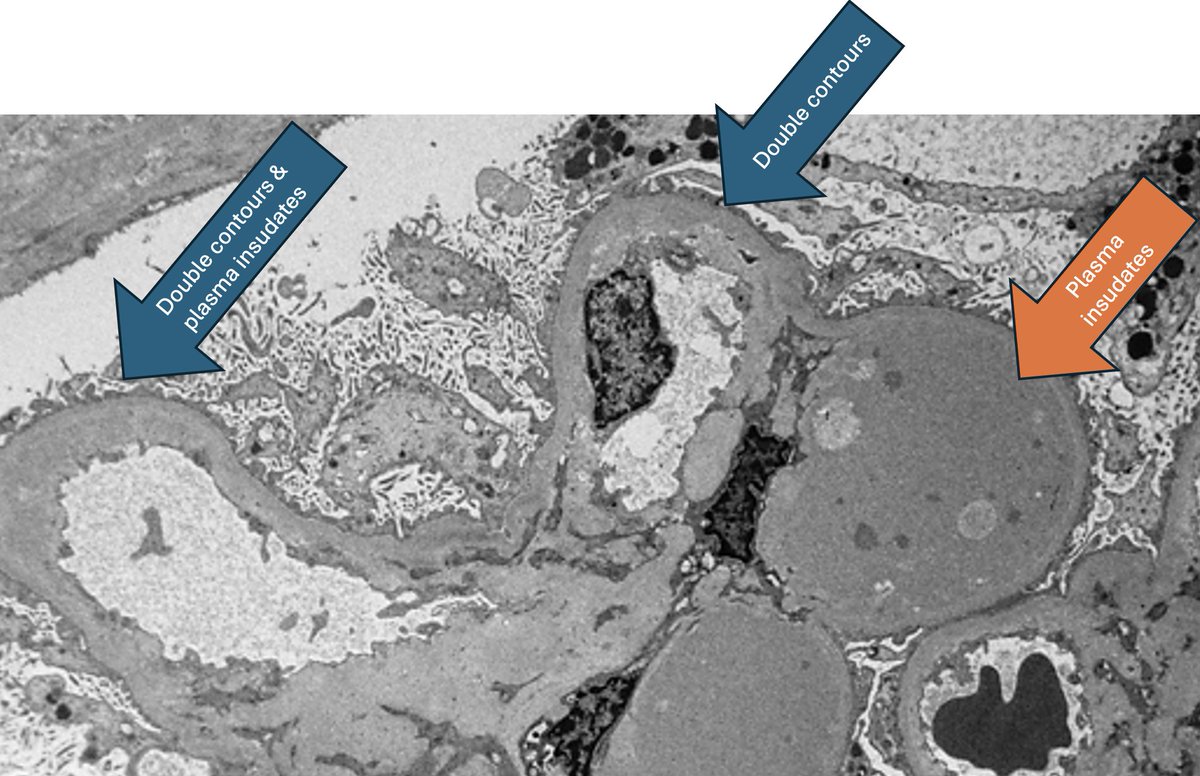
Overlap of C3GN and TMA (aHUS).
Both are complement-mediated diseases.
The study is the 1st to show overlap of C3GN-TMA findings in C3GN.
TMA findings are present on electron microscopy & maybe missed.
The lesions are often C3GN-dominant or TMA-dominant.
https://t.co/oZXxywGMKm
🔬 Spiculated intratubular casts on silver stain, Congo red positivity, and apple-green birefringence point to amyloid cast nephropathy. Paraffin IF confirmed kappa restriction despite negative routine IF.
#RenalPathology#KidneyBiopsy#Amyloidosis#NephPath
Renal Pathology Society's Case in Focus
Middle-aged male with HTN & CKD presented with nephrotic range proteinuria
Rita Santarsiere & Nicolas Kozakowski
English: https://t.co/7LFCD7VgNC
Links to translations (Spanish, Portuguese, French, Chinese) in next post below
#renalpath
Finding the etiology of membranoproliferative glomerulonephritis https://t.co/OHHlnZPmGT
My review of evaluation of MPGN on kidney biopsy is out.
Take home messages:
1. Idiopathic/primary immune complex (IC)-MPGN is very rare.
2. Careful evaluation of IC-MPGN will invariably reveal the etiology. Always rule out monoclonal Ig.
3. Beware of entrapment of Ig in cases of C3GN, as you might label these as IC-MPGN.
4. Consider infection related GN in cases of C3GN, even if IC is sparse/absent, in the right clinical scenario.
Here is today’s #eyeSCANdy! Acellular scanning EM showing a glomerulus with ischemic collapse.
Photo courtesy of Dr. Stephen Bonsib. #renal#pathology#kidneypath
Want to learn about the role of the Complement System in the pathogenesis of Glomerular Diseases? 📆Mark your calendars: Friday, May 8, in the time zones below ⬇️ as Dr. Abdallah Geara - a phenomenal educator and expert in GN and Onconephrology, delivers a presentation on this timely topic, moderated by @alanephro
Join meeting here:
https://t.co/5GM9sjJOJ4
Meeting ID: 884 4208 1901
Passcode: 100499
Visit us 👉https://t.co/my949rApI6
@glomconarabia@GlomCon@PennGlomCTR
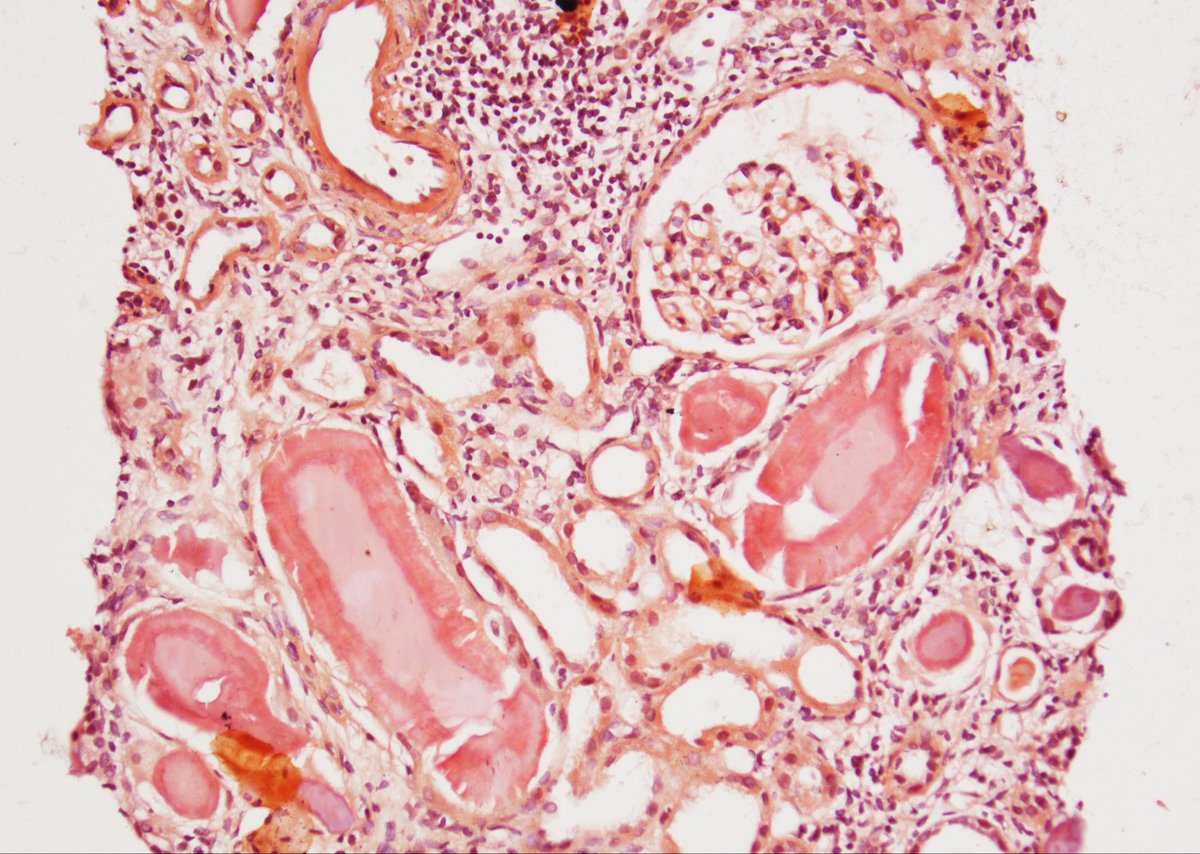
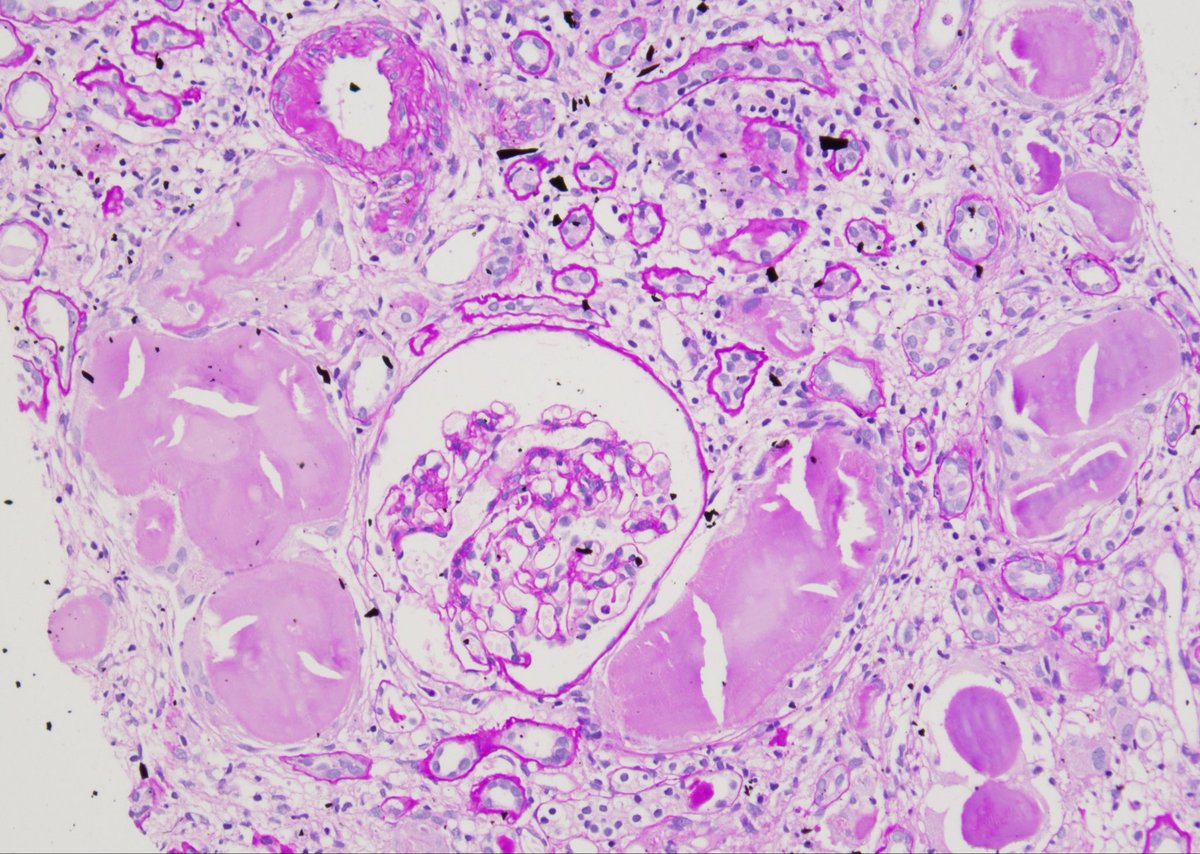
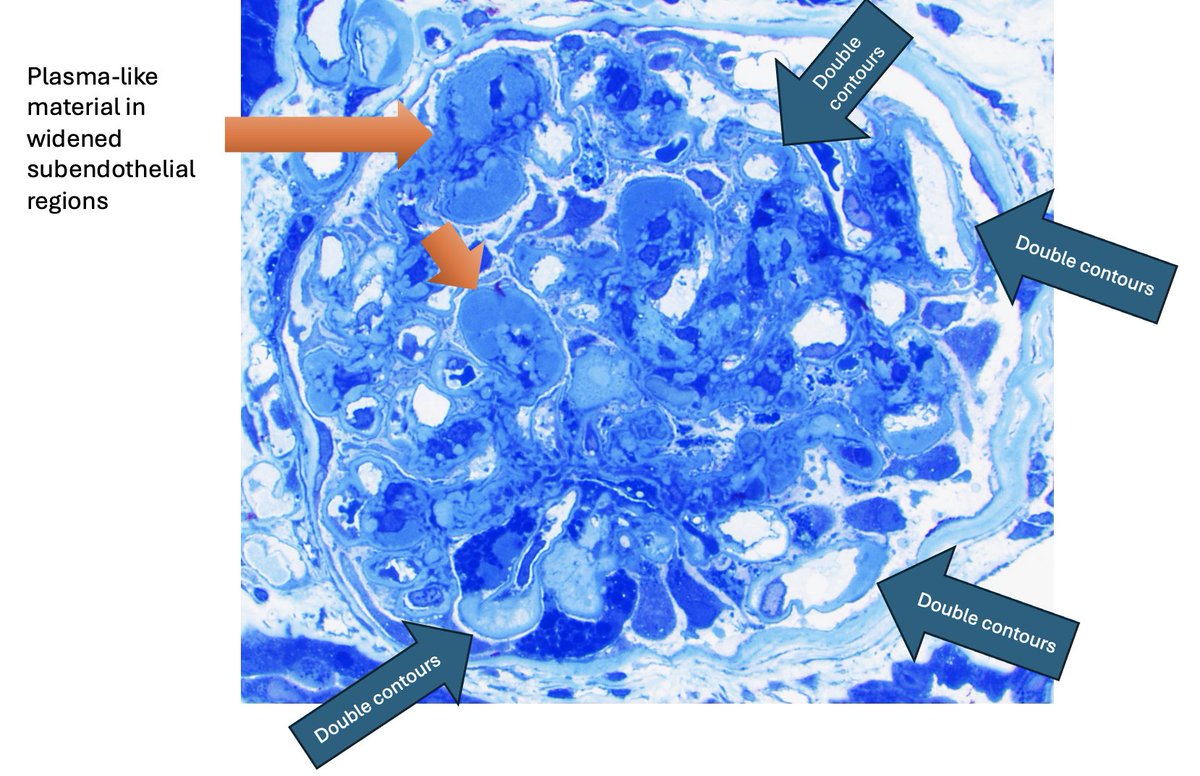
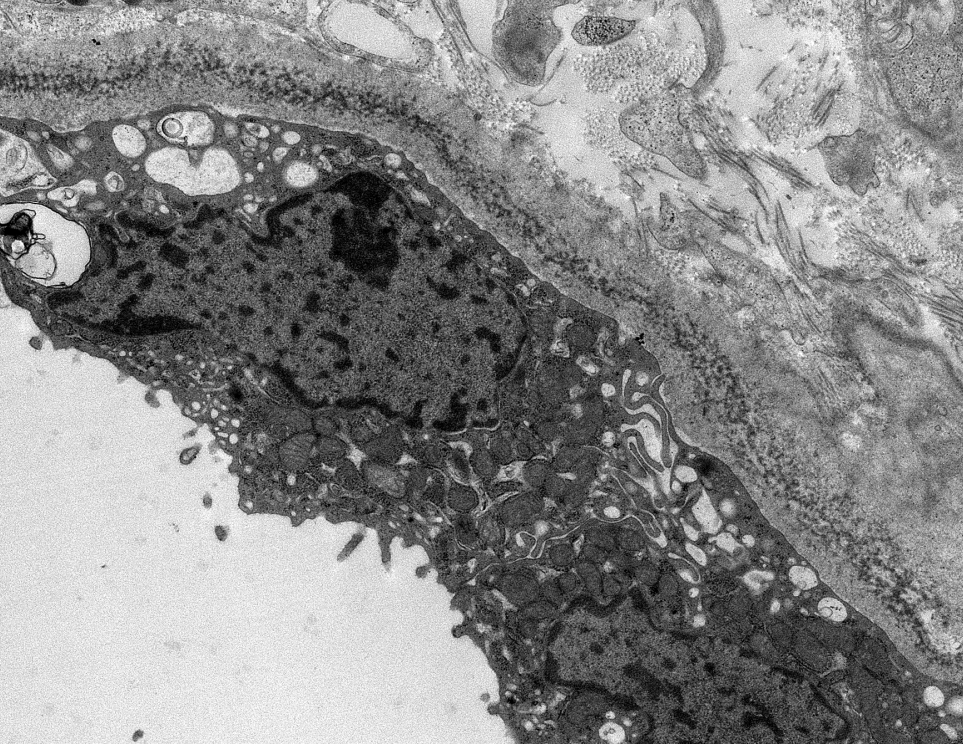
This biopsy was taken from an older adult man with acute kidney injury and non-nephrotic range proteinuria. His medical history included metastatic colonic adenocarcinoma, for which he was taking bevacizumab, an anti-vascular endothelial growth factor (anti-VEGF) inhibitor. The sampled glomeruli show changes of thrombotic microangiopathy (TMA), including double contour formation of glomerular capillaries (Fig. 1) and intracapillary red blood cell fragmentation (Fig. 2). TMA is one of the most common adverse effects in the kidney of bevacizumab therapy, and it has been reported as early as one week after starting the drug. Other pathologies reported in the setting of anti-VEGF treatment include focal segmental glomerulosclerosis (FSGS), collapsing glomerulopathy, and immune complex-mediated proliferative glomerulonephritis, among others.
Reference
Usui J, et al. Clinicopathological spectrum of kidney diseases in cancer patients treated with vascular endothelial growth factor inhibitors: a report of 5 cases and review of literature. Hum Pathol. 2014 Sep;45(9):1918-27. Review. PubMed PMID: 25087655.
#TeachingPoints #kidneypath #renal #pathology
Nodular diabetic GS can have double contours..But not this much
This case has superimposed chronic TMA related to VEGF inhibitor
🔸Some can have PAS-positive pseudothrombi (also described with TKI inhibitors)
https://t.co/8pVQV5U18h
https://t.co/rlLIoWHRyL
#renalpath
It's not always just diabetic GS
Case of diabetic GS with chronic TMA 2/2 tyrosine kinase inhibitor (TKI)
🔸Anti-VEGF effects
🔸Most within weeks to months after starting TKI
🔸TMA +/- PAS+ pseudothrombi
References:
https://t.co/zixSoWDD2U
https://t.co/vrOfwUw6Oo
#renalpath
Bx for AKI in a pt on checkpoint inhibitor: neutrophil rich tubulointerstitial nephritis. We would usually think pyelonephritis, high risk neutrophil rich variants of CKI inhibitor AIN have been characterized. https://t.co/wHkozCOZaa #renalpath#pathtwitter#nephrology
Impressive review. Hypertension might be just a result of complement-mediated TMA here.
Severe hypertension with thrombotic microangiopathy: the need for pathogenically targeted treatments - Kidney International https://t.co/dYrUBCFJsF
Classic powdery electron dense deposits along GBMs, TBMS, and in vascular walls by EM in this case of light chain deposition disease. #renalpath#pathtwitter#nephrology
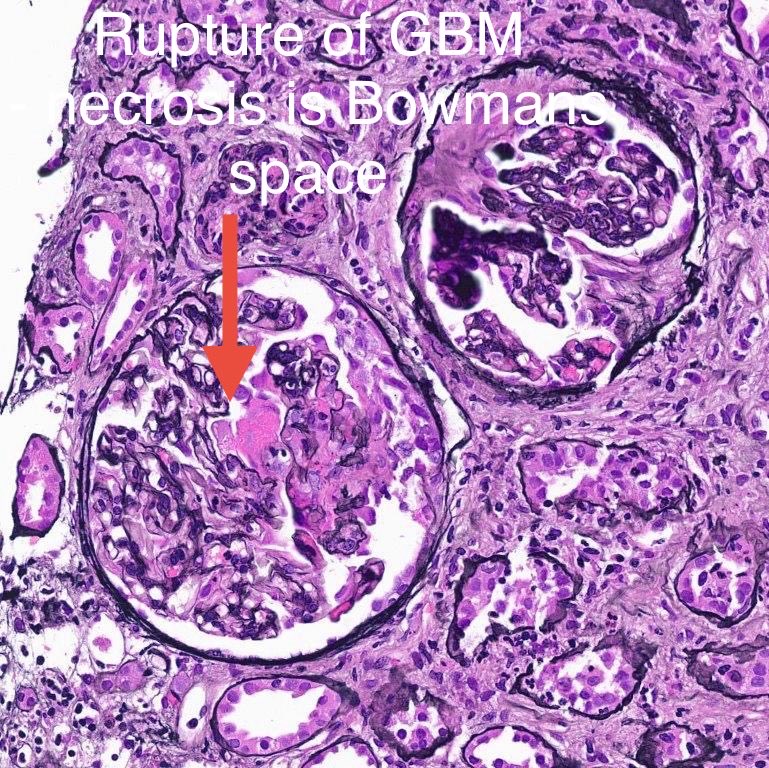
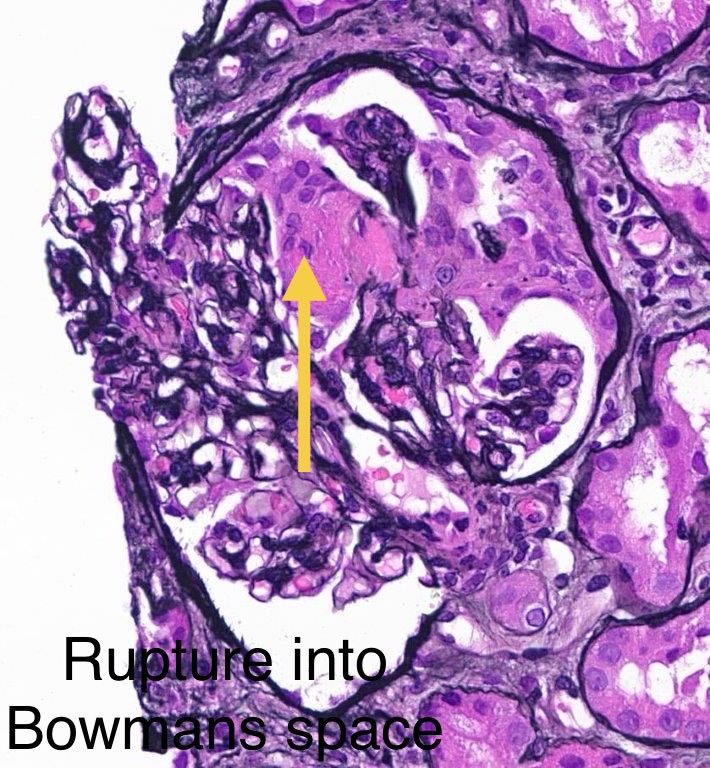
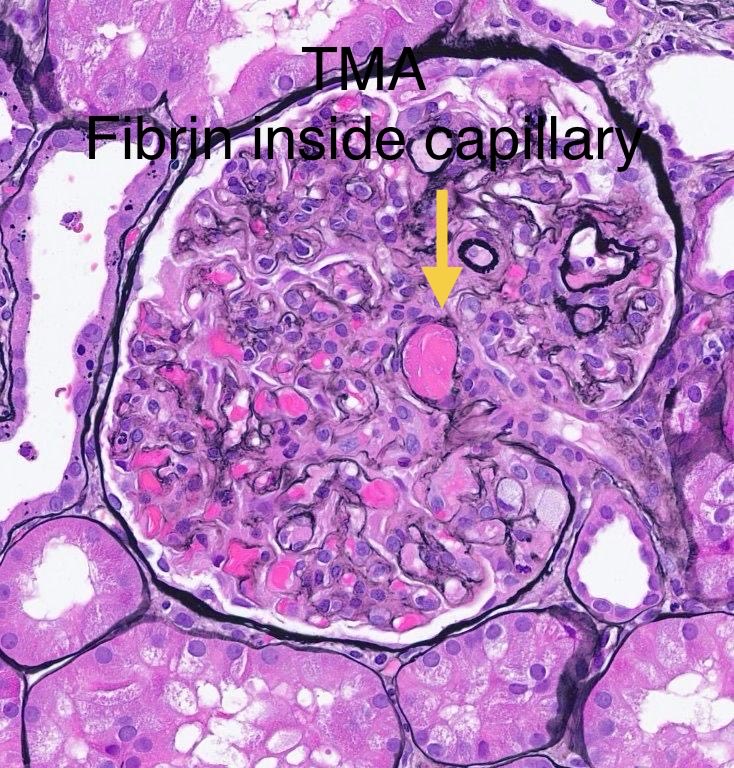
Simple concept: Fibrinoid necrosis (necrotizing glomerulonephritis) versus Fibrin thrombi (thrombotic microangiopathy, TMA)
1. In fibrinoid necrosis, there is breach/rupture of the glomerular basement membrane (GBM), & fibrin is present in the Bowman’s space.
Top panel.
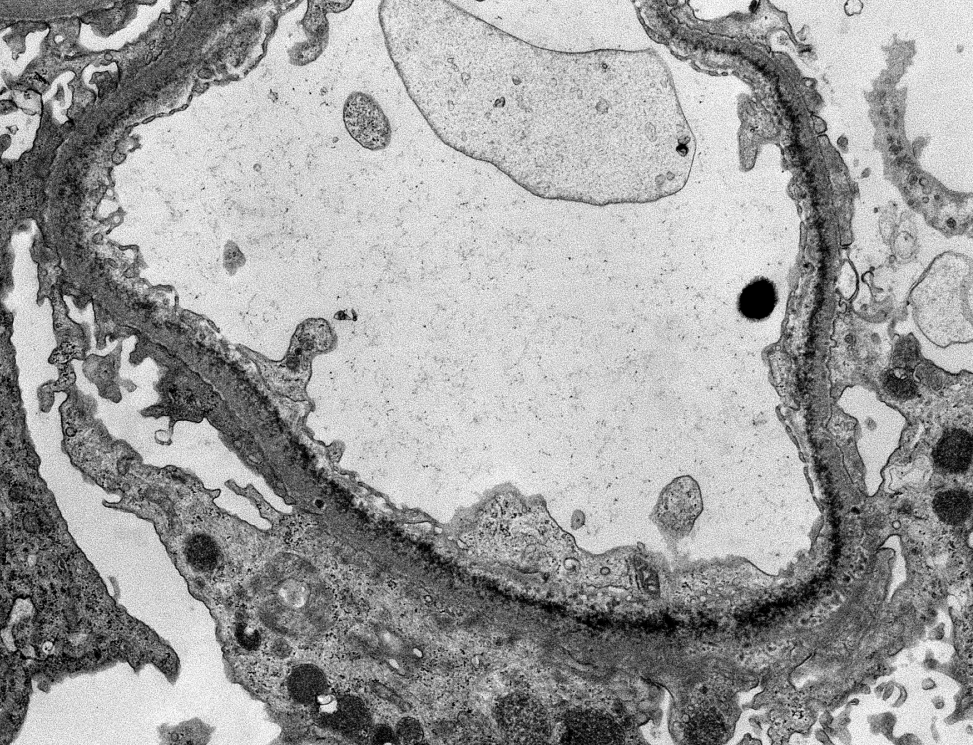
2. In fibrin thrombi, the glomerular basement membrane is INTACT. There is No rupture of the GBM. Fibrin is present within glomerular capillary, and not in Bowman’s space.
Bottom panel
Case 6 (2026): A 20 year old was biopsied for acute renal dysfunction. Urinalysis was bland. IF was negative. What’s your diagnosis? What are the common causes for this pathology? #askrenalpath
Evidence-based guidelines for Laboratory Workup of Amyloidosis from @Pathologists in the March issue of Archives of Pathology & Lab Medicine
Don't forget to use the TRITC filter to screen the Congo red slide (if you have one)!
https://t.co/7k0rRqaLKY