Sim Pub with #AHA24 in @CircOutcomes:
Is cost to blame for disparities in access to semaglutide? Not always
📝 shows inequities in Semaglutide Prescriptions persist even in the VA, w/ its universal access to free or low-cost health care
🧵 (1/2)
Stanford Health Policy researchers lead new study that finds screening all U.S. adults 35 and older for Chronic Kidney Disease would increase life expectancy in cost-effective way. 🫘📷 =📷https://t.co/RZwwGoGX0M
#StanDOM researchers (including @beccatis, @gchertow & @dkowens) determine that screening everyone aged 35 & over for #ChronicKidneyDisease could be a cost-effective way to increase life expectancy. https://t.co/fCtUmfwAQG
The team that hikes together and @vahsrd conferences together, stays together! All-star mentor @DonnaZulman promoting teammate achievements both academic and physical 😄 @va_vccore @Ci2iFellowship
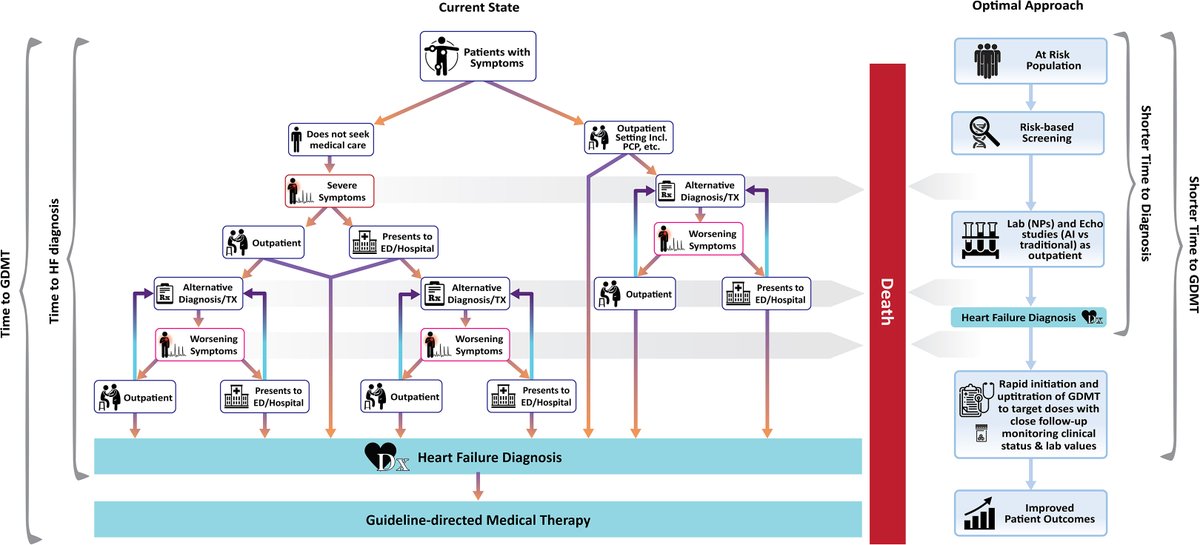
Some fantastic @vahsrd work here via @beccatis on what the location of a first diagnosis of HF can tell us about our patients. No surprise…inequalities appear to exist
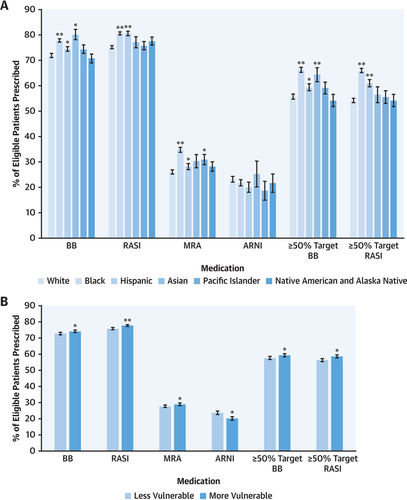
New work in #JACCHF@CelesteWitting@ATSandhu on a VA cohort analysis of pts w/ new HFrEF, studying GDMT implementation + optimization
✅ No significant disparity by race
✅ ⬇️ rate of dose titration in rural pts
Opportunity to leverage telemed?
📎 https://t.co/rCrTzKSlYR
Many first #HeartFailure diagnoses occur in the acute care setting, especially among socioeconomically vulnerable populations. Better outpatient care was assoc. with lower rates of an acute care diagnosis. https://t.co/HzSGFHrrDL
#JACCHF#CardioTwitte@beccatis
Disparities work is hard work ✊🏻✊🏽✊🏿 @American_Heart & @ABCardio1#HF Data Challenge out today in @CircHF Special Issue.
In analysis of #GWTG-HF, we found Black, Hispanic, and Indigenous patients had ⬆️🏥length of stay for HF than White patients.
https://t.co/cbbh1GosnM 🧵/4
Honored to comment on @JAMANetworkOpen findings that virtual care (VC) after ED visits may not be as good as F2F follow-up.
My take:
1. need MORE studies on the optimal use of VC
2. Not all VC is the same: video vs. phone
3. Is there an optimal mix of VC & F2F care?
1/2
@beccatis & I discussing this interesting paper in @JAMANetworkOpen on the concordance of virtual to in-person diagnosis.
https://t.co/DGeJ5NVW51
Authors find concordance rate of 87%. Not gonna lie, this seems high? Or, am I truly underestimating the power of virtual care?