Head of Oncology Department @KUTRRH.
Fellow at European School of Oncology @ESOncology and @IEO. ASCO24 IDEA Awardee. Top 40under40 2024. Proud Kilifornian
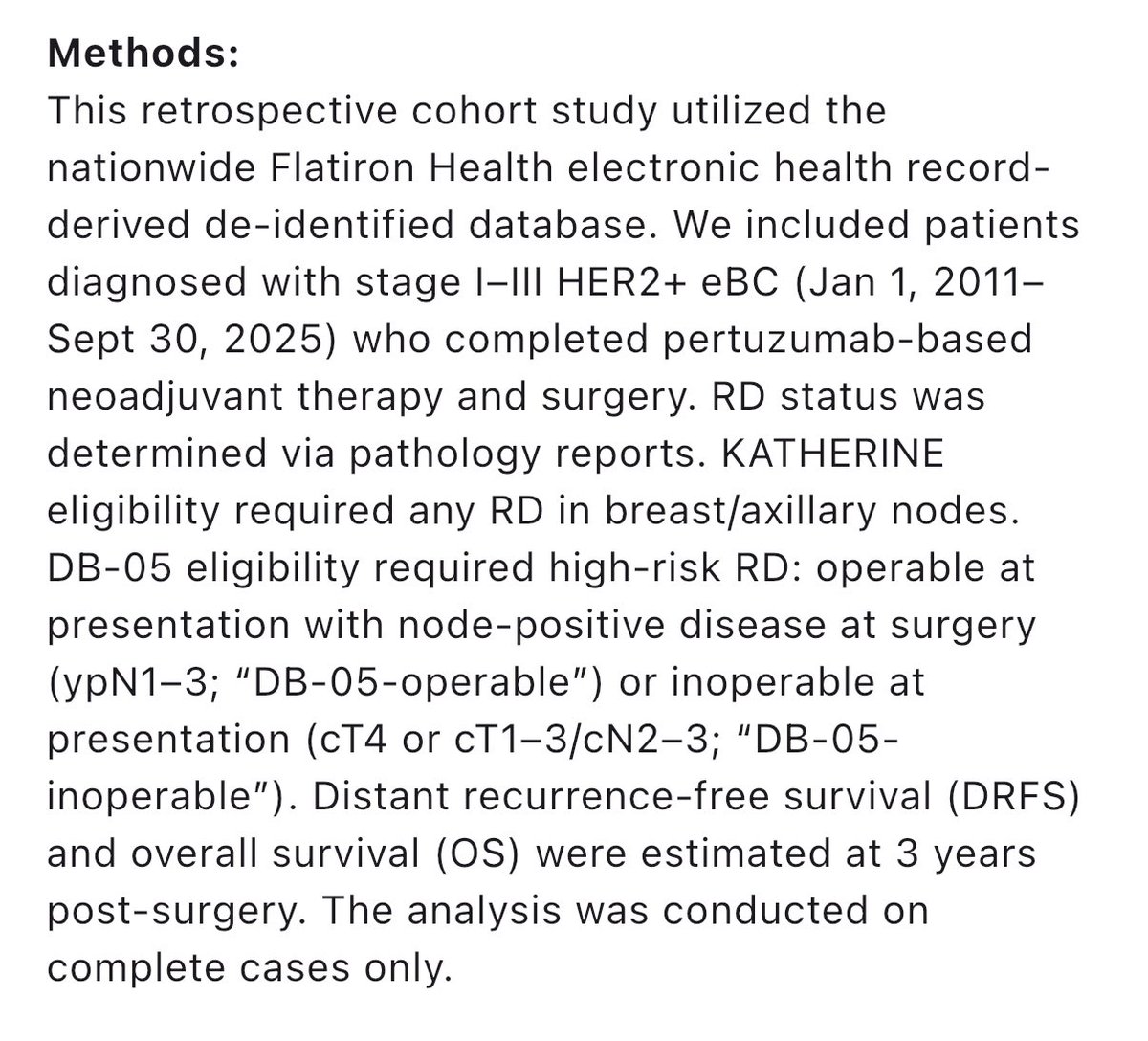
Adjuvant T-DXd is approved for pts with HER2+ BC and high-risk RD by DB05 criteria. What about pts with lower risk RD? We looked at ~10.000 pts in Flatiron, finding that 52% have low-risk RD, with 3yr DRFS 94%, suggesting that T-DM1 remains an adequate SoC for them. #ASCO26 Ab545
New @JCO_ASCO * analysis of ~5,000 HCC patients treated with external beam radiation therapy across 30 centers in 11 countries.
Median overall survival:
-BCLC-0 (very early stage, a single tumor 2 cm or smaller): 6.8 years
-BCLC-A (early stage, single tumor of any size or up to 3 tumors ≤3 cm each): 4.6 years
-Treatment-naive BCLC-A: 5.4 years
Retrospective, but the scale is striking. EBRT belongs in the frontline HCC discussion.
5-year update of FASTTRACK: SABR for kidney cancer by @_ShankarSiva. Organ-sparing at its best A single arm study that changed the guidelines! Stellar effort for the our field and our patients.#ESTRO26 https://t.co/ehJHz7AKU2
🚨 RESET-C trial: single-cycle neoadjuvant pembrolizumab in stage I–III dMMR colon cancer (n=85)
https://t.co/j2KFLLOdVg
🎯 pCR 44% || MPR 57%
💥 DFS and OS rates: 96% and 98% at 18.4 months
▪️ Grade ≥3 AEs in 11%; only 1 recurrence reported
One shot and the tumor may already be hitting the RESET button 🔄
@OncoAlert@OncoReporte@myESMO@_SEOM@GrupoTTD
The names of the candidates running for the ESMO Presidency 2029-2030 have been announced. Find out more about the candidates and their vision. #ESMOElections
🔗 https://t.co/hckWMPVahg
🌟 Honored to speak at #ESMOBreast26 today on "Adjuvant CDK4/6 inhibitors: Could they replace chemo for intermediate-risk ER+ eBC?"
Outstanding educational session chaired by @SibylleLoibl, with C. Denkert, FC. Bidard & H. Parsons. 🎓
#ESMOBreast26
ER-low breast cancer remains biologically messy.
Prior NCDB data suggested worse OS with omission of adjuvant ET in ER-low disease, especially ER 6–10% / residual disease.
But the Quebec/Canada cohort does not clearly reproduce this signal.
My take: ER-low should not be treated as a single entity.
When possible, intrinsic subtype should guide decisions.
Otherwise, separating ER 1–5% from ER 6–10% and individualizing by residual disease/risk may be more rational than a binary ER+ vs ER− approach.
Kenya’s #health budget is set to rise sharply this year, but the story behind the numbers is intriguing. I dug into the latest #budget books to briefly analyze sector allocations the against the background of a shifting health financing landscape. Here's what I found 👇
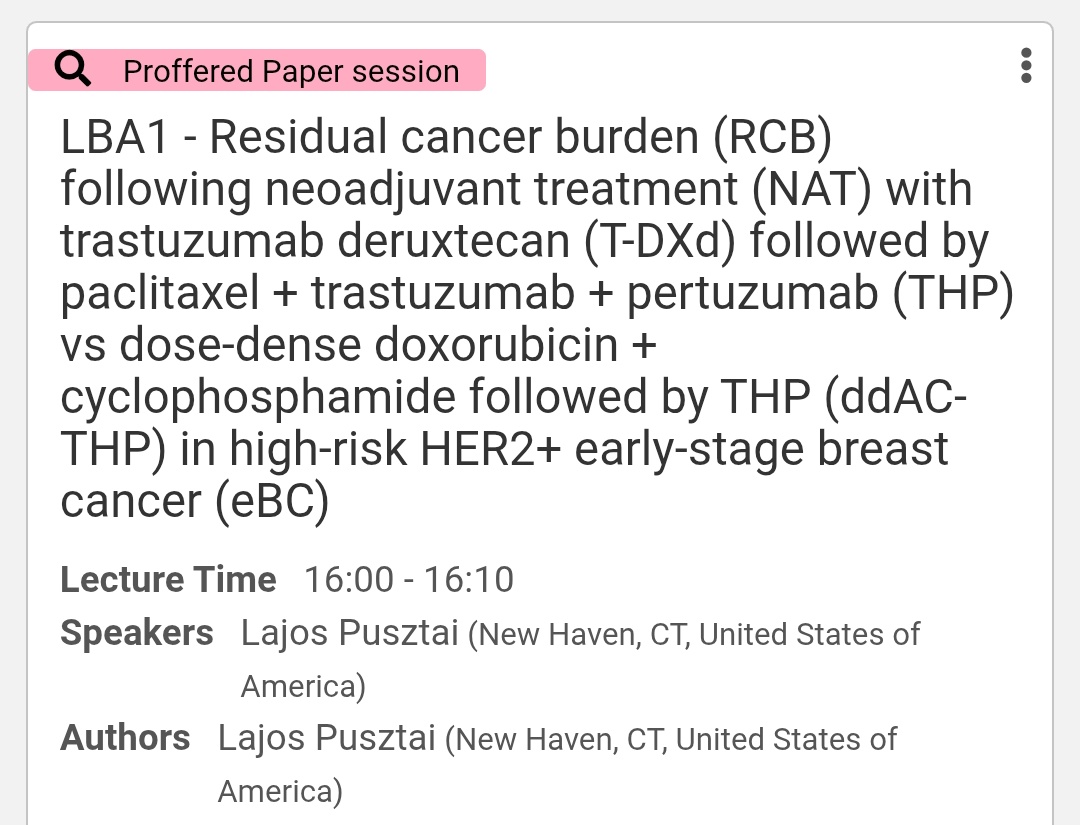
Esmo Breast 2026 - LBAs are out . What's the new data from Destiny Breast 11 ?
It improves RCB across all the subgroups. Looking forward to full data. @myESMO#esmobreast26
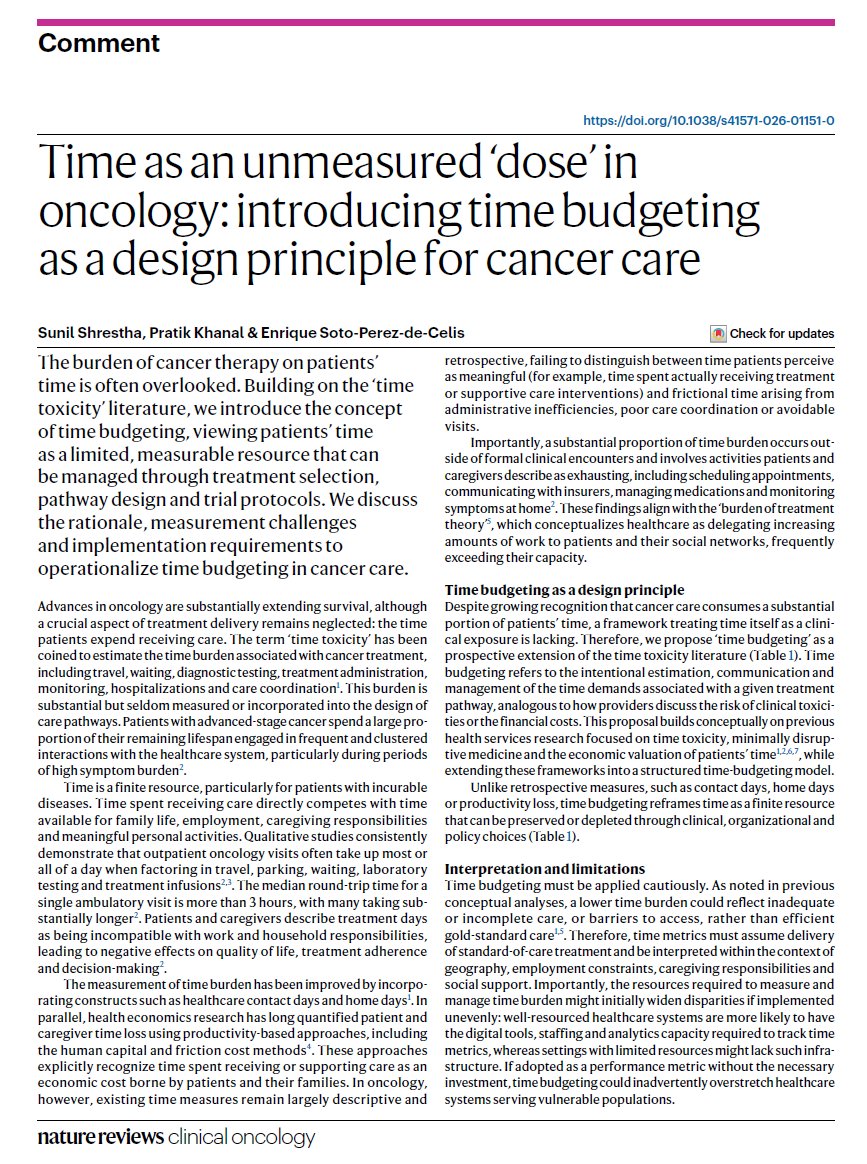
New paper in @NatRevClinOncol !
We propose “time budgeting” as a new design principle for cancer care: treating patient time as a finite resource that should be measured, protected, and incorporated into care pathways & clinical trials.
Because time is also a toxicity. ⏳
Effects of ovarian ablation or suppression on breast cancer recurrence and survival: patient-level meta-analysis of 15 000 women in 23 randomised trials - The Lancet https://t.co/9nWVFxGIVT
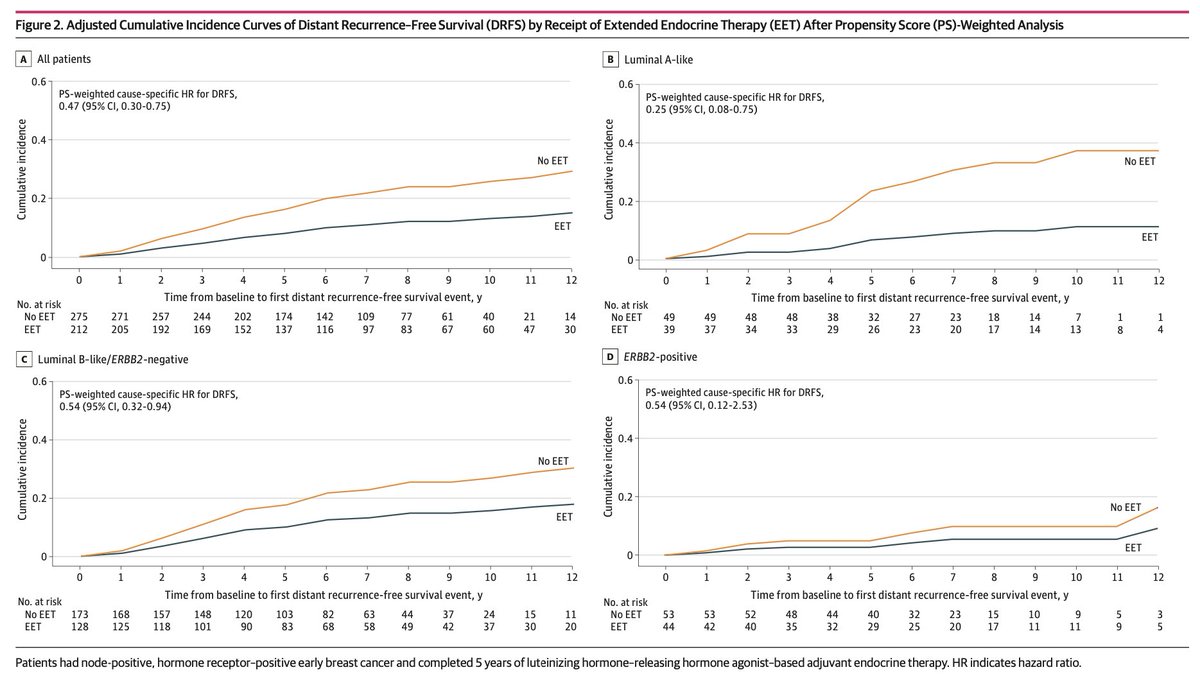
📢 Just out on @JAMANetworkOpen our secondary analysis of extended ET in prem pts with eBC according to surrogate subtypes
🚨 Take home: not only the stage but also biology matters when considering eET beyond 5y of LHRHa
Pts w/ Lum A-like eBC appear to derive greater benefit
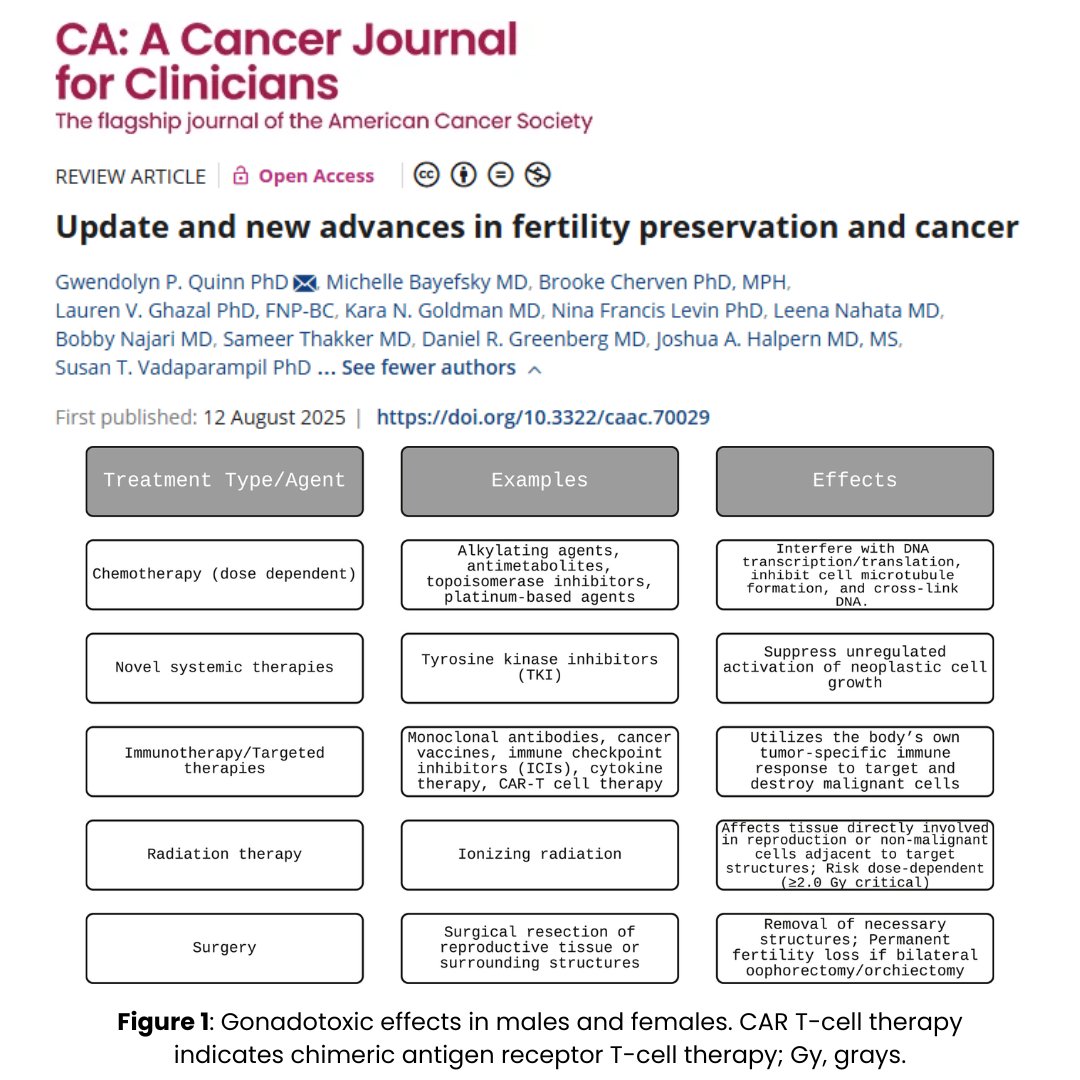
This recent review describes new advances in fertility preservation & cancer, including novel treatments in male and female fertility. Additionally, the authors call for more inclusive methods for gender minorities.
https://t.co/uIq7xsWfMX
@BrookeCherven@lghazal@OncoAlert
Hi friends, it's #LungCancer Wednesday! Here are Top Posts of the Week 🧵
1/ @StephenVLiu on zoldonrasib in KRAS G12D NSCLC from @riess_md:
https://t.co/ZHsS4hxlBZ
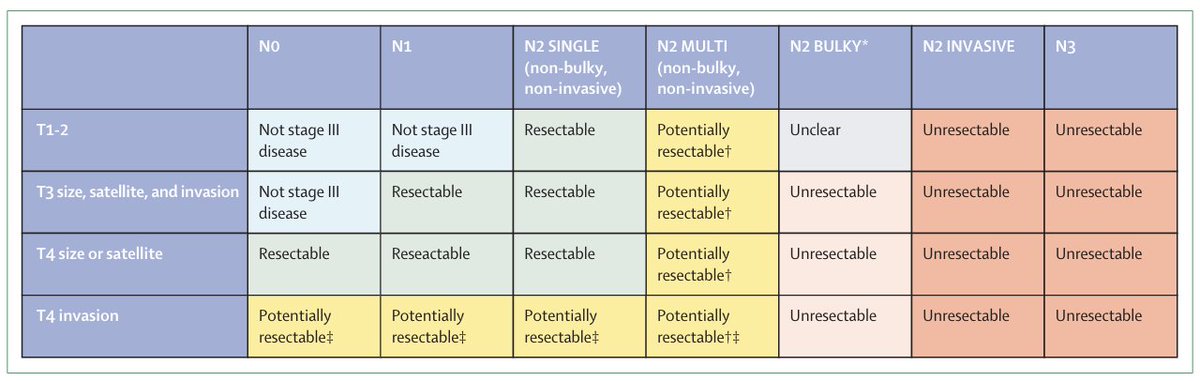
Consensus definition on resectability of stage III NSCLC from @EORTC published @LancetRespirMed. Current consensus is that N3 or bulky N2 is unresectable but multi-station N2 remains potentially resectable. Does not lend itself perfectly to a flowchart given heterogeneity:
Here is Version 2.0 of when to hold systemic tx during RT. Updated & w 3 additional drug categories (ADCs, CDK4/6 inhibitors, PARPi).
More details on newer drugs in 🧵 below.
Please use this version as reference & thanks for all input/experience crowdsourcing! (1/3)