@Dee_Knipe@suicideresearch@lab_jobes Having said that, I also agree there is a spectrum and we need to be able to distinguish when further care and support is needed. But, this requires treating suicidal ideation as an outcome and developing evidence-based guidance akin to what we have for self-harm.
@Dee_Knipe@suicideresearch@lab_jobes That assumes we pathologise self-harm by treating it, which I don't agree with (although it is clearly still happening). Moreover, there is no evidence of a difference in suicide risk between suicidal ideation and self-harm (see Large et al https://t.co/dgcPMifZFm)
This incredible study looked at emergency department visits in children for suicidality (attempts & ideation) before & during the pandemic and found, unsurprisingly:
a) kids more likely suicidal during school months
b) school closures associated with DECREASED ER visits
/1
RESEARCH SEMINAR | Join us to learn more about the patterns of mobility among primary school children in the Northern Territory, presented by Prof. Steve Guthridge from Menzies Centre for Child Development and Education. Register: https://t.co/NecP7AImIE
On the look out for recent psychology grads in Australia. Did you graduate from ANY psychology Uni studies (undergrad or postgrad) in Australia in the last 5 years? We are super interested in your thoughts about suicide prevention and support.
Unclear why ⬆️ in self-harm was only in girls aged 13-16, not older. Rates in boys fell.
Likely a combination of pre-Covid & pandemic factors. SH has been rising for several yrs & moving down age range to younger adolescents - a new prevention priority.
@LancetChildAdol study.
Work with our wonderful team of suicide and mental health researchers & benefit from a project that collaborates with a bunch of other brilliant researchers! We’re looking for a postdoc with interest in suicide prevention, translation, implementation https://t.co/7rqn5HlCrs
Too few studies of suicidal ideation in hospital settings, despite there being no evidence of a difference in suicide risk compared to self-harm (see Mathew Large's SR). Important work from Northern Ireland to help fill this gap.
🚨New open access publication @EpiPsychSci 🚨
Emergency department presentations with suicide and self-harm ideation: a missed opportunity for intervention?
See thread below ⬇️
#MentalHealth#SuicidePrevention#SuicideResearch
https://t.co/i139Qnzlpd
TFW you are 3/4 of the way through writing up a systematic review and realise you added the wrong PDF for one study...so much work for such a silly and simple mistake :(
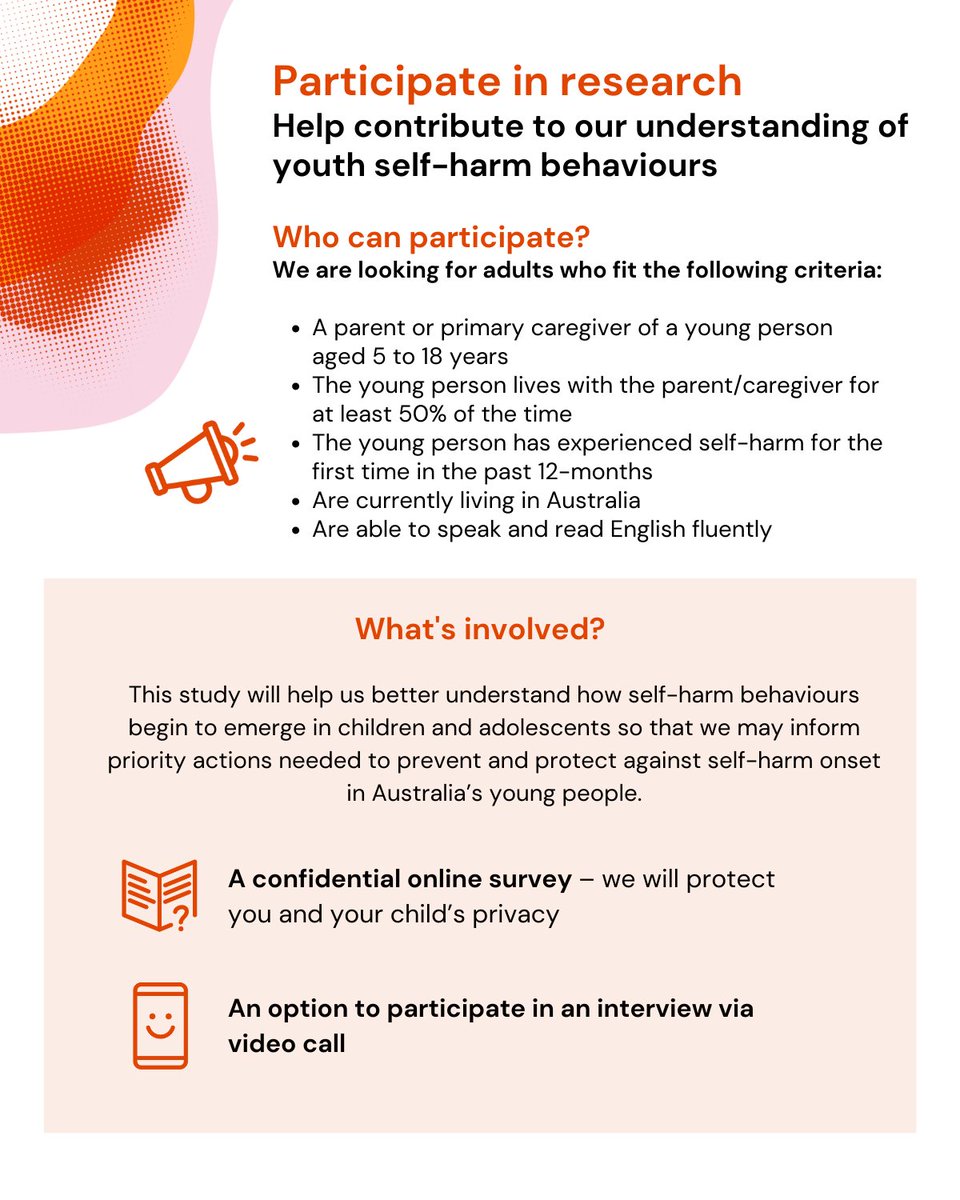
Take part in a confidential survey and/or optional interview to help us find urgent solutions and protect our young people. Learn more information and get started 👉 https://t.co/YhwhCrKm5E
Child protection contacts are an important opportunity for early intervention that we're ignoring (bordering on neglect!)
Things are changing but we're still not doing enough to help some of the most vulnerable children & families in our community!
Preventing suicide in Australian young people requires policy beyond the health system.
Our new paper in the MJA: https://t.co/HQFNAQu1MO
Almost 75% of self-harm and suicidal ideation incidents in health records involved young people in contact with child protection services
We're still looking for practitioners to share their experiences of delivering suicide safety planning!!
Thank you to all the lived experience respondents - v grateful and humbled ❤️
Really looking forward to combing the wisdom from both perspectives to see how we can do more!
We’re seeking mental health practitioners who have delivered safety planning, to share their experiences with us via an online survey 👉 https://t.co/5C9MZTNRWm
Ok this is big.
Web of Science just removed the MDPI flagship journal IJERPH from their lists. This means IJERPH has no more an Impact Factor.
Why is this big? What are the implications? 🧵
Do you deliver safety planning to people experiencing a suicidal crisis or know someone who does? We would love to hear from you!!
Help us learn more about what is happening and how we might be able help improve delivery and outcomes. Click the link below to share your thoughts!
We’re inviting 200 people, both those with lived experience of safety planning following a suicide experience, and mental health practitioners who have delivered safety planning, to share their experiences with us via an online survey → https://t.co/5C9MZTNRWm
The most interesting thing for me about this work led by @DrLeahQuinlivan is that patients tend to report the same barriers to adequate care! Much more can and needs to be done with a focus on implementation where aftercare services exist.
Have to catch train 🚆:
Free access to paper @TheBJPsych-: https://t.co/mDfY5lbMoB
We also conducted a patient paper- published v soon.
T: @PSTRC_GM @DonnellyGorman @LizMonaghan5@StephenMarks12 Sadika Asmal, Roger Webb, Nav Kapur @NCISH_UK@mashproject
Nav Kapur +MS4MHr
@FionaShand1@DrLeahQuinlivan@DemeeRheinberg1 Some very honest insights into medicalisation of acute distress and clear pathways to improved care. Also need to think about $$$ to support this - very little real increase in MH spending and where is it going? Need to ensure balance between and targeting within levels of care
@DrLeahQuinlivan@NICEComms @Dr_KatrinaWitt is leading a SR and MA of the prevalence of psych ax, in/out-patient care following hospital-treated self-harm. Interestingly, improvements in prev. of psych ax over time (evidence of impact of guidelines??), but highly variable rates of ax and care globally.