Seven Things This 63 Year Old Surgeon Would Tell My 40-Year-Old Self
I am 63 now, and I spend my days as an orthopedic surgeon watching how people's earlier choices show up in their bodies decades later. I see it in my college friends, high school buddies, and patients that I have known for 20+ years. If I could sit across from myself at 40, here is what I would want that man to understand. None of what follows is complicated, and all of it compounds over the decades… either against you… or in your favor. You are largely in control.
@smithECGBlog@PendellM@PMcardioApp The 2 takeaways in this excellent blog post are:
1. Try to find an old ECG to compare to
2. Repeat the ECG in 15 minutes.
(the ECG should always be repeated, even more than once, before the troponin gets repeated)
Must-peruse case of dual-access controlled snare retrieval for bailout management of aorto-ostial LM stent entrapment, highlighting the importance of systematic intravascular imaging after complex LM retrieval https://t.co/g1yoJJpUQU
A 77-year-old marathon walker developed a headache. Over the next four months, she was seen by a nurse practitioner, a PA twice, a medical assistant, and an emergency room. She was given two Medrol dose packs, NSAIDs, and a prescription for fluoxetine after a PA decided she had anxiety. She had never actually seen her primary care physician. She had giant cell arteritis. A sed rate of 41 confirmed it, the moment her neurologist finally examined her, took her history, palpated her temporal arteries, and asked about jaw claudication.
The patient told her neurologist: "if you think I need fluoxetine I'll be on it, but I don't think I'm anxious and this headache is just crazy."
The structural argument matters more than the cinematic detail. Team-based care is sold as a solution to the physician shortage. The math runs the other way. If a physician is the diagnostic instrument that holds the differential together on a multi-system presentation in a 77-year-old, the marginal cost of putting that physician in the room at visit 1 is zero. The marginal cost of NOT putting that physician in the room across this case was four office visits, an ER visit, two courses of steroids that partially masked the inflammatory signal, a misdiagnosis of anxiety, an SSRI prescription, and a delay in identifying a vision-threatening time-sensitive diagnosis. The team did not save physician time. It spent physician time everywhere except with the patient.
Reeta Achari, MD, a neurologist in solo private practice in Houston for 25 years, makes the operational case in plain terms. There is a physician shortage. The response has been to use physician time for documentation, prior authorizations, peer-to-peer calls, board recertification weeks, and electronic-record data entry. The response should have been the opposite. If there is a shortage of the diagnostic instrument, the workflow has to put the instrument in front of the patient, not behind four other people.
Her own response was structural. She opted out of Medicare. She built a quarterly subscription practice with prices middle-class patients can afford and scholarships for long-relationship patients. New patients get a one to one-and-a-half hour intake. Follow-ups get 30 minutes. The model is not concierge. It is continuity, priced to clear.
The diagnostic line from her conversation: "No physician touched her."
Listen to the full conversation on The Podcast by KevinMD. Link in the replies.
What does the cascade in your practice or your own care look like? Where in the workflow did the physician finally enter the room?
#ThePodcastbyKevinMD
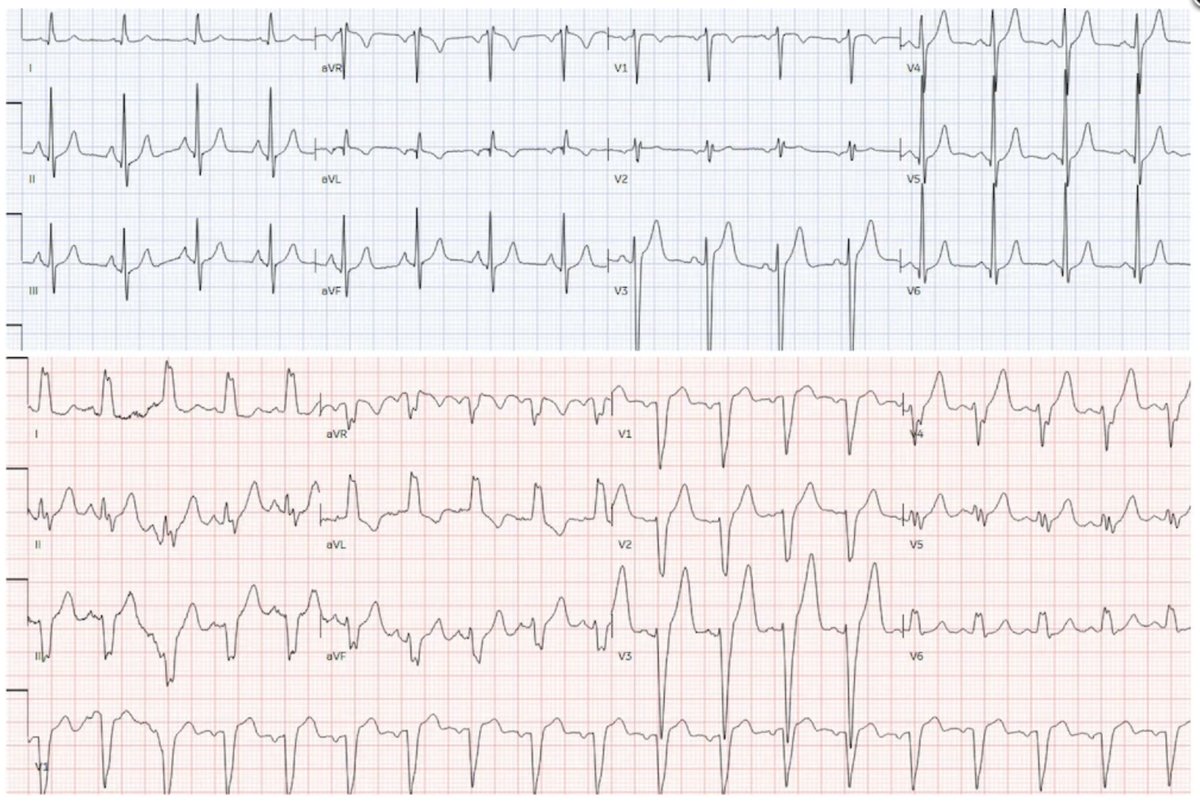
65 year old with chest pain + new Left Bundle Branch Block: is this acute coronary occlusion?
https://t.co/s6G2mnxxl6
@ECGcases
Old ECG on top. New on bottom.
@DavidJuurlink I actually have a colleague who, when provided with the most trivial & seemingly irrelevant detail, can the recall the entire (chronic) cardiac history and all cardiac lab results (EF to the percent)!
@drjohnm I have actually seen a referral note, likely AI generated, with the phraseology “Would you like me to formulate a concise assessment and treatment plan for…” that finishes with “refer for cardiac cath”.
I’m so incredibly frustrated. We have an outbreak report for the cruise ship, published in NEJM, and great clinical, epidemiological, and genomic reporting, and…
NOT A SINGLE MENTION OF VENTILATION/FILTRATION SETUP ON THE SHIP
Folks, we keep doing this. A lot of MD/PhD coauthors on the “Andes Virus Outbreak Working Group”, and no one with expertise on mechanical systems. And no one on the team even thought to check or investigate it.
It’s malpractice at this point, and I’m not exaggerating in my use of the term. I do investigations in buildings and if I failed to check the status of the mechanical systems I’d be sued. (It’s actually *the first* thing I check)
@NEJM: see our report from The Lancet COVID-19 Commission on this in the thread. Include this in your reviews. Mandate this info in every outbreak investigation report.
The reason I first called the doctor on the ship was because I wanted to see if he could get info on the ship’s systems before he left it, bc I knew the official investigations would miss it. Because they always do.
@nickmmark@Flynn38080271 When CPR started en route to Cath Lab, Lucas allows us to work without interruption of compressions. I see very few people who don’t show “hemodynamics” signs of fatigue within 20 seconds. I am often calling out “next” in addition to the rest of my cognitive load.
@angularboxoid@abhinuv23@drjohnm Usually because the troponin is positive…
Why would patients with new AF (and nothing to suggest angina, let alone ACS) get a troponin drawn?
@ellecreative 🤷♂️
It's really up to circumstances outside of our control or knowledge at this point
If 100 embers are scattered to the wind will one of them catch fire? 🔥
That's where we're at right now
It's widely accepted that hantavirus transmits from rodent excreta to humans via inhalation of aerosolized virus, so I don't understand why we're so reluctant to acknowledge the inhalation route for human-to-human transmission.
https://t.co/aGFDKS94Qk
An important measure of how much contact is required for transmission, and for how long, will come from passengers on the airplane that carried a critically ill cruise passenger who died shortly after the 4.5 hour flight to Johannesburg. Late this week, a flight attendant, with potential symptoms, tested negative.
I was up last night with a STEMI until 4:30. For my entire career I’ve gone to work the next day with whatever sleep I could get. Not anymore. Today, I slept in and did chart work from home. You can’t fly an airplane or drive a truck if you’ve been up all night. Why should it be different for docs?