Interested in thiamine deficiency and COVID, keto diet, renewable energy, building energy efficiency, regenerative agriculture, permaculture, computing, scottis
Please note: my arguments for a connection between the level of thiamine sufficiency or deficiency in the body and outcome following COVID infection are my unqualified speculations, based on the work of Drs Derrick Lonsdale and Chandler Marrs at
https://t.co/l2keKKRhIE
Selective Serotonin Reuptake Inhibitors block the transport of vitamin B1 (thiamine) by inhibiting SLC19A3 one of two Solute Carrier (SLC) transporters accidentally inhibited by the same mechanism as the serotonin transporter (SERT/SLC6A4).
Thiamine genuinely reverses brain damage on some studies on this matter.
SLC19A3 is the principal mechanism for driving thiamine across the intestinal wall and through the blood-brain barrier (BBB) (Gabriel et al., 2024)
Disrupting the transport of Thiamine causes cognitive harm as B1 is necessary for the creation of acetyl choline.
Also thiamine deficiencies can manifest in brain tissue even if a patient's dietary intake of B1 looks fine on paper (Gabriel et al., 2024).
So SSRI’s not only increase suicidality, mood instability, risk taking behavior, but they also cause cognitive impairment and metabolism issues.
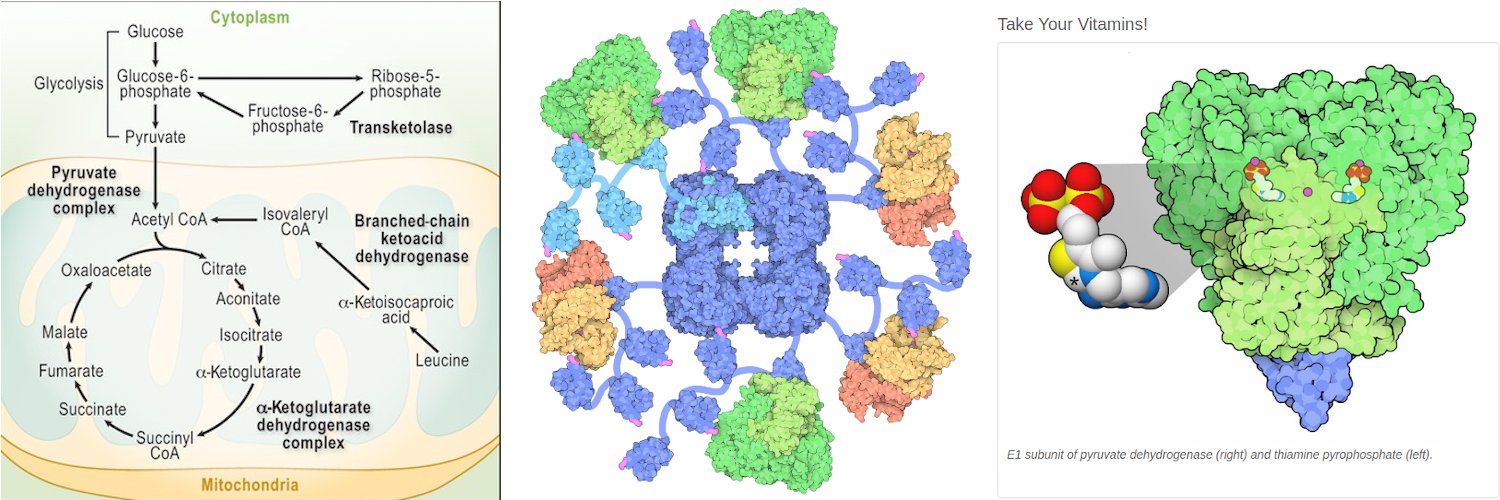
Also thiamine is phosphorylated into Thiamine Pyrophosphate (TPP), a co-enzyme required by mitochondria for the citric acid cycle(Dhir et al., 2019; Lin et al., 2015). Blocking the transport of Thiamine cascades into cellular energy failure, lactic acid accumulation, and heightened neuro-inflammation.
Adjuvant thiamine improved standard treatment in patients with major depressive disorder: results from a randomized, double-blind, and placebo-controlled clinical trial
https://t.co/UbRHskkxQG
Thiamine deficiency is a silent but ever-so-present issue. This is because common foods like sugary snacks, white breads, crackers, sodas, ice cream, and the like use a molecule of thiamine for every molecule of carbohydrates.
Thiamine deficiency can occur within 2-3 weeks of inadequate dietary intake. It is more prevalent in populations with diets rich in carbohydrates but lean in proteins, such as those who rely heavily on polished rice or refined wheat flour.
This deficiency can lead to serious health issues, including beriberi, a disorder characterized by cardiac involvement with swelling, gut issues, memory issues, and neuropathy.
More in this thread! https://t.co/U7LM3v74I5
@BagTooth I have hypothesized that Covid infection leads to increased likelihood of thiamine deficiency and consequent symptoms (see my pinned tweet thread), which is also connected to alcohol consumption.
The Role of Hypoxia in Longevity
"...Hypoxia, marked by reduced oxygen availability, has emerged as a promising area of study within aging research..."
https://t.co/HFODDoSw8a
Long COVID as a network disorder: a mechanism-anchored framework for biological stratification and therapeutic targeting
🚨Interesting new paper that strongly reinforces my own view on LC.
Long COVID is a syndrome, not a single disease, driven by a vicious network of broken systems post SarsCoV2. We’ve been treating too many “shadows” instead of the actual mechanisms.
➡️The paper’s core thesis:
- Long COVID is not one uniform disease but a heterogeneous “network disorder” (= syndrome) where interacting physiological systems create self-reinforcing loops.
- Symptom overlap masks completely different upstream mechanisms, which is why grouping patients only by complaints dilutes trial results.
- That’s why so many trials fail.
- Long COVID is a network disorder built on 6 measurable biological domains (often called endotypes/phenotypes) that constantly interact and amplify each other.
➡️Primary Domains/Phenotypes (objectively measurable, targetable nodes capable of generating multisystem symptoms):
1. Autonomic dysfunction (e.g, tilt-table, HRV)
2. Mitochondrial/bioenergetic impairment (e.g, CPET, lactate)
3. Endothelial/microvascular dysfunction
4. Gut dysbiosis/barrier disruption
5. Mast cell activation (e.g, tryptase, mediators)
6. Neuroendocrine dysregulation (e.g, cortisol, thyroid, sex hormones).
➡️Secondary Amplifiers (sustaining loops):
Persistent immune activation, viral antigen persistence (no replication?), autoantibodies, neuroinflammation, sleep destabilization.
➡️Framework Innovation:
- Presents Long COVID as a “network disorder” of interconnected physiological nodes linked by self-reinforcing feedback loops.
- Includes practical tables that list:
• domain-specific objective tests,
• typical symptom triggers,
• cross-node interactions, and
• explicit, falsifiable hypotheses (e.g, patients selected for autonomic dysfunction will respond significantly better to targeted therapy than patients matched only by identical symptoms).
➡️The practical tools:
• Clear tables of objective tests, triggers & cross-interactions
• Explicit falsifiable predictions (e.g, autonomic patients will respond to targeted Rx while symptom-matched controls won’t)
• A ready-to-use prototype screening tool for real stratification
➡️Author calls for:
Prospective validation comparing biologically enriched vs. symptom-only cohorts to test whether mechanism-guided selection sharpens therapeutic signals and clarifies pathophysiology.
‼️So, Symptom-based medicine has hit its ceiling in Long COVID. Not NEW!
Until patients are stratified and treated according to their dominant biological driver/phenotype, rather than their overlapping complaints, most clinical trials will keep failing and millions will stay untreated.
The network model is deliberately falsifiable as the author states: "Enriched cohorts must now deliver superior outcomes, or the field must finally admit it is still chasing “shadows” instead of mechanisms!"
The field has known for years that we’re dealing with a messy interconnected network. This paper didn’t discover that, it just handed us a clear clinical roadmap to stop pretending it’s one disease.
LC It’s ONE syndrome with 6 major driving mechanisms(phenotypes).
It’s evolutionary, not revolutionary… but exactly the kind of evolution the field desperately needs right now.
One may want to discuss/criticize this framework proposal, no problem, but let it be already very clear, LC is NOT ONE DISEASE, it’s a SYNDROME for which I thank the author!
https://t.co/tentkAbfW2
Small #LongCovid study finds LC patients' cells used way more energy than controls during infection, then way less.
This correlated with LC symptoms & suggests widespread metabolic reprogramming. Cells also ignored crucial hormone and metabolic signals.
https://t.co/f2XYoZTd2A