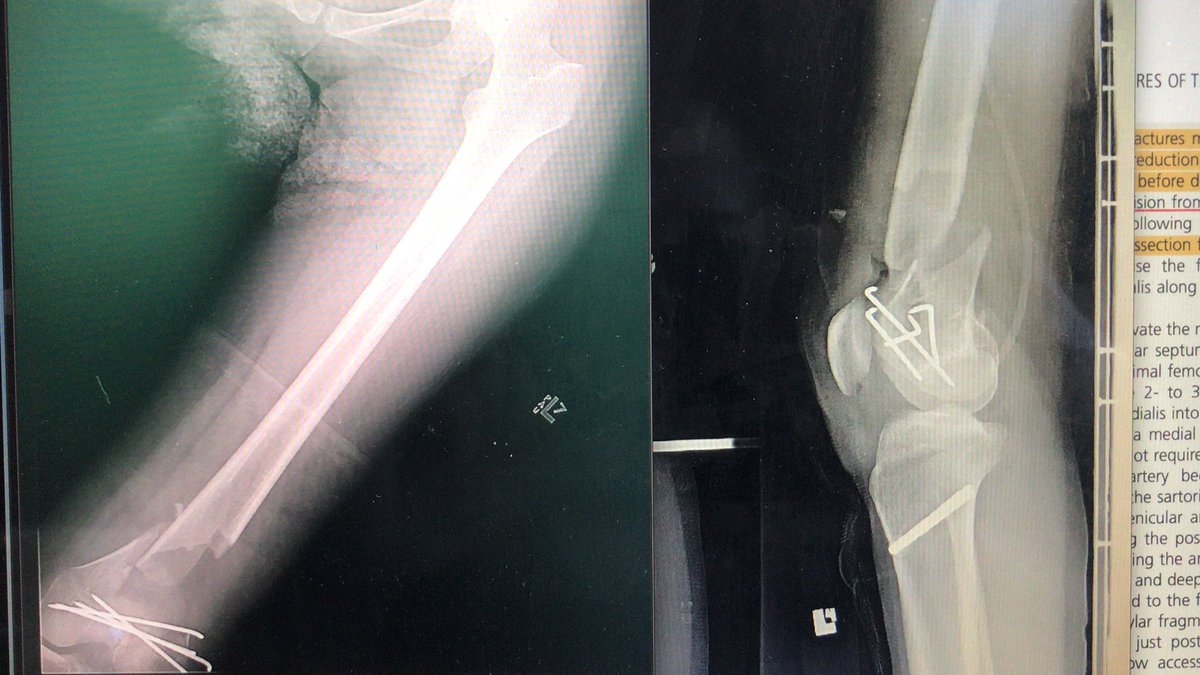
[1/2] Another case done according to Paul’s technique (see linked tweet.) These distal pole avulsions are the cases where it’s very useful because that plate grabs and cups the pole much like the olecranon analogy he discusses in his talk.
@InvictaOrtho Hi just wondering— what’s the principle behind 3 syndesmotic screws? Haven’t encountered here in our practice. And also curious when weightbearing was resumed? Thank you!
An excellent trick to find the radial nerve in posterior triceps split approach, from paper by Frank Liporace: 2 fingerbreadths or 4cm proximal to where triceps aponeurosis meets septum between long and lateral heads of triceps. It’s neat; it has worked every time for me so far.
Tibia fracture fixed with IM nail. Arrow shows the Herzog bend. It’s a little different depending on the nail, but this is frequently a culprit when it comes to proximal tibia fracture displacement if the bend is too distal. See figure on page 102 of this: https://t.co/LCzXupMFU9
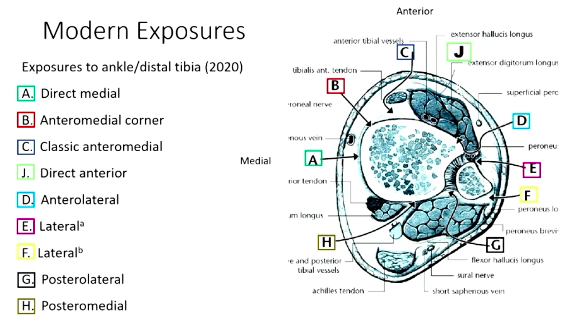
A great slide describing pilon exposures that I saved. I'm pretty sure it's from a talk by @FractureDoc! My most commonly used approaches are a mini-medial, anterolateral, and posterolateral.
Healed ankle. Here I want to point out importance of placing screw in right place and not too medial in low transverse medial mal, otherwise screw won’t capture most of fracture & may even displace it into translation. You really have to abduct foot to get the right start point.
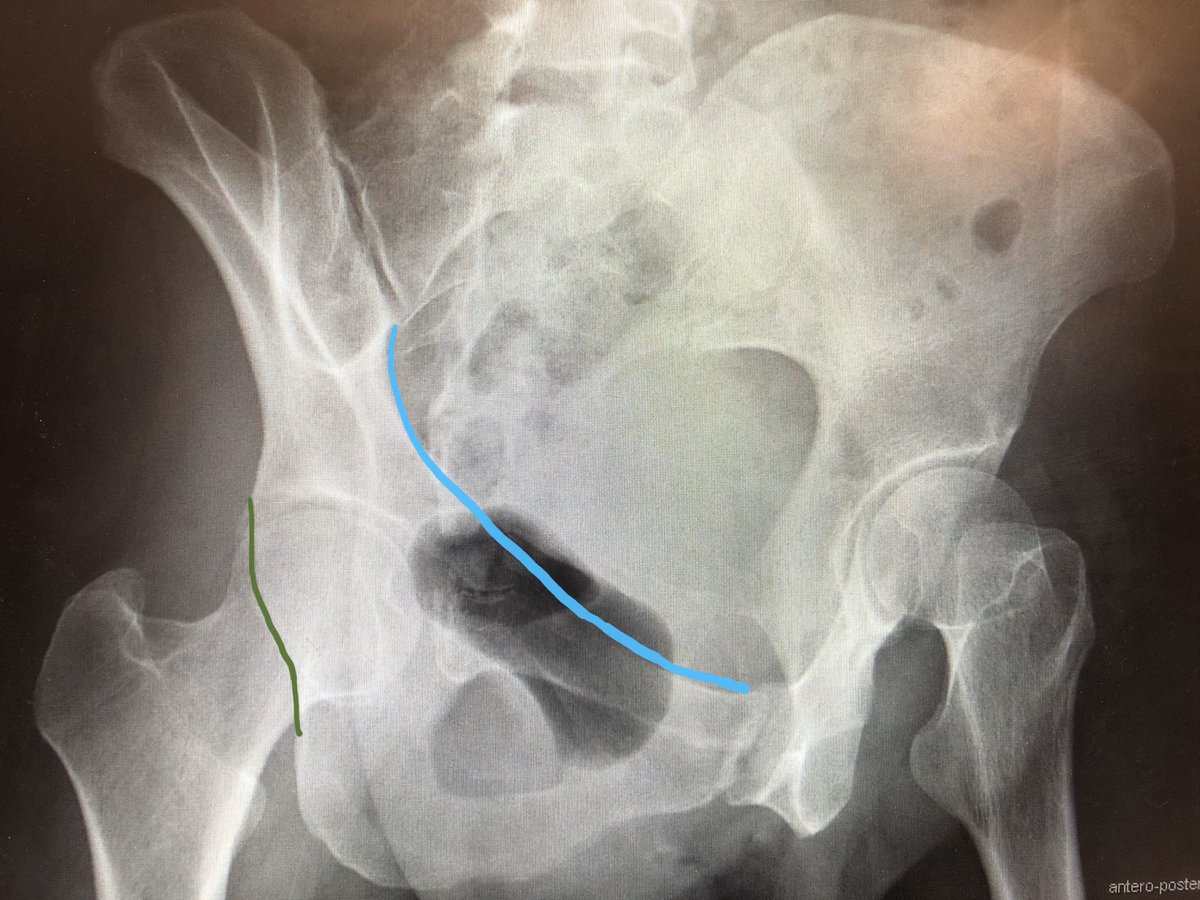
Judet views used for acetabular fractures. Obturator oblique shows anterior column (blue) & posterior wall (green). Iliac oblique shows posterior column (pink) & anterior wall (yellow). Because pelvis is tilted for view, iliac oblique of one side = obturator oblique of the other.
External fixation is in my mind still great option for distal radius. The problem is that people flex wrist instead of translate, causing problem with finger motion. But if done right, people can use their fingers well. My residents haven’t seen one before—is this a dying art?
Currently templating. DFLP + 2 lag screws outside the plate + bilateral autologous bone graft + bone substitute. We did aggressive debridement and minimal fixation at the ER (swashbuckler approach). She will be 4w post injury during surgery. #orthotwitter

![InvictaOrtho's tweet photo. [1/2] Another case done according to Paul’s technique (see linked tweet.) These distal pole avulsions are the cases where it’s very useful because that plate grabs and cups the pole much like the olecranon analogy he discusses in his talk. https://t.co/Ldx29YjdSU](https://pbs.twimg.com/media/E8L-dnwXoAE9kNf.jpg)
![InvictaOrtho's tweet photo. [1/2] Another case done according to Paul’s technique (see linked tweet.) These distal pole avulsions are the cases where it’s very useful because that plate grabs and cups the pole much like the olecranon analogy he discusses in his talk. https://t.co/Ldx29YjdSU](https://pbs.twimg.com/media/E8L-dnwWUAEbu4d.jpg)













![InvictaOrtho's tweet photo. [1/2] Another case done according to Paul’s technique (see linked tweet.) These distal pole avulsions are the cases where it’s very useful because that plate grabs and cups the pole much like the olecranon analogy he discusses in his talk. https://t.co/Ldx29YjdSU](https://pbs.twimg.com/media/E8L-doXX0AENBbM.jpg)