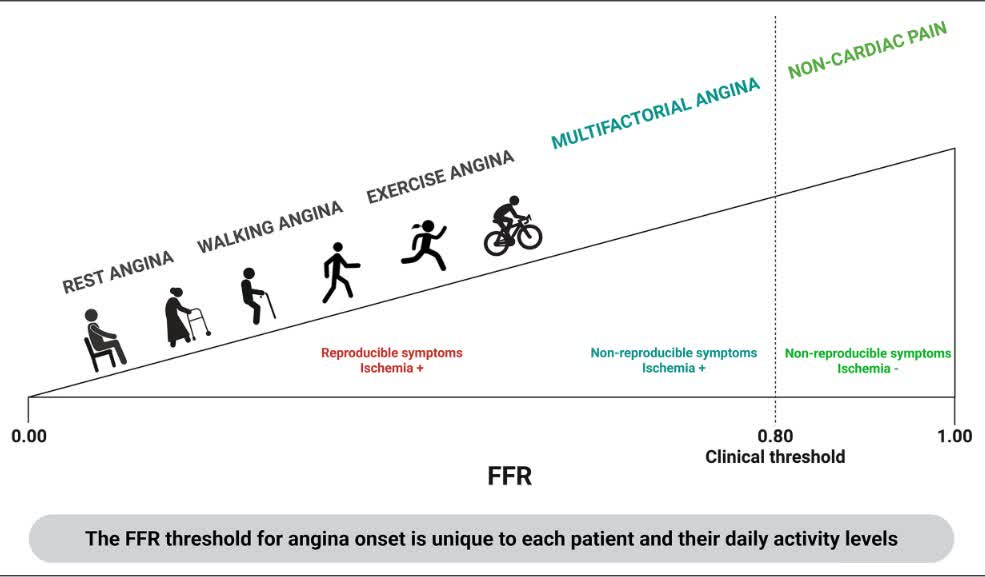
ORBITA-FIRE suggests universal Ischemia-based thresholds for FFR and non-hyperemic pressure ratio should be interpreted with caution: Integrating symptom-linked physiology may refine PCI selection and improve symptomatic response.https://t.co/oGyHMRbOLZ
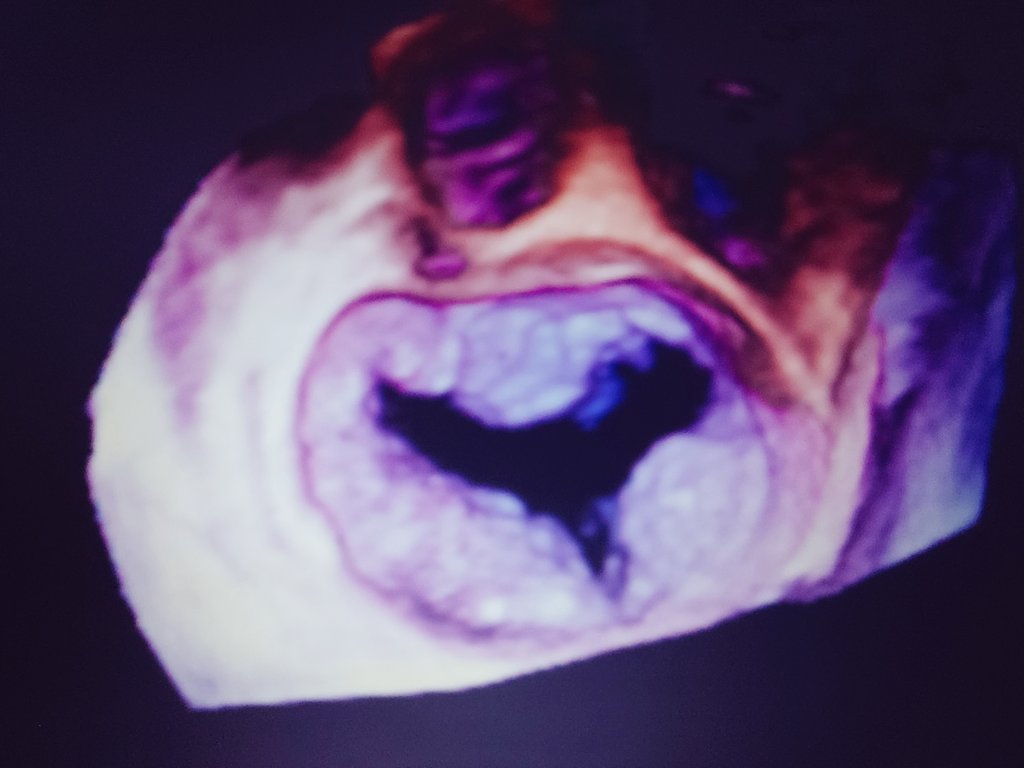
New CMR Case Drop! 🫀
What is the diagnosis of a 66 year old female who presented with dyspnea based upon the CMR images provided?
👇 Drop your answer below!
Answer revealed soon…
#SCMRCases#WhyCMR
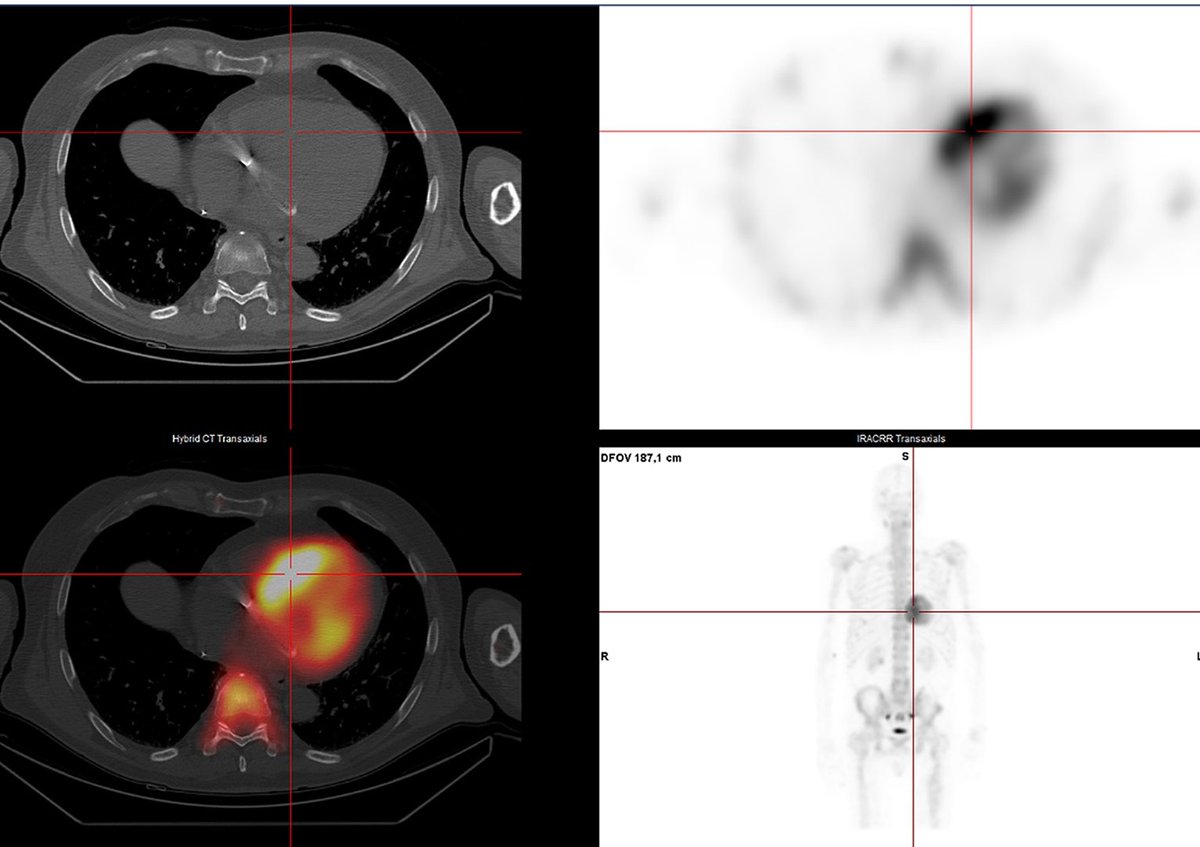
Patients with Fabry disease can have intense myocardial uptake on bone scintigraphy mimicking cardiac amyloidosis. Interesting observation, since there is phenotypic overlap
https://t.co/iuYQQe0fbH
Presented at #ACC26:
Among patients with a preserved ejection fraction at least 1 year after myocardial infarction, stopping beta-blockers was noninferior to continuing therapy with respect to major clinical outcomes. Full SMART-DECISION trial results: https://t.co/dZS03RaTcA
@ACCinTouch
#echofirst
✅ Closing out, 🙏 for all comments
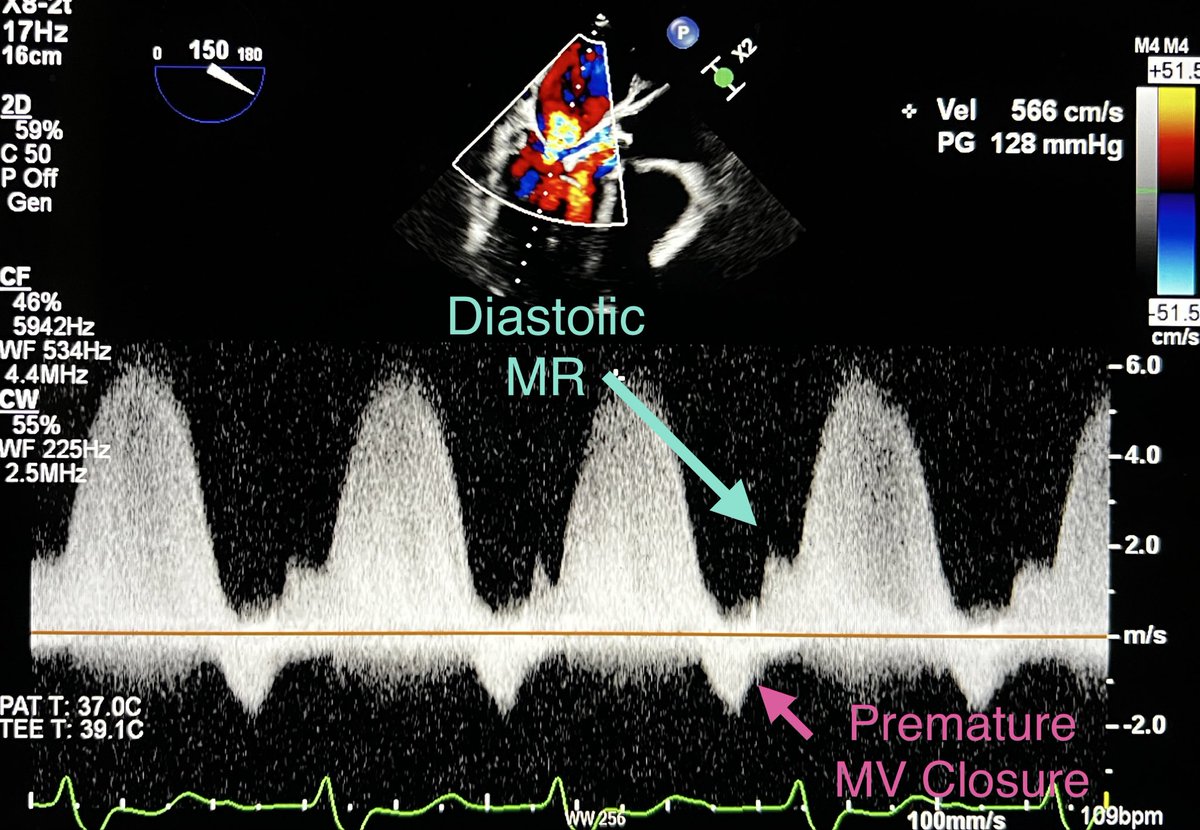
✅ Diagnosis: Post Balloon Aortic Valvuloplasty (BAV), severe acute AR➡️ worsening MR with additional new diastolic MR + baseline mild-moderate MR
✅ Pre-BAV MR CW Doppler signal less dense & with parabolic shape compared to post BAV MR (denser & triangular shaped envelope)- suggests ⬆️in LA pressure
✅ Early/premature MV closure & diastolic MR seen post BAV (image ⬇️)
✅ AR Color Doppler width ratio was difficult to assess after BAV due to presence of catheters in LVOT; thus changes in MR Doppler helped in diagnosing acute AR by echo in this example
✅ Worsening MR in this scenario could be also due to the double curve LV guide-wire ( Safari), but we would not expect diastolic MR in that scenario
@argulian@iamritu@HeartOTXHeartMD@bwoody58
@PWengrofsky
@hvanspall
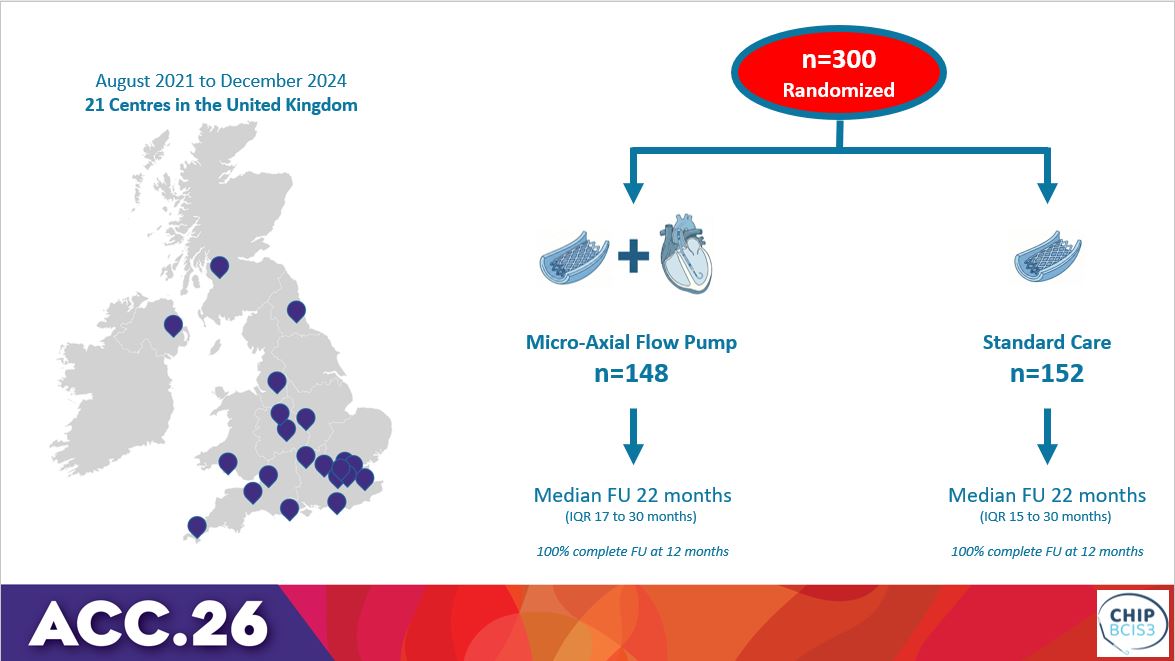
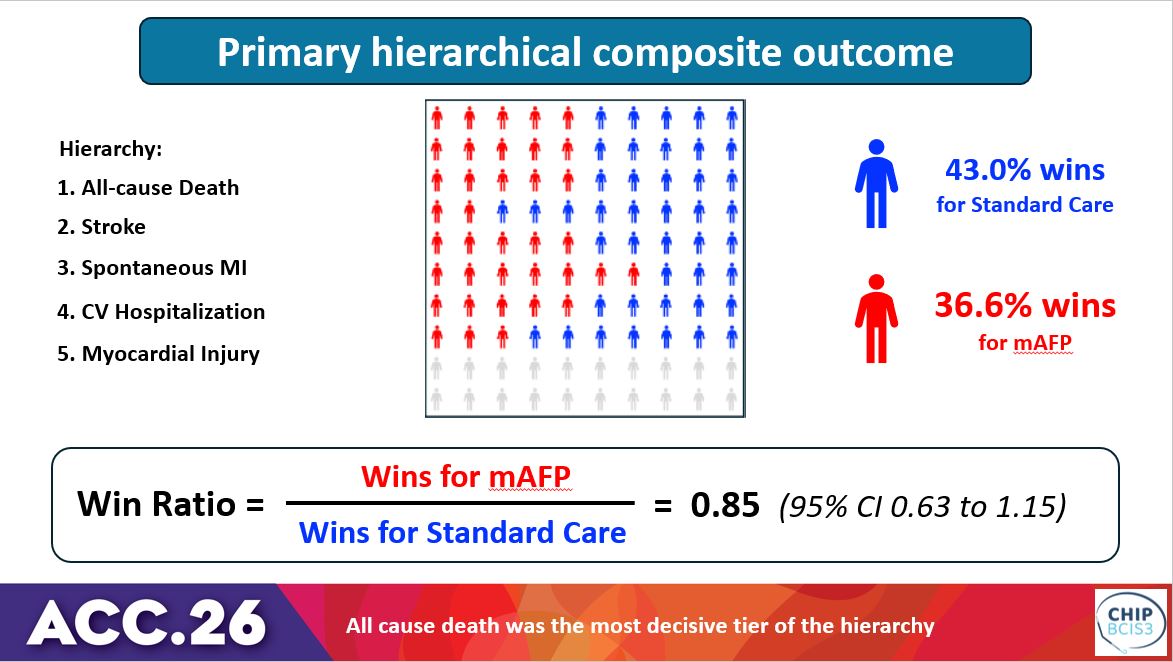
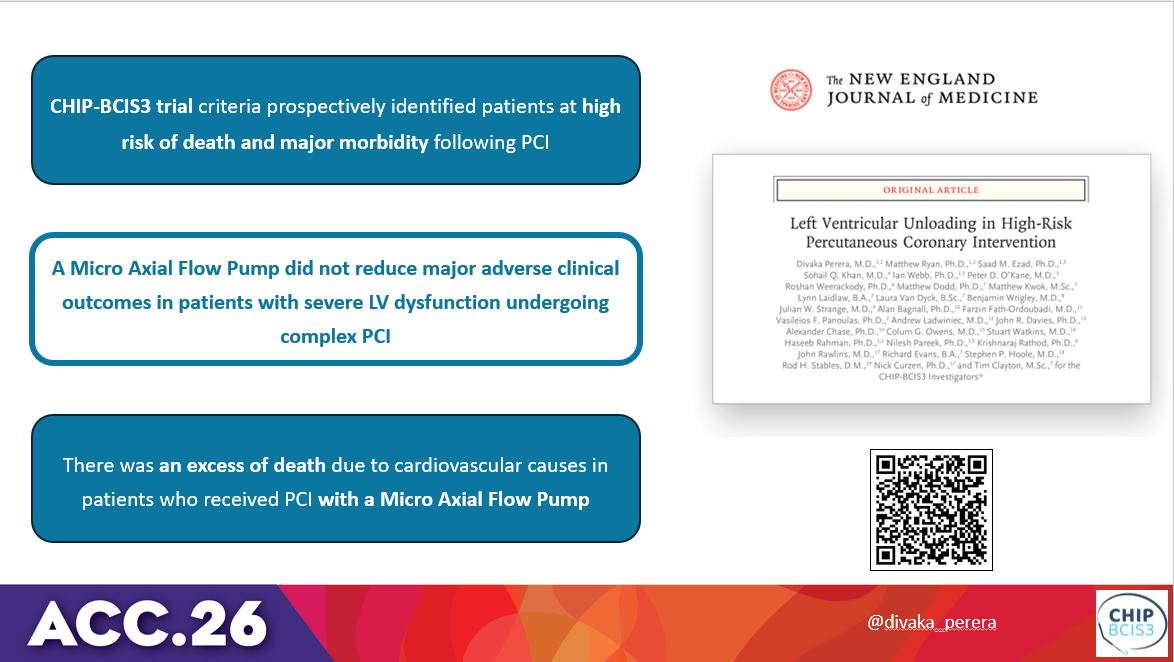
CHIP-BCIS3 trial: Percutaneous LV unloading with microaxial flow pump did not reduce major adverse clinical outcomes vs. standard of care in patients with severe LV dysfunction undergoing complex PCI. #ACC26 View the slides here: https://t.co/ylmrlzroTj
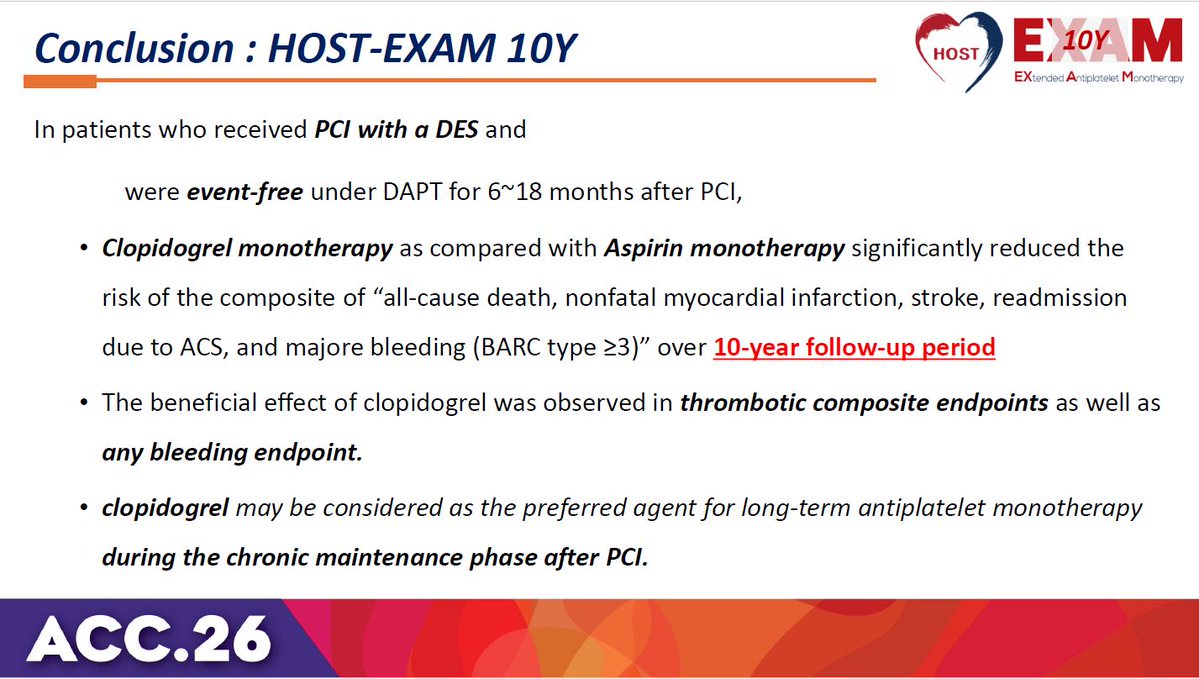
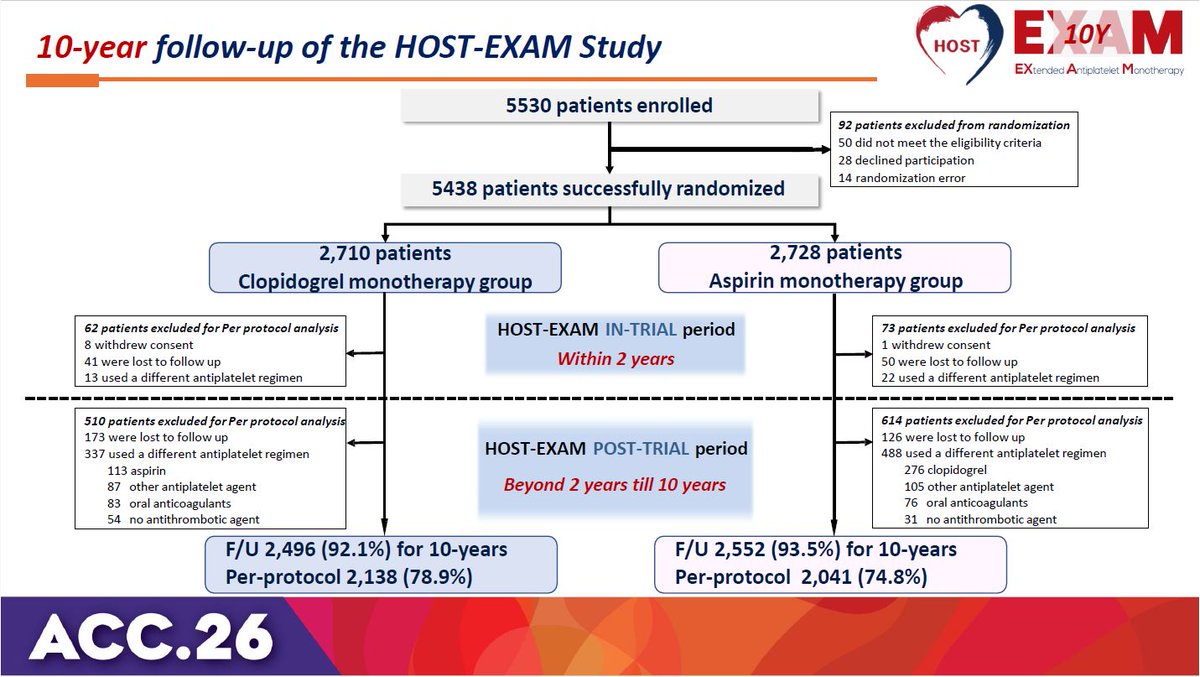
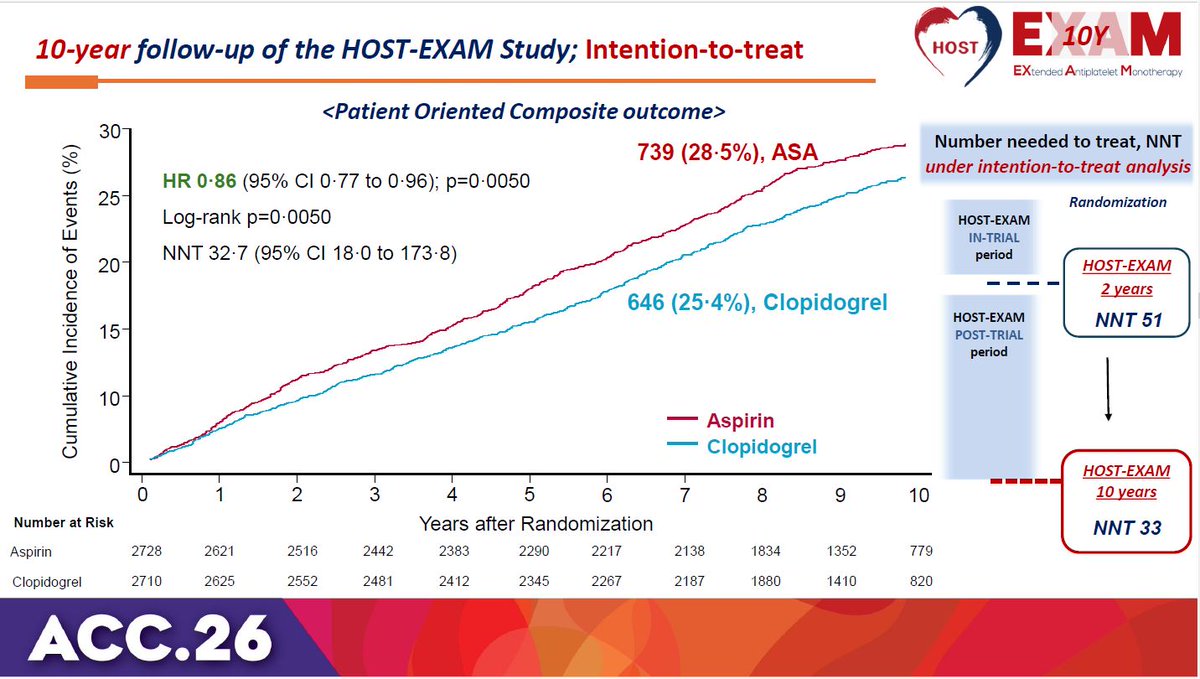
HOST-EXAM trial 10-year results: Clopidogrel monotherapy is superior to aspirin for chronic maintenance after PCI, significantly reducing both thrombotic and bleeding events. #ACC26 View slides here: https://t.co/ihoudzlxIi
#acc26 Six reasons why CHAMPION AF should not change oral anticoagulation for AF
I will have a formal post up on @theheartorg but here is a short summary
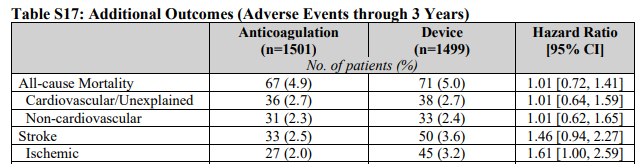
1) Stroke and Ischemic Stroke went the wrong way.
All S -> 33 vs 50 [HR 1.46 95% CI, 0.94-2.27)]
IS -> 27 vs 45; [HR = 1.61; 95% CI, 1.00-2.59)]
Look at those upper-bounds.
2) NI would not have been met for efficacy had they used a margin with both rate ratio and risk difference, which is standard practice.
The margin of 4.8% is based on event rates at 12%, which is 1.4 in relative terms (40% higher). But when event rates come in lower, as they did: 4.8% vs 5.7%, the 4.8% margin is too lenient.
The 0.9% higher rate of the primary endpoint has a 95% CI of (-0.8-2.6%), so 2.6% is less than the margin of 4.8%. Now do it with relative risk.
It's in table 2. The relative risk is 1.20. The 95% confidence intervals were 0.87-1.66. Note that 1.66> 1.40 so LAAC is not noninferior based on rate ratio margins
3) The primary safety endpoint is flawed because it excludes periprocedural bleeding and uses nonmajor bleeds, such as gum bleeds and bruising. It's open label trial so who which group will complain of more nonmajor bleeding?
4) When counting all events, Watchman barely reduced major bleeds. Also in the main results table is that major bleeds were 83 vs 87 (5.5% vs 5.8%; HR 0.92 95% CI 0.68-1.24)
5) Net Clinical Benefit was also flawed because they used nonprocedural bleeding and nonmajor bleeds.
A normal patient would simply say, there were 17 more strokes and only 4 less bleeds. Hardly a good trade.
6) Bayes: trials don't give answers, they update priors. For Watchman, you have PREVAIL failing against warfarin, CLOSURE AF clearly failing against best med Rx (mostly DOACs) so priors are pessimistic. To go from pessimistic priors to enthusiastic posteriors you'd need hugely positive data. CHAMPION is not that.
Don't believe the stories that CLOSURE failed due to them using other LAAC devices. In the AMULET IDE trial, Watchman and Amulet were similar. Also, if you believe that German operators are worse than US authors, you need to travel more.
Conclusion: Oral anticoagulation for AF is one of the most evidence-based practices in all of medicine. To upend that would take much stronger data.
Don't be bamboozled by this trial, which was designed to be positive before the first patient was enrolled.
#ACC2026
@NEJM Why does the most critical data , 61% increased risk of ischemic stroke in the device arm, is hidden in supplementary table 17 ? This should be in the abstract , main figures and main tables.
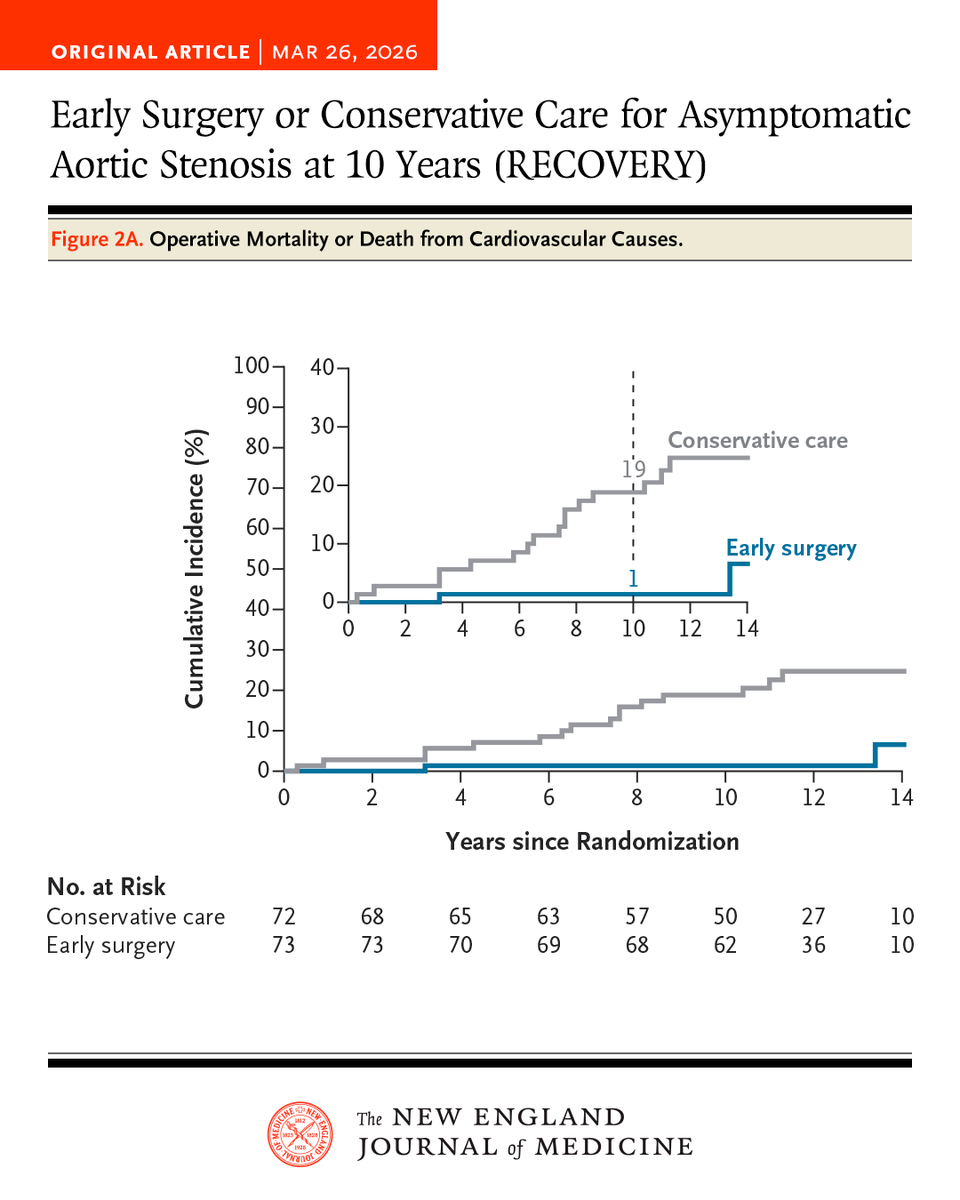
Early surgery in asymptomatic patients with very severe aortic stenosis led to a lower risk of a composite of operative mortality or death from cardiovascular causes at 10 years than conservative care. Full RECOVERY trial results: https://t.co/tLqC25ccCJ
I hope no one needs an MRI this year.
The world's largest producer of liquified helium is in Qatar and is shut off. We just got a notice that our supply for the year will be at least cut in half.
No one could have predicted this (unless they thought about it).