Enzalutamide with or without leuprolide in patients with high-risk biochemically recurrent prostate cancer: EMBARK post hoc analysis by age
https://t.co/v4CM6kWiJU
The post hoc age-stratified analysis of the EMBARK trial found that enzalutamide, with or without leuprolide, improved metastasis-free survival in patients with high-risk biochemical recurrence of #ProstateCancer regardless of whether they were younger than 70 or 70 and older.
Although older patients were more likely to have higher baseline PSA levels and to have received prior radiotherapy, they showed similar efficacy benefits from treatment.
@nealshore@UgoDeGiorgi@MatkoKalac@MelissaJHuynh@CarcanoMD@SFreedlandMD@OncoAlert 🚨
@Silke_Gillessen@AOmlin@weoncologists
Enzalutamide with or without leuprolide in patients with high-risk biochemically recurrent prostate cancer: EMBARK post hoc analysis by age
https://t.co/v4CM6kWiJU
A post hoc analysis of the EMBARK trial examined whether age influenced outcomes with enzalutamide ± leuprolide in patients with high-risk biochemical recurrence of #ProstateCancer , finding that both younger (<70 years) and older (≥70 years) patients experienced meaningful improvements in metastasis-free survival compared with leuprolide alone. Although older patients entered the study with somewhat higher-risk disease characteristics and experienced a higher incidence of adverse events—including more grade ≥3 events—treatment-related serious adverse events remained uncommon across all groups.
Overall, the efficacy of enzalutamide-based therapy was consistent regardless of age, with safety differences largely attributable to increased vulnerability in the ≥70-year cohort.
@nealshore@UgoDeGiorgi@MatkoKalac@MelissaJHuynh@CarcanoMD@SFreedlandMD@OncoAlert 🚨
@Silke_Gillessen@AOmlin@weoncologists
Viewpoint: Recognizing the heterogeneity of small cell lung cancer, efforts are underway to apply precision oncology through molecular subtyping and targeted therapies for tailored treatment. https://t.co/T2vJIoLSHt
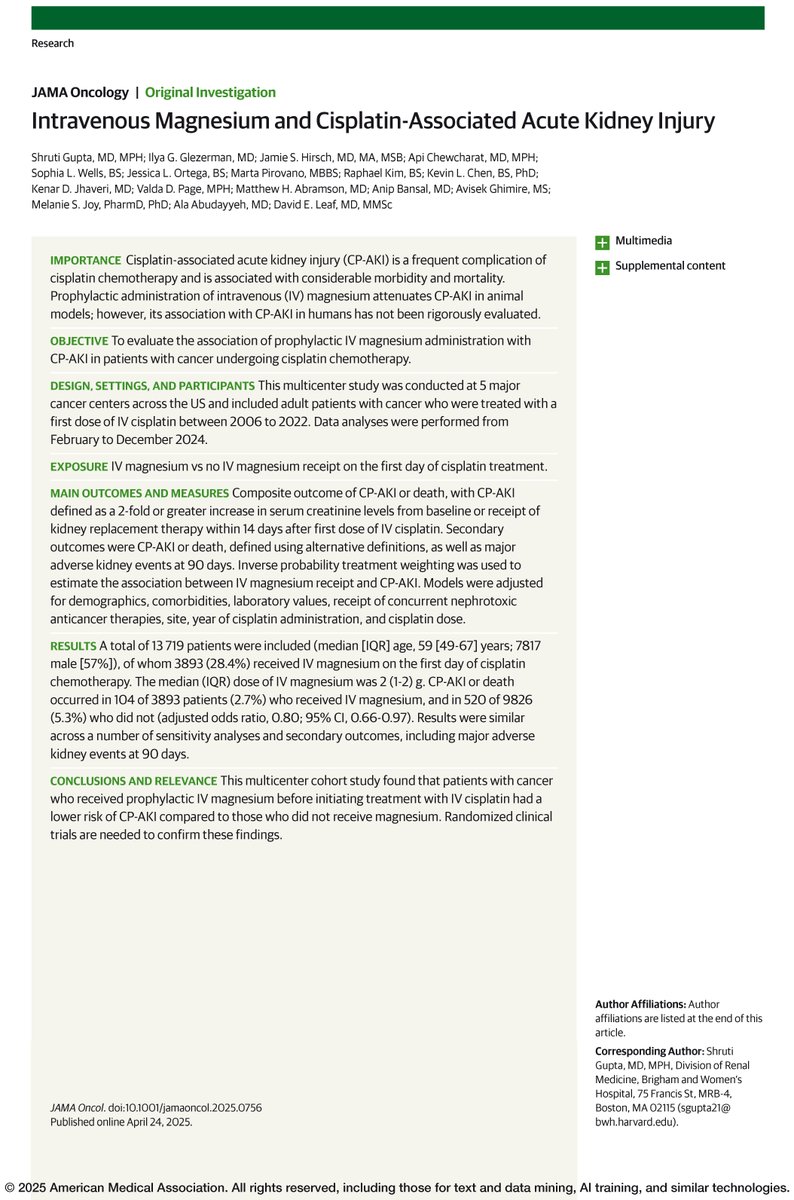
Prophylactic IV magnesium administration was associated with a lower risk of cisplatin-associated acute kidney injury (CP-AKI) in patients with cancer undergoing cisplatin chemotherapy. https://t.co/Al9FpH395g
🚨 Wow! #ASCO25@ASCO was absolutely massive!
10 @NEJM papers published simultaneously 👉 all practice-changing studies ! 🔬✨🧵 See below for these studies 👇@oncoalert
Intratumoral heterogeneity drives therapy resistance in metastatic #ProstateCancer. @laurasenamd@hopkinskimmel joins @AndreaMiyahira@PCFnews discussing a detailed analysis of a patient's disease progression over seven years, Dr. Sena demonstrates how distinct cancer cell populations within the primary tumor led to treatment resistance through clonal selection rather than adaptation. #WatchNow > https://t.co/re6KTz81Uf
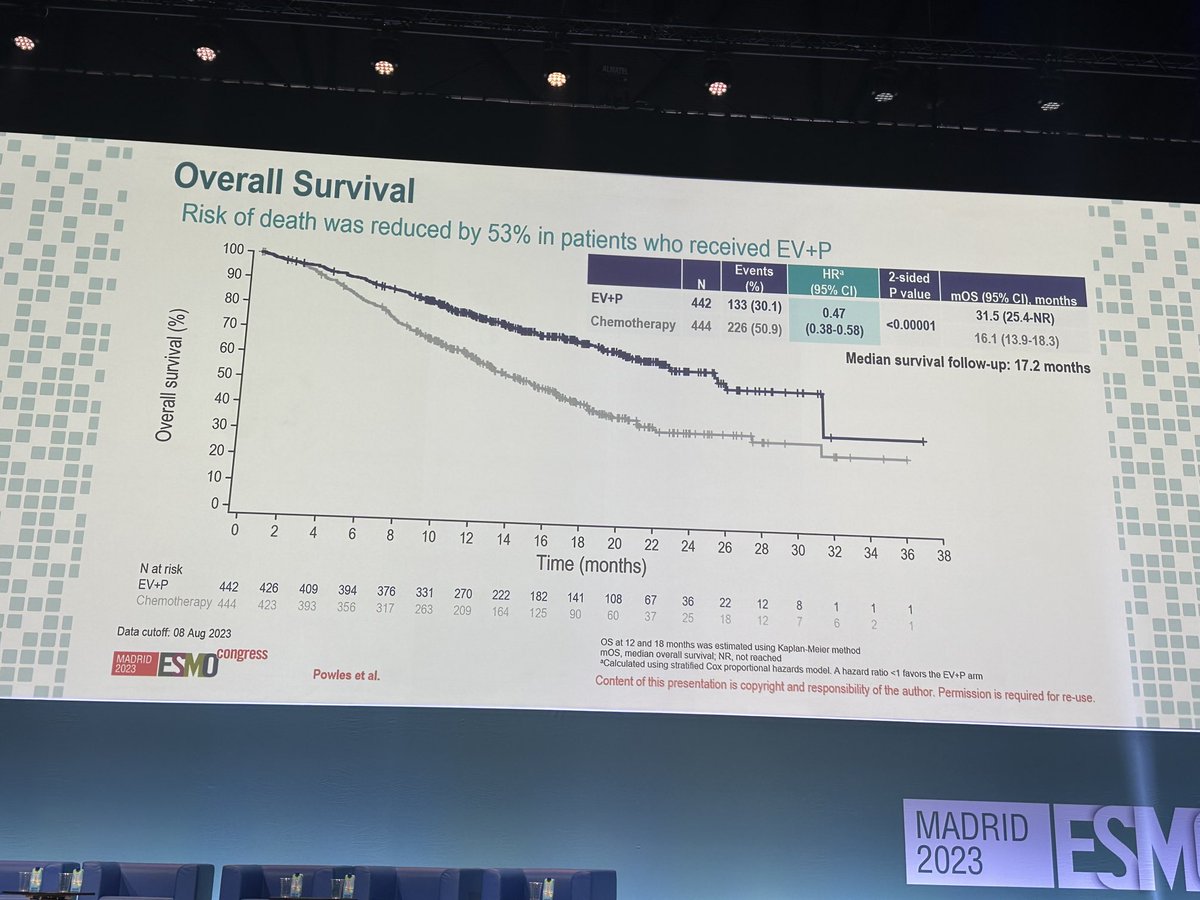
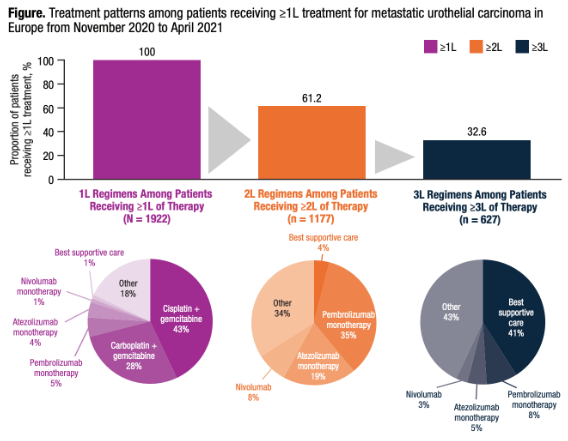
🇪🇺 Real-world treatment of metastatic urothelial carcinoma (mUC) in Europe shows persistent gaps vs evolving guidelines.
📉 41% receiving 3L therapy got only supportive care
🧪 Few patients received 1L PD-1/L1 inhibitors
📊 Newer regimens like EV+P not yet reflected
More data needed to bridge evidence-to-practice.
#AuthorCommentary from Torsten Strunz-McKendry, PhD @AstellasEurope > https://t.co/yOROTyfHJI
The Future of ADCs in #ProstateCancer
Dr. John Lee @UCLA reviews the challenges & progress of #AntibodyDrugConjugates:
�� Early ADCs failed due to antigen heterogeneity (PSMA volatility)
🔬 Hope in new agents: ARX-517 (auristatin payload) & FOR46 (CD46-targeted) show promise
🎯 Next-gen ADCs explore dual targets (PSMA + STEAP-1) & synergistic payloads
Exciting innovations ahead! #ReadNow > https://t.co/MvpoJKtXEB @PSMAconference 🔬 #PSMAandBeyond2025
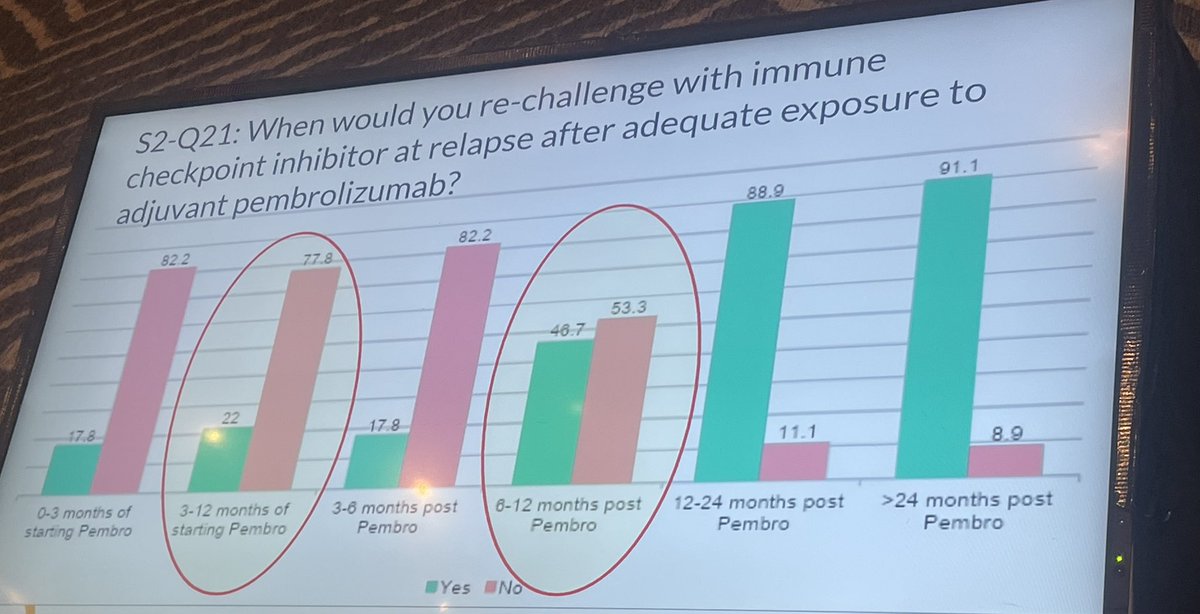
When to rechallange with PD1 therapy in advanced RCC after progression on/after adjuvant pembro #AUC3 ? Rechallange studies in advanced disease (CONTACT3) have been negative. However the group conclusively support rechallange after a gap of a year since adjuvant pembro.
KEYNOTE 564 is huge. 38% OS difference which solidifies pembro’s position in the adjuvant setting. In the placebo group 70% of pts had subsequent IO which is good. M0 subgroup is significant on its own as well. Impressed! @ASCO@Oncoalert@Merck#GU24
Constant TKI is NOT necessary in IO/TKI regimens. We need to prioritize strategies to de-escalate therapy for better QOL and possibly delaying resistance. Congrats to @DrIacovelli and the team for this important work.
FDG-PET CT is widely used in NMIBC. @kalasri3@uromigos investigator led study showed in a randomised trial it didn’t change practice or outcomes. I’m going to stop using PET in MIBC it delays and complicated things without clear benefit. #ESMO23
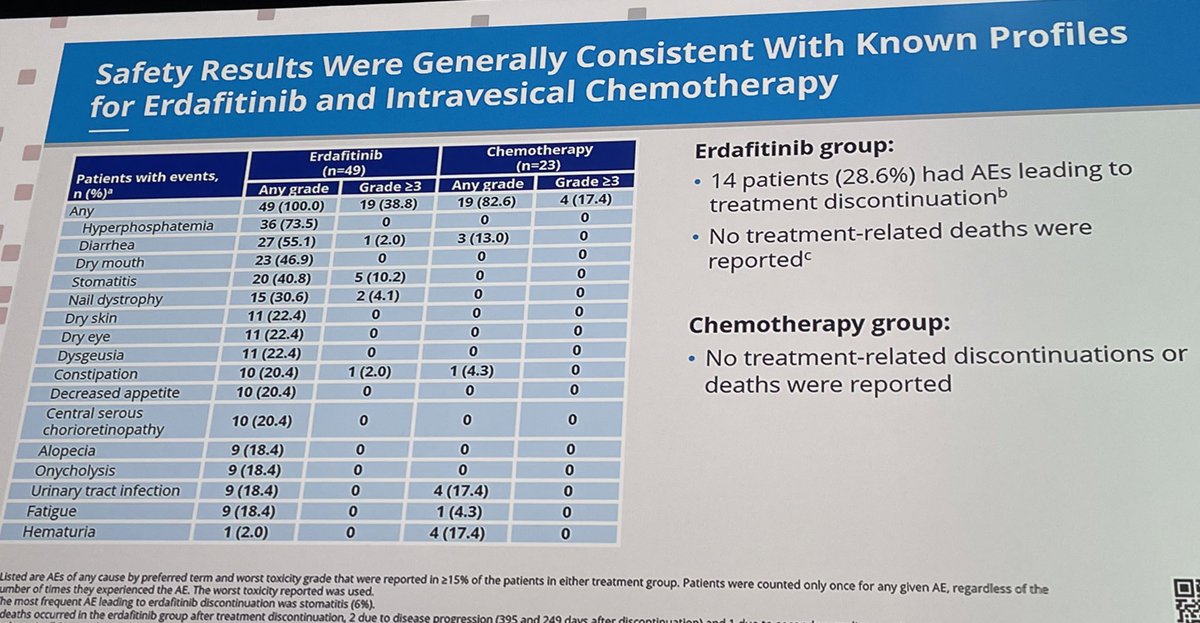
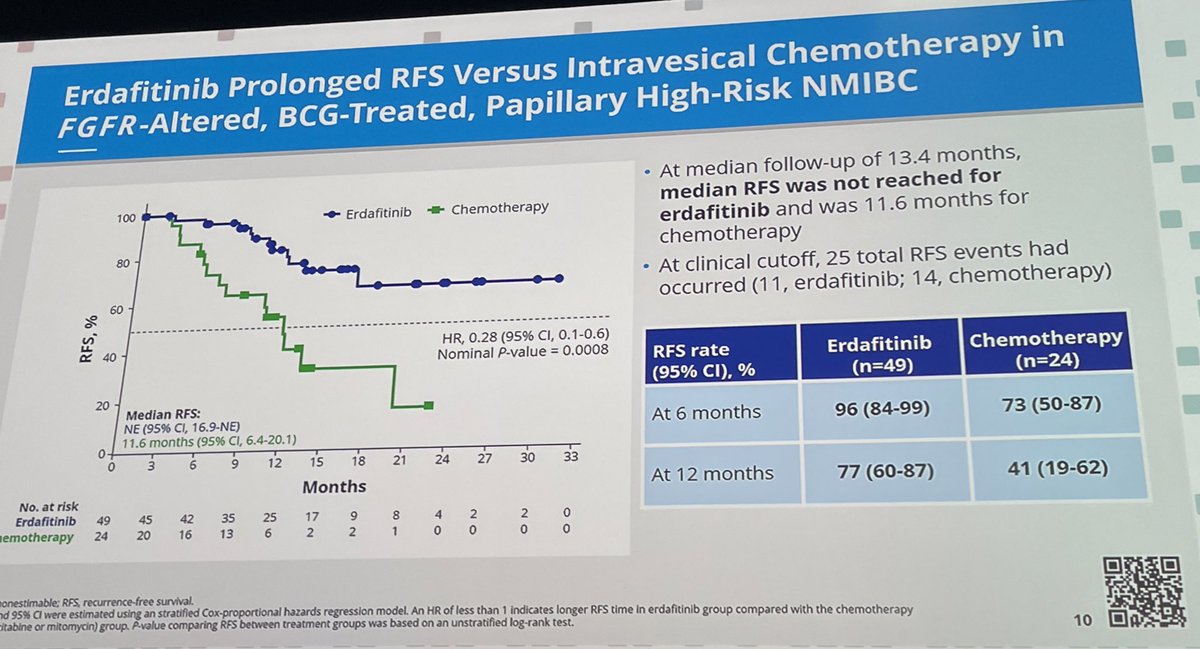
#ESMO23 THOR-2 data were brilliantly presented by @JimCatto
Huge and significant data with erdafitinib in NMIBC with FGFR2/3
mut/fus tumors that failed to prior BCG.
📌 A major issue: only 76 of the 240 pre-planned patients were recruited
Would it be enough to change practice? 🤔
@OncoAlert@myESMO@urotoday@GuardConsortium
Belzutifan vs everolimus in pretreated RCC #ESMO23: 25% ⬆️ in PFS, OS HR = 0.88 (95% CI 0.73-1.07) with RR=23% vs 3% & 25-45% ⬆️ in time to ⬇️ QOL. Tox of note: hypoxia. This looks attractive in VEGF/IO refractory disease instead of evero. Combos earlier in the disease awaited.
Oral EPI-7386 monotherapy in patients with #mCRPC. @RPachynski@WUSTLmed joins @CaPsurvivorship@DanaFarber to discuss this first-in-class N-terminal domain AR inhibitor that suppresses androgen activity through a novel mechanism of action > https://t.co/1V8Caa6lVK @EssaPharma