The ctDNA hype cycle is over.
ASCO’s first ctDNA guideline tells us where liquid biopsy actually changes practice. 🧬
✅ Use ctDNA when:
• Tissue is unavailable or unsafe
• Results are needed urgently
• Drug approvals allow/require liquid biopsy
⚠️ Negative ctDNA does NOT exclude actionable disease.
Tissue confirmation remains critical.
Practice-changing trials cited by ASCO:
🔹 DYNAMIC
Stage II colon cancer
Less chemotherapy, same outcomes.
🔹 PADA-1
ESR1-guided switch to fulvestrant + palbociclib improved PFS.
🔹 SERENA-6
ctDNA-detected ESR1 mutations enabled earlier intervention and significantly prolonged PFS.
🔹 IMvigor011
MRD-positive bladder cancer benefited from adjuvant atezolizumab.
❌ ctDNA should not replace imaging, pathology, or standard staging.
Bottom line:
The question is no longer:
“Can we detect it in blood?”
The question is:
“Will acting on it improve outcomes?”
That’s the bar ASCO has set. 🎯
#Oncology #ctDNA #LiquidBiopsy #ASCO #PrecisionMedicine
@OncoAlert@ASCO@JCOPO_ASCO
CONGRESS | #EHA2026 | PRESENTATION
Eugen Tausch presents the final 5-year biomarker analysis of the phase III GAIA/CLL13 trial evaluating genetic predictors of efficacy with venetoclax-based regimens — rituximab + venetoclax (RV), obinutuzumab + venetoclax (GV), and obinutuzumab + ibrutinib + venetoclax (GIV) — vs chemoimmunotherapy (CIT) in fit patients with previously untreated CLL (N = 913).
At a median FU of 63.8 months, U-IGHV was independently prognostic for PFS with both venetoclax-based regimens (HR, 2.01; p < 0.001) and CIT (HR, 3.55; p < 0.001). With venetoclax-based regimens, complex karyotype (HR, 1.93; p < 0.001), mutated NOTCH1 (HR, 1.56; p = 0.003), and mutated EGR2 (HR, 1.61; p = 0.036) also remained independent adverse prognostic factors for PFS. For CIT, complex karyotype also remained independently prognostic for PFS (HR, 1.69; p = 0.019). At relapse, acquired resistance mutations were rare, with BCL2 mutations in 1.2% after RV and no acquired BTK/PLCG2 mutations; TP53 mutation/del(17p) evolution occurred less frequently after venetoclax-based therapy vs CIT.
Follow our live feed for more updates: https://t.co/SucPqSTkNI
Intended for HCPs only. This congress coverage is independently supported by pharmaceutical companies, who are allowed no influence on the content; a full list of supporters can be found on our website.
#lymphoma #lymsm #MedicalCongress @uni_ulm
CONGRESS | #EHA2026 | PRESENTATION
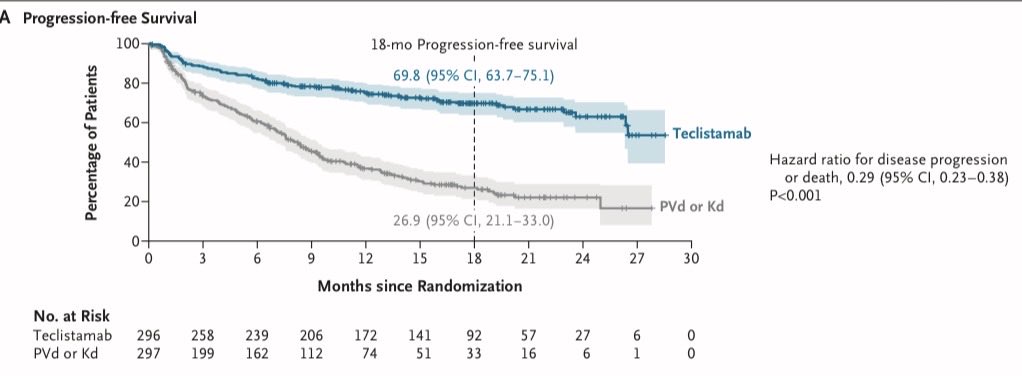
Cyrille Touzeau presents results from the phase III MajesTEC-9 study evaluating teclistamab monotherapy versus pomalidomide, bortezomib, and dexamethasone (PVd) or carfilzomib and dexamethasone (Kd) in patients with RRMM.
After a median follow-up of 17.3 months, median PFS was not reached with teclistamab versus 8.2 months with PVd/Kd (HR, 0.29; p < 0.0001). ORR was higher with teclistamab versus PVd/Kd (OR, 4.62; p < 0.0001). OS also favored teclistamab (HR, 0.60; p = 0.002). Infection rates were higher with teclistamab, including grade 5 infections (5.5% vs 2.8% with PVd/Kd).
Follow our live feed for more updates: https://t.co/IjiLwPfcB5
Intended for HCPs only. This congress coverage is independently supported by pharmaceutical companies, who are allowed no influence on the content; a full list of supporters can be found on our website.
#MultipleMyeloma #myeloma #mmsm #MedEd @CHUnantes
CONGRESS | #EHA2026 | PRESENTATION
Sonja Zweegman discusses regulatory approvals and novel trial endpoints in #MultipleMyeloma treatment development, highlighting how improved outcomes are reshaping trial design and decision-making.
With survival improving in MM, trials using survival endpoints may require long follow-up, delaying access to effective and potentially curative treatments and risking that comparator arms no longer reflect contemporary SoC at study readout. MRD was highlighted as a reasonably likely surrogate endpoint that can support earlier readout and conditional/accelerated approval, but trials should remain powered for PFS and followed for OS and QoL. MRD is prognostic for PFS/OS at the patient level and shows encouraging trial-level predictive value; however, further validation is needed, including optimal MRD timing, the role of sustained MRD-negativity, and whether PB-based assessment can complement BM testing. Earlier endpoints must not compromise long-term safety assessment, particularly for irreversible neurotoxicity, SPMs, and late/opportunistic infections. Patient preferences and PROs should also be embedded and monitored longitudinally.
Follow our live feed for more updates: https://t.co/IjiLwPfcB5
Intended for HCPs only. This congress coverage is independently supported by pharmaceutical companies, who are allowed no influence on the content; a full list of supporters can be found on our website.
#myeloma #mmsm #MedicalCongress @amsterdamumc
During induction chemo for AML, why do we give continuous IV cytarabine, instead of bolus dosing like in consolidation?
Cytarabine is a pyrimidine analog that inhibits DNA synthesis. The chemo kills cells that are undergoing active DNA replication, making cytarabine "S-phase specific". But leukemia cells are constantly in flux in the cell cycle. They are not all uniformly in the same cell cycle phase. In active AML, leukemia blasts are slowly entering S phase over days, and cell kill is enhanced when they are getting continuously exposed to IV cytarabine
Once patients achieve remission, we do high dose bolus cytarabine to consolidate that remission. Bolus dosing generates high peak plasma concentrations and elevated intracellular levels of cytarabine metabolites (Ara-CTP) to overwhelm resistance mechanisms that characterize residual AML. Bolus dosing produces high peak concentrations, but exposure is transient as plasma cytarabine has a short half life (10-15 min) due to rapid deamination
So continuous IV yields low peak concentrations but prolonged duration above effective concentration, vice versa for bolus.
Effectively, one should think of continuous IV and bolus dose cytarabine as TWO DIFFERENT DRUGS WITH RADICALLY DIFFERENT MECHANISMS OF ACTION!
🧬 Next-Generation Sequencing (NGS) has revolutionized modern oncology.
From identifying actionable mutations and tumor-agnostic biomarkers to detecting minimal residual disease (MRD) and resistance mechanisms, NGS is the cornerstone of precision cancer medicine.
🎯 What can NGS detect?
✅ EGFR, ALK, ROS1, RET, NTRK alterations
✅ MSI-H & TMB-high biomarkers
✅ Germline mutations (BRCA1/2, TP53, PALB2)
✅ MRD and ctDNA
✅ Resistance mutations such as EGFR T790M
💡 Remember: TARGET MRD
🔹 T – Targetable mutations
🔹 A – Agnostic biomarkers
🔹 R – Resistance mechanisms
🔹 G – Germline mutations
🔹 E – Evaluation of prognosis
🔹 T – Tissue of origin
🔹 M – MRD detection
🔹 R – Recurrence monitoring
🔹 D – Drug selection
Precision oncology is shifting treatment decisions from “where the cancer started” to “which molecular alteration is driving it.”
#NGS #PrecisionOncology #CancerGenomics #MedicalOncology #MolecularOncology #LiquidBiopsy #ctDNA #MRD #TargetedTherapy #Immunotherapy #GenomicMedicine #CancerEducation #OncologyTraining #OncologyPearls #DrRupamManna #CancerConceptsExplained
🗓️ #WorldMSDay takes place on 30 May. 🌍 In this recent article, we explore how aHSCT has transformed care for people living with multiple sclerosis (MS).
From registry research to emerging cellular therapies, discover how collaboration and innovation continue to shape the future of MS care. 📖 Discover more: https://t.co/eS2CAXj8fq
#MS #MultipleSclerosis #HCT #CellTherapy
📊 A major milestone for the EBMT community: the 2024 EBMT Activity Survey has now surpassed 1 million haematopoietic cell transplants (HCTs) and 20,000 CAR-T therapies.
📖 Read the full Open Access Activity Report in @BMTjournal: https://t.co/5PdnLNM8SD
This landmark report reflects the strength of collaboration, the evolution of cellular and gene therapies, and the growing impact of our data in shaping clinical practice and research worldwide. 🌏 Thank you to all contributors across the community! 🙏
Authors 👤 @RaffaellaGrecoM, @IsaSchezOrtega, Antonio Risitano, @krzysztofkalwak, @AnnalisaRugger1, Iliana Kleovoulou, Marina Atlija, Tobias Alexander, Emanuele Angelucci, @AverbuchDina, Ali Bazarbachi, Maria Ester Bernardo, Charles Crawley, @MetteHazenberg, Olaf Penack, Helen Baldomero, @passweg, @i_yakoub_agha, @DonalMcLor, @CiceriFabio, @AnnaSureda5
#HCT #CARTtherapy #CellTherapy #GeneTherapy #CommunityMilestone
A standard serum B12 test can appear normal while the body is actually functionally deficient at the cellular level. Two deeper markers reveal the truth:
•Homocysteine
•MMA
Even with levels nearly 3× above the deficiency cutoff, functional deficiency is still possible
New publication 📝 5-year follow-up results from the ZUMA-2 trial, published in the Journal of Hematology & Oncology, show brexu-cel produced durable responses in R/R MCL, with a median DoR of 36.5 months.
Learn more: https://t.co/DNvS3ZXgX6
#lymsm#MedNews#MedEd
New issue of Blood out now featuring CD117-targeted HCT preconditioning in AML and MDS, CSNK1E as a key to unlocking drug persistence in DLBCL, Novel functions of WPB proteins seem to cluster with VWF and more. Explore here: https://t.co/4NRWRoQeTD
Concomitant publication in @NEJM#ASCO26
BCMA bispecific moves earlier in myeloma.
MajesTEC-9 | NEJM 2026
Teclistamab monotherapy vs PVd/Kd in RRMM after 1-3 prior lines, all exposed to anti-CD38 + lenalidomide.
🧬 18-mo PFS
69.8% vs 26.9%
HR 0.29
🫀 18-mo OS
79.2% vs 68.6%
HR 0.60
🎯 CR or better
65.9% vs 16.8%
But the price is real:
Grade 3/4 infections 41.6%
CRS 66%, mostly grade 1-2
ICANS 4.1%
Takeaway:
Teclistamab is no longer just a late-line rescue story.
Early BCMA targeting is becoming a serious relapse strategy - but infection prevention is not optional.
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #MultipleMyeloma #Myeloma @OncoAlert@myesmo@esmo_open