Great to hang out with my Western Canadian GI Oncology colleagues last weekend for our 27th Annual #WC5 Consensus Meeting in #Calgary 🤗
Lots to discuss in CRC this year - CHALLENGE, ALASSCA, ATOMIC, 8HW & BREAKWATER…
➡️ important to contextualize how this data will help our pts 🇨🇦
The most practice changing trial from #ASCO25 is now live on @NEJM .If this was a drug, this would be approved today. Globally relevant and low-cost intervention that is not only delaying relapse but actually improving survival.
Perfect case example of a #cancergroundshot trial.
https://t.co/ZnqeplJ7IA
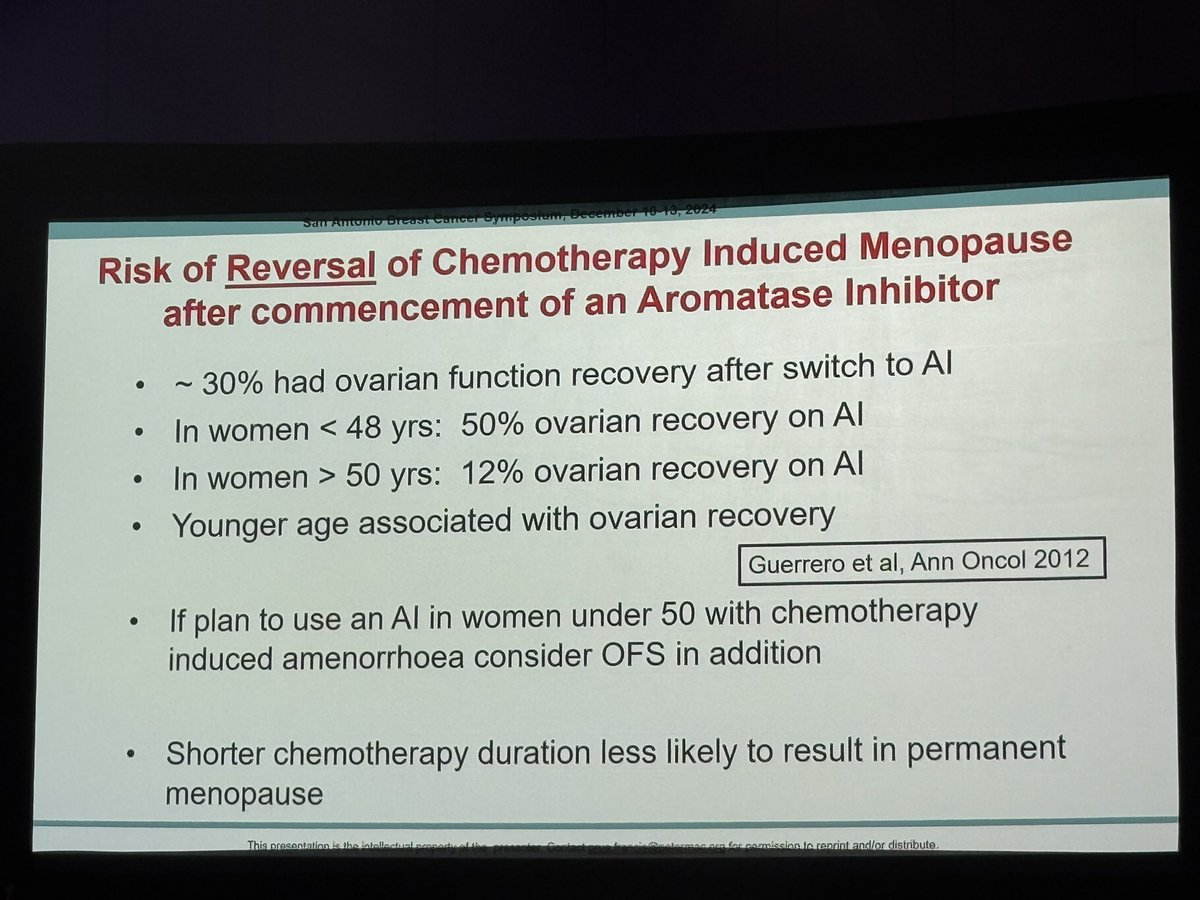
Don't underestimate risk of starting AI in people who were premenopausal before chemo and stopped having periods.
~30% (even after 2 years of amenorrhea) regained ovarian function when put on an AI.
@OncoAlert@SABCSSanAntonio#SABCS24#bcsm
This thread by the AMA does a great job of articulating the challenges for cancer care across Canada. These challenges are not unique to Alberta. Would love to see similar advocacy here in Manitoba!
Why is there more need for cancer care?
Cancer rates are outpacing population rates. Reduced access to primary care, amid pandemic disruption to screening and prevention, means patients are often diagnosed with advanced cancer in overcrowded, underresourced emergency departments.
Technological innovations like genomic therapy can save patients who would not have survived a few years ago. This advanced development, however, adds a new population of complex patients requiring special care that only oncologists can provide for years after treatment.
Why is there more need for cancer care?
Cancer rates are outpacing population rates. Reduced access to primary care, amid pandemic disruption to screening and prevention, means patients are often diagnosed with advanced cancer in overcrowded, underresourced emergency departments.
Great discussions #NPC2023. As a med onc, how do you discuss with a PDAC patient:
- SOC treatments
- toxicity mgmt
- patient expectation on treatments
- PERT
- outcomes and prognosis
- NGS sequencing
- clinical trials
- palliative care
Is an hr enough time? @CraigsCauseCan
@supriyadwivedi@DavidWCochrane@sbrunetti I'm so sorry for what you experienced. Thank you for sharing. We need to hear this in this country. We need more palliative care services for patients with cancer & patients need this early, not just in the last days of life
And the gut shall lead them…
Well done GI oncology leading this discussion within NCTN. @JNCI_Now
Room Where It Happens: Addressing Diversity, Equity, and Inclusion in NCTN Clinical Trial Leadership https://t.co/AY8QOxhpgV
@aparna1024@PamelaKunzMD@NiuSanford@rachnatshroff
💯credit to @PamelaKunzMD@KarynAGoodman for leading this call for action 👏 & including representation from all NCTN #GIOnc groups @CDNCancerTrials @j_lukovic
👉important recommendations to advance #DEI in clinical trials research
👉 will definitely explore this further within our 🇨🇦 GI disease site
https://t.co/TEQBvg7q35
Agree! Thank you to Rebecca Snyder for your leadership on this manuscript & thank you to @PamelaKunzMD & @KarynAGoodman for your leadership on this task force. An inspiring community
All kudos to Rebecca Snyder for leading this paper, & @PamelaKunzMD & @KarynAGoodman for putting together the NCTN Task Force.
Also props to @TedHong9 & @TGeorgeMD, NRG GI co-chairs, for giving opportunities to junior faculty and welcoming diverse ideas.
All kudos to Rebecca Snyder for leading this paper, & @PamelaKunzMD & @KarynAGoodman for putting together the NCTN Task Force.
Also props to @TedHong9 & @TGeorgeMD, NRG GI co-chairs, for giving opportunities to junior faculty and welcoming diverse ideas.
NRG GI Committee members @hitchcock_kate & @NiuSanford were part of an independent NCTN Task Force for Diversity in GI Oncology & contributed to this paper focused on increasing opportunities for women in leadership of NCI-sponsored GI cancer studies:
https://t.co/fwffuOGxT0