@mouseter_chef@DocEd We do use etomidate often for emergent RSI in the US, but it really isn't so bad! It works quickly, generally has minimal hemodynamic effect, and the adrenal suppression is treatable. Ketamine is better with very experienced team, but need to be very careful with dose. @K2Pharmer
@Core_EM Important to note that blood is most commonly seen between the spleen and the diaphragm in LUQ +FAST views, as in this case. Look carefully above the spleen along the entire diaphragmatic surface in the LUQ. This is different from the expected location of blood in the RUQ views.
@DenverEMed If you have to use IV benzodiazepines for agitation in an elderly patient, use a waaayyy lower dose than you would normally think of. For IV midazolam, I start with 0.5-1 mg, and wait several minutes before even considering trying more than that.
Beers Criteria recommends avoiding anticholinergics, antipsychotics, and benzodiazepines in the elderly. So what do we do when faced with an agitated elderly patient?
#EMConf
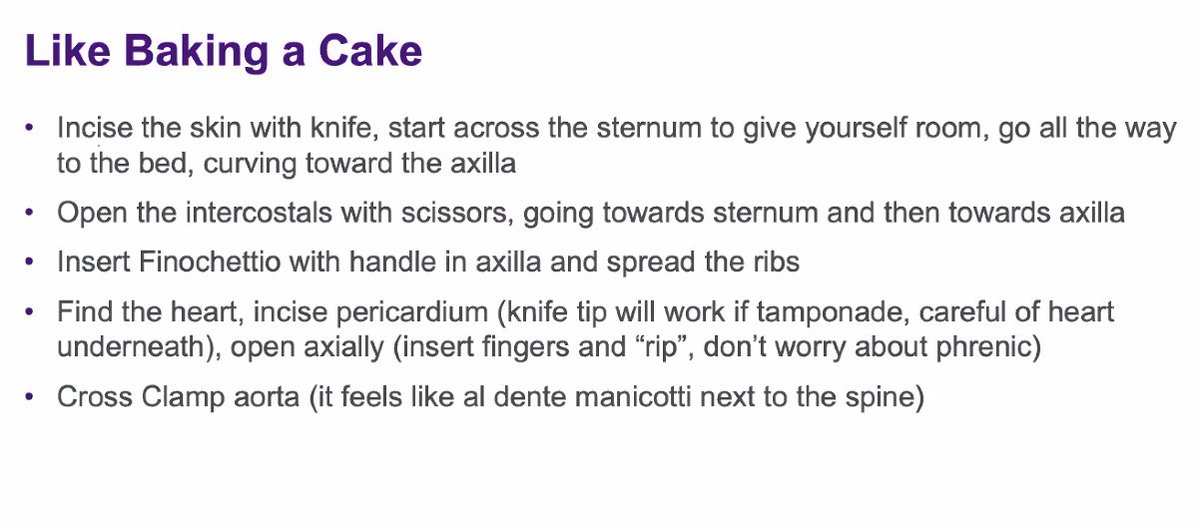
Chest Trauma by our @NYULangoneBK Trauma Surgeon @AlexSchwed
-in tension physiology PTX - first focus on relieving the pressure w/ finger thoracostomy
-no benefit for larger size of chest tube
-very reasonable to use pigtail in hemothorax
@Jonesy_MA The paper suggests that the pulse oximeter in its current design may be inadequate for detection of hypoxemia in our black patients. Occult hypoxemia in the paper meant an arterial oxygen saturation of <88% despite an oxygen saturation of 92 to 96% on pulse oximetry.
Phenomenal PGY4 Grand Rounds with Dr. Sobolev, encouraging use to embrace our creative side in emergency medicine and finding outlets to share #narrativemedicne
Dr. Shar Johnson on Blunt Abd Trauma in Pregnancy:
-Look out for domestic violence
-US has lower sensitivity, CT if you are concerned
-meds dose similar. If pt at risk for early deliver, start steroids!
-be prepared for perimorterm C-section
#emconf
Pelvic Trauma with Dr. Savan Patel
-BP <110 and increased base deficit are both associated w/ increased mortality in trauma
-large practice variability in REBOA use based on trauma center location
-don't forget the GU/pelvic exam!