Diagnosis of Acute Aortic Syndrome in the ED: An observational cohort study of people attending the ED with symptoms consistent of Acute Aortic syndrome (AAS)
The @dashedstudy team are in the process of preparing a grant application for a trial comparing strategies for investigating Acute Aortic Syndrome (AAS) in the ED. If you are a UK ED and interested in being a recruiting site, please email [email protected] for further information
High-sensitivity troponin has transformed MI detection, but front-door loading and unselective testing risk overdiagnosis & missed pathology. Our @EJ_EmergencyMed viewpoint article out today argues for reclaiming clinical reasoning in ED chest pain care https://t.co/h9ggpzYiUv
🚨 Emergency Medicine Journal Club Acute Aortic Syndrome: Can decision rules help diagnosis?
Join us for a discussion of the DAShED study, chaired by Prof. Gordon Fuller 🧠
🗓️ 30th Sept | 🕑 2–3pm
🔗 Register: https://t.co/Xwru2qOAi9
Delighted our ASES study summary ‘Diagnostic strategies for suspected acute aortic syndrome; systematic review, meta-analysis, decision-analytic modelling & value of information analysis’ has been published in the @NIHRresearch HTA journal; download here: https://t.co/08LeNS4xnA
Great to see @dashedstudy is the paper of choice for the next meeting of the new UK emergency medicine journal club on the 30th September at 2pm on Zoom, focussing around diagnostic approaches to acute aortic syndromes presenting to ED. Register here https://t.co/Xwru2qO2sB
Case-control designs show high bias resulting in inaccurate estimates and lack of representativeness of test accuracy when applied in a clinical setting
Our ASES study also shows that diagnostic biomarkers for AAS, other than D-dimer, are not ready for routine clinical use. Large cohort studies are required to evaluate multiple biomarkers in an appropriate population with suspected AAS; https://t.co/wx6M30QrZm
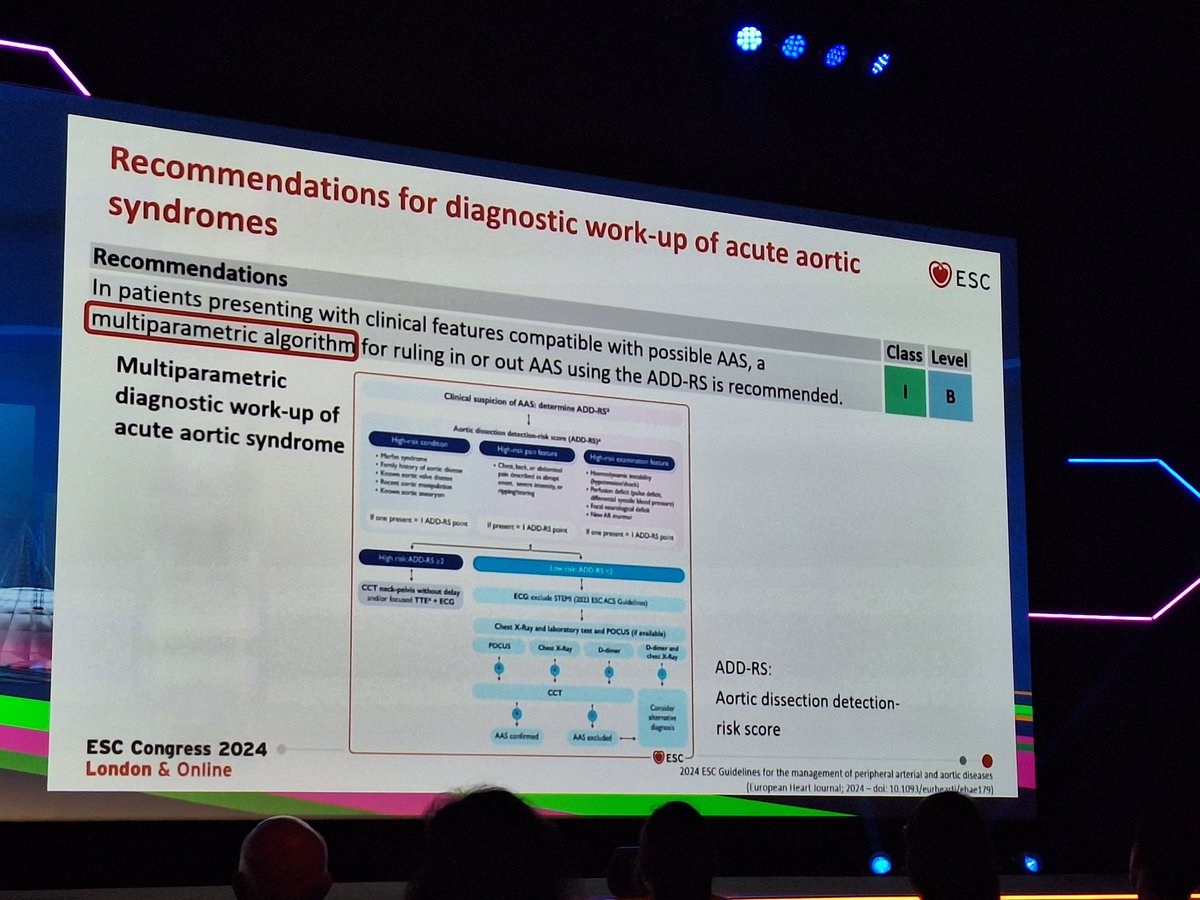
Our ASES decision analytical modelling of strategies for investigating suspected AAS shows that a strategy based on the Canadian clinical practice guideline using ADD-RS>1 or ADD-RS=1 with raised D-dimer to select patients for CTA appears cost-effective https://t.co/JGWL7wxW8d
I suggested a strategy based on D-Dimer & ADD-RS/Canadian will probably reduce the number of CTAs, be cost-effective & not lead to increased missed AAS but that a properly designed & funded implementation study is now required to provide clinicians with a safe effective strategy
What is the evidence around diagnosing Acute Aortic Dissection in the ED? At @EuropSocEM #eusem2024 I summarised the results of DAShED, ASES & PROFUNDUS. Here is a copy of my presentation; https://t.co/Ats8tole5K
Catch up on the review of the @dashedstudy and get a sneak peek into DAShED2. Learn how this phase addresses what to do once #aorticdissection is considered but a CT scan isn't absolutely necessary. The recording is now available. #AortaEd https://t.co/AoBPLlWuGO
A great summary of the NIHR funded ASES study from Professor Steve Goodacre with insight from Valerie Lechene, an aortic dissection survivor who participated in the research
#OriginalResearch#March2024
Diagnosis of Acute Aortic Syndrome in the Emergency Department (DAShED) study: an observational cohort study of people attending the ED with symptoms consistent with acute aortic syndrome
https://t.co/pICeT8OsrJ
@mattreed73@emerge_research
We definitely need to sort out the question of what you do once you ‘think aorta’ when the patient doesn’t absolutely need a scan (2.5% in DAShED) because we cannot CTA everyone - DAShED2 is in preparation and will attempt to answer this key clinical question
@davehartin It’s worse than that @davehartin the @dashedstudy showed us that there are no ‘good’ screening tests, including gestalt to spot the diagnosis
Simply thinking aorta won’t work
More here at @stemlyns
https://t.co/RqMDdu4EgP