🫀 Septic shock is not just about pressure. It’s about coupling.
We often treat septic shock with a familiar mindset:
➡️ Fluids
➡️ Vasopressors
➡️ Maybe inotropes
But we rarely ask the deeper question:
👉 Is the heart actually working efficiently with the arterial system?
⚙️ Enter: Ventriculo-arterial coupling (LVAC)
LVAC = Ea / Ees
• Ea → arterial load
• Ees → ventricular contractility
➡️ This ratio reflects how efficiently energy is transferred from the heart to the circulation
🧠 Why this matters
The cardiovascular system is not just a pump.
It is an energy transmission system.
From the pressure-volume perspective:
• Stroke work = useful energy
• Potential energy = wasted energy
• Total energy (PVA) ∝ myocardial O₂ consumption
👉 Efficiency depends on coupling, not just output.
📊 Key physiological insights
✔️ Optimal mechanical efficiency
→ LVAC ≈ 0.5
✔️ Maximal stroke work
→ LVAC ≈ 1
✔️ Septic shock
→ Often LVAC > 1 (uncoupling)
🚨 What happens in septic shock?
A complex mix:
• Vasodilation → ↓ Ea (sometimes)
• Myocardial dysfunction → ↓ Ees
• Microcirculatory chaos
• Variable preload
➡️ Result:
👉 Frequent ventriculo-arterial uncoupling
And here’s the key:
❗ Normal MAP ≠ optimal coupling
❗ Improved BP ≠ improved flow
💉 Therapeutic implications
Same MAP, different physiology:
🔵 Patient A
→ NE increases Ees > Ea
→ ↓ LVAC → ↑ SV (responder)
🔴 Patient B
→ NE increases Ea > Ees
→ ↑ LVAC → no SV improvement (non-responder)
🧬 Clinical reality check
Even more provocative:
• LVAC-guided resuscitation → faster lactate clearance
• BUT → no mortality benefit yet
And importantly:
👉 Optimizing coupling does NOT guarantee microcirculatory perfusion
🔥 Take-home message
We should move from:
❌ Pressure-driven resuscitation
To:
✅ Efficiency-driven hemodynamics
Because:
👉 The goal is not just to push blood
👉 The goal is to transfer energy effectively to tissues
📚 Caicedo Ruiz JD. et al. (2026)
Journal of Critical Care
https://t.co/1ZNMHqwBl4
Is continuous noradrenaline infusion the answer to preventing post-induction #hypotension? Does better haemodynamic stability translate to improved outcomes? This new trial explores these key issues. https://t.co/uPuthM9sDL
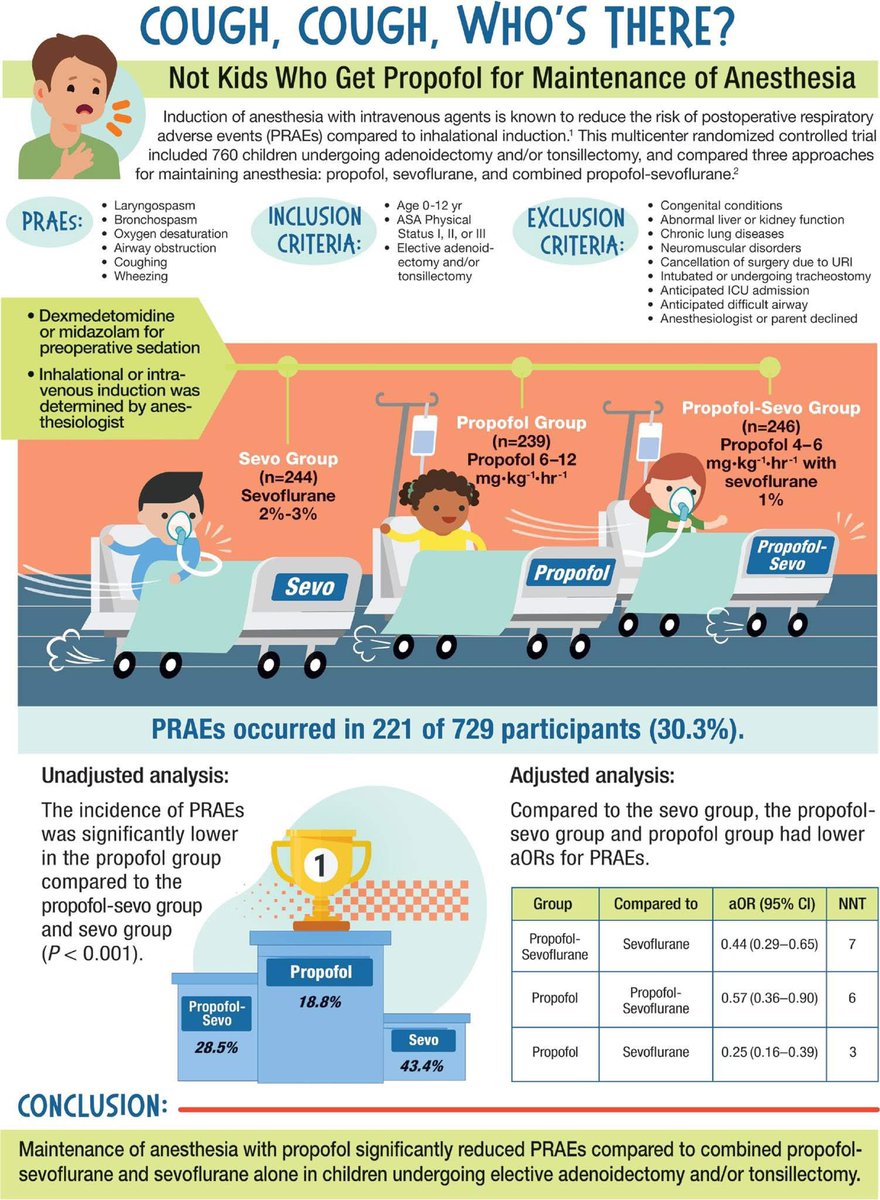
Tips for TIVA: amazing what's possible these days. sedation for brain MRI needed but no compatible pumps or shielded equipment available... No problem! iTIVA app and bolus method for TCI to maintain appropriate sedation level for 60mns☺️ everybody happy
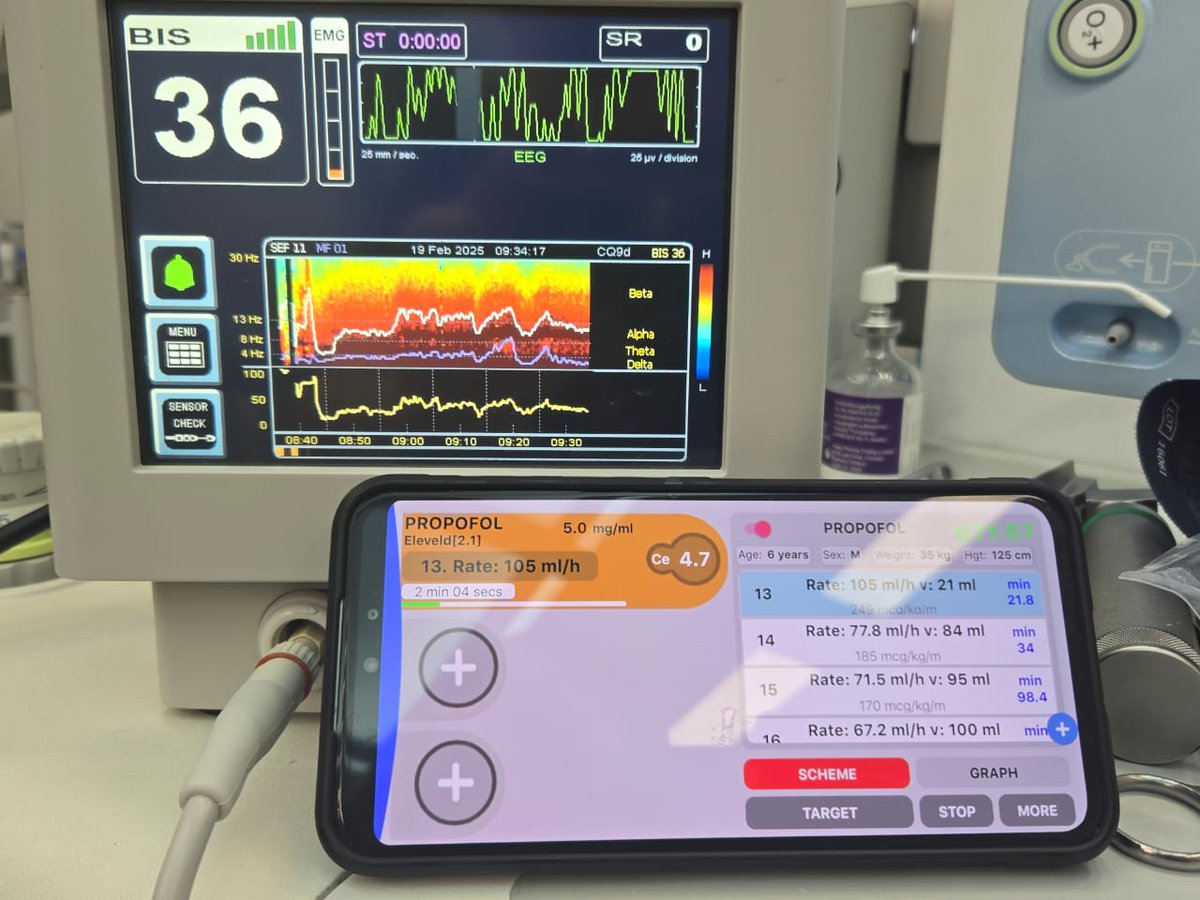
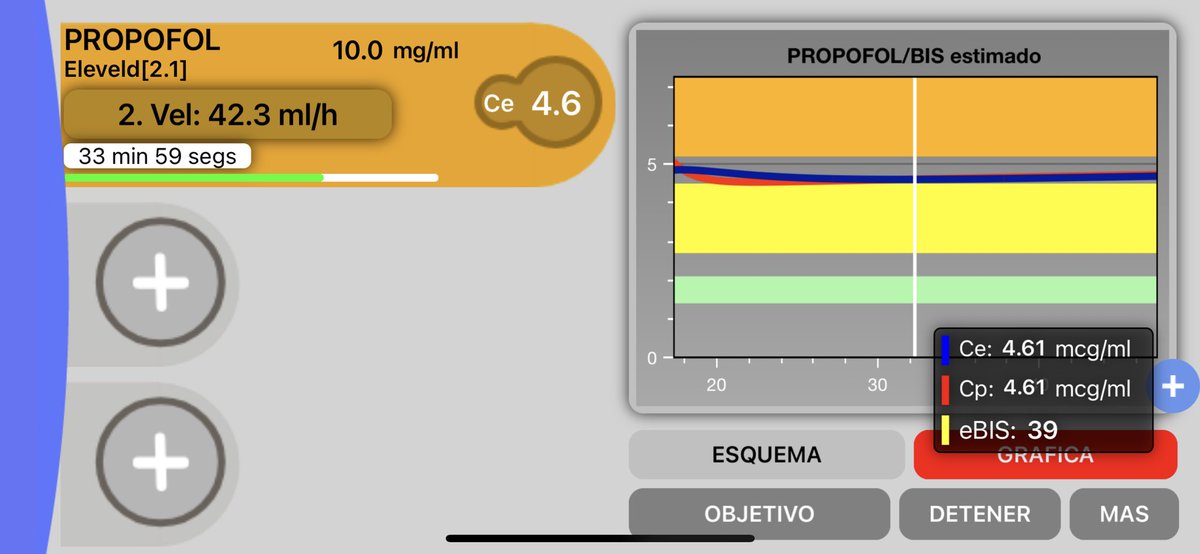
Tips for TIVA: Eleveld Excitement edition. No pump at moment with newer models, no problem! 6 years old for 2 hours...iTiva again but TCI MODE... Nice DSA on monitor as well. Titrating hypnosis to EEG feedback.
Using TIVA? Use Flows of 6L
In the UK flows of 6L are best for the environment and to save money.
This was a nice poster / infographic presented at SIVA a few years ago.
Have you started making your infographics? There's not long left!
@saraharuss Ouchy! Not happened recently but I’ve had this.
I’d suggest keeping the barrel of a 5ml syringe available (I know it’s a 2ml in the vid we did but 5 mls is the one to use)
https://t.co/pkjfkyRZCM
@nolittley@DrShmuk Yes, running the pump in ml/hr is the easiest way to update the infusion rate when using iTIVA, just check the syringe have the same concentration in the app. And in the app you can check the dose in milligram per kilogram