Some personal news.
Today, I’m leaving The Atlantic after almost 17 years and moving my writing to Substack.
It would be convenient, for the purposes of crafting an exciting departure announcement, to have a dramatic exit story: a fight, a grievance, a shouting match with an editor that ended with me hurling a bunch of leather-backed Thoreau volumes across the open-plan office. That is not the case here.
I love The Atlantic, and I'll remain a contributing writer there. But after almost two decades at one publication, I wanted to write for myself. The things I've published that I'm most proud of—whether it was the original abundance agenda essay, or my piece on workism—emerged from a very personal expression of frustration, or confusion, or curiosity. I want to know what my thinking and writing is like if I lean into a more independent and personal writing life.
That's brought me to Substack, which is already home to an astonishing share of my overall reading. I'm excited to join their community and excited to build my own. The name of the newsletter should be easy to remember: Derek Thompson.
The newsletter will have three main pillars
1. Abundance
2. The frontier of science and technology—GLP1s, AI, biotech, energy breakthroughs—covered in a way that’s both curious and skeptical
3. The anti-social century & the social crises of anxiety and aloneness
Thanks to The Atlantic for 16.8 incredible years and thanks to everybody who follows me across the river.
- dt
SITUATION DETECTED: Sam Altman, Dario Amodei, and Demis Hassabis have signed a joint open letter calling on Congress to mandate screening of synthetic nucleic acid orders, citing AI’s rapidly improving ability to assist with biological research as an urgent biosecurity risk.
The reason Ozempic makes you feel sick is also part of why it works. It slows your stomach to a crawl, so food sits there and you feel full for hours. Most people accept the nausea as the price of losing weight.
@novonordisk's next drug, zenagamtide, may break that trade. It hit 24% body weight loss over 36 weeks in people, and the new finding presented this month is what sets it apart: it appears to suppress appetite straight from the brain’s hunger circuits, without slowing the stomach at all.
The catch is that the no-slowed-stomach result is still early, shown in animals, not yet confirmed in humans. If it holds, the queasiness that makes people quit may fade, and the rule that you stop these drugs before surgery may stop applying.
The version of these drugs that skips the gut is the one to watch.
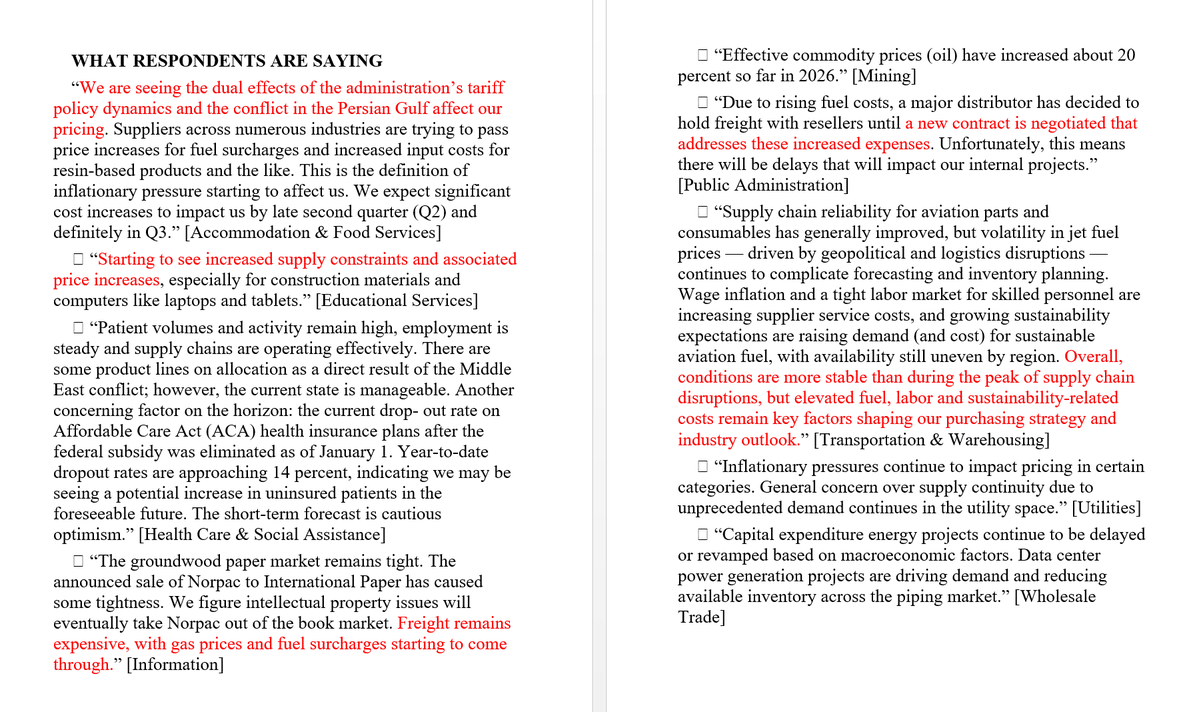
Across the 10 responses included from this month's ISM survey of service-industry purchasing managers (the people who buy things on behalf of businesses), the dominant theme is rising costs, driven by fuel and energy prices, tariffs, and AI-related demand.
No respondent reports prices easing or falling. A few comments focus more on supply tightness than on prices directly, but none point in a disinflationary direction.
Very kind of Dara to sprinkle some tasty morsels into every AI camp's feeding trough
For the AI-value skeptics: They blew thru their annual AI budget in a quarter and they're already pivoting
For skeptics who say the frontier labs have no moat: Once Uber figures out what works, Dara says they'll switch to "efficient models or even "open source."
For the AI boosters: He's still pushing teams to "fundamentally use the power of AI to rebuild systems and processes from the bottoms up"
Dara (CEO of Uber) on their AI spend:
"We blew through our AI budget in a quarter, for the whole year. It is forcing us to adjust.
We are going to meter headcount increases because to the extent that my engineers are getting much more efficient, their throughput is increasing. There's a cost to that, and it's a significant cost.
AI adoption has been occurring in all parts of the business –– whether it's engineers and how they scope projects, how they build, debugging, platform migrations.
I'm pushing the teams to fundamentally use the power of AI to rebuild systems and processes from the bottoms up.
I do think it's a combination for us right now of encouraging adoption, but then driving efficiency.
We're using the more expensive models to explore. Once we scale some of these experiences, we'll look to bring in more efficient models that are more efficient on a token basis or are open source."
Today's topically abundant pod w/ @DKThomp!
On the slush-fund backdown & ending the cycle of political vice-maxxing, AI: bubble or nah, why English-speaking youth are the most unhappy, the debt & fertility kinda crises, why Dems need a Wemby & more.
https://t.co/NnXcls7gLL
"Late Kakistocracy" is that phase of democratic decline where the regime starts running out of ppl who will work for it, and so the folks who aren't qualified for their current positions are promoted to even larger positions for which they are even more unqualified
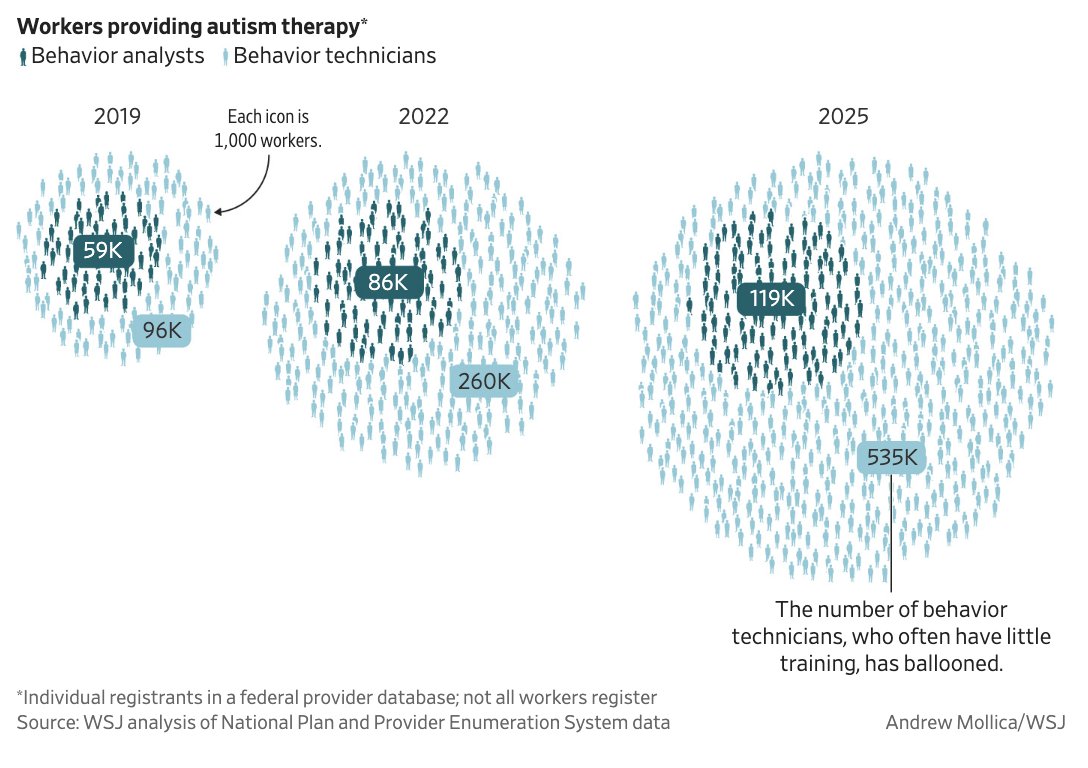
I have no idea what the "right" number of workers in autism therapy is. Feels like a rich developed country should probably have a lot of people working in health care. But it's wild for an industry to quintuple in 6 years. In other contexts, it might even be the sort of thing we call a bubble.
In 2019, there were about 150,000 people working in autism therapy.
Six years later, there were 654,000—more than the number of people who work in mining and logging, or telecommunications, or at the US Postal Service.
I think we're on the verge of a golden age in cardio-metabolic health (thanks GLP1s!) and oncology (CAR-T, daraxonrasib, checkpoint inhibitors).
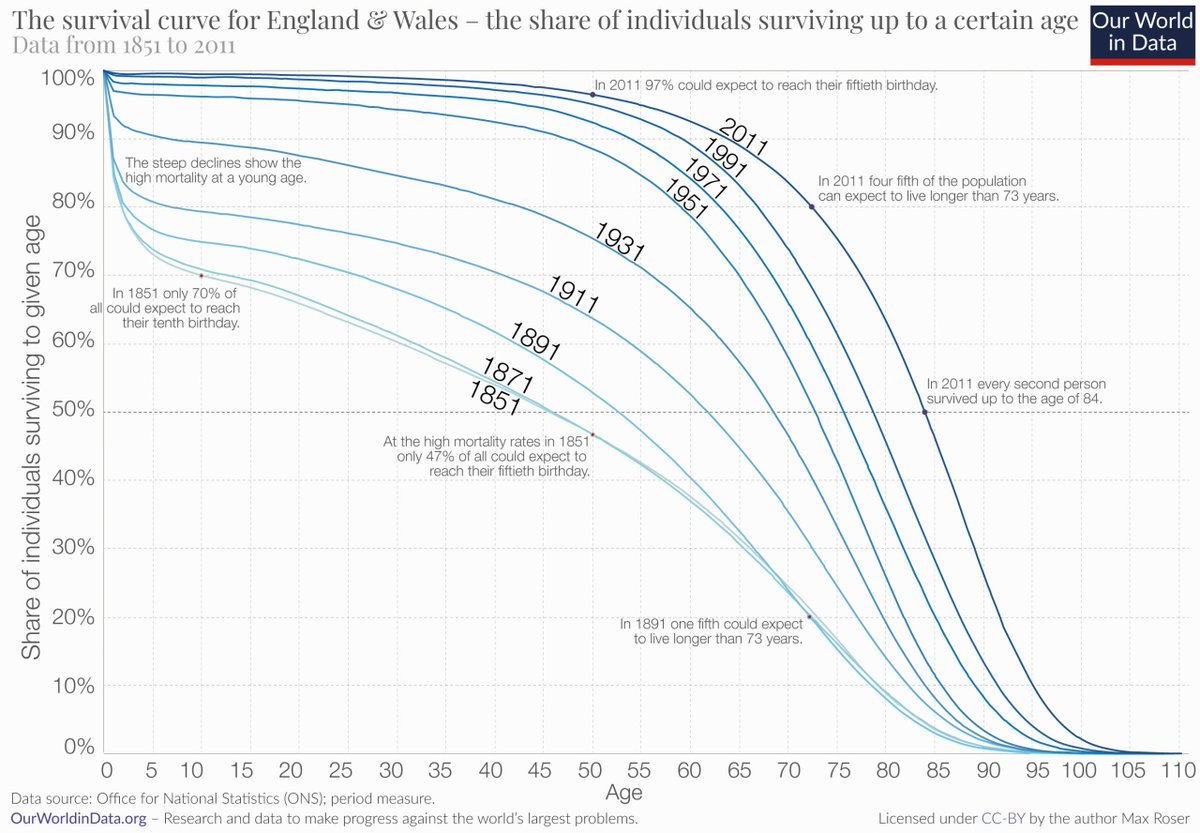
But let's be real about what average lifespans in the 100s would require.
The oldest documented person died 29 years ago. Jeanne Calment at 122yo. In 30 years, with all of the advances in medicine, NOBODY ELSE has even gotten to 120.
A life expectancy at birth of 110 years would require about 25% of women to live longer than Calment and about 6% of women to live past 150—three decades older than the record. (source: Olshansky et al).
This isn't even close to happening yet.
The good news is that we're getting better and better at eliminating death before 80. We're not (yet) getting any better at extending life beyond 110. Doing so will probably require advances that have nothing to do with GLP1s and cancer therapies. You basically need to build new bodies for humans.
if you're under 50 and you stay healthy, i think you will live to 150 years old minimum
the medical singularity is happening.
just in the past 2 months alone:
> revmed's pancreatic cancer drug (daraxonrasib) doubled survival in the deadliest cancer there is, 13.2 months vs 6.7 on chemo. it got a standing ovation from 40k+ doctors at the world's biggest cancer conference
> a one-time gene editing infusion (verve-102) permanently switched off the gene that drives bad cholesterol and cut it up to 62% from a single dose. one and done, no daily pill for life
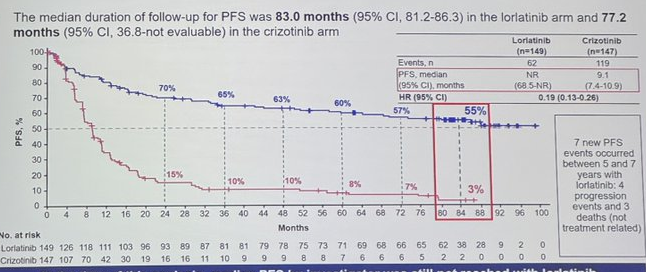
> a lung cancer pill (lorlatinib) kept 60% of patients with spread cancer progression-free at 5 years. the longest anyone has ever held back a metastatic solid tumor with a single drug
> mayo built an ai that catches pancreatic cancer on routine ct scans up to 3 years before doctors can. it spotted 73% of the earliest cases vs 39% for human radiologists
> lilly's new weight loss drug (retatrutide) hit up to 30% body weight loss in its big phase 3 trial, and along the way it cut knee arthritis pain by 76% and dropped bad cholesterol about 20%
and we are still just at the beginning of the exponential
call me crazy but i'm a believer when Demis hassabis says we will cure all disease in the next 10 years
I think we're on the verge of a golden age in cardio-metabolic health (thanks GLP1s!) and oncology (CAR-T, daraxonrasib, checkpoint inhibitors).
But let's be real about what average lifespans in the 100s would require.
The oldest documented person died 29 years ago. Jeanne Calment at 122yo. In 30 years, with all of the advances in medicine, NOBODY ELSE has even gotten to 120.
A life expectancy at birth of 110 years would require about 25% of women to live longer than Calment and about 6% of women to live past 150—three decades older than the record. (source: Olshansky et al).
This isn't even close to happening yet.
The good news is that we're getting better and better at eliminating death before 80. We're not (yet) getting any better at extending life beyond 110. Doing so will probably require advances that have nothing to do with GLP1s and cancer therapies. You basically need to build new bodies for humans.
This has quietly been a miracle month in medicine.
In the last 5 weeks we’ve got news on:
- retatrutide, the triple agonist GLP-1 from Lilly, basically melting fat and body-wide inflammation at record levels
- RevMed’s new pancreatic cancer drug showing unprecedented abilities to extend life
- small trial of a one-and-done PCSK9 gene editing therapy for slashing LDL cholesterol
- Mayo’s AI-assisted radiology showing vastly improved cancer detection
- this new therapy for metastatic solid tumors
This stuff is at varying levels of evidence. Retatrutide is ~100% on its way, other stuff needs more clinical trial data. But put it together and we’re maybe on the verge of majorly reducing the mortality of heart disease and cancer, the two leading causes of death in America.
This is actually insane.
97% of people taking the standard of care for metastatic solid tumor got worse by seven years.
But with lorlatinib, that number was only 45% in the same time!
This is an ENORMOUS jump in the quality of cancer care.
As a non-oncologist, i feel quite comfortable jumping on the bandwagon here. I can count the number of times I've seen unsolvable problems in medicine get solved in my lifetime. No, this is not a cure, but there has been no greater challenge than pancreatic cancer. Nothing worked. Now this...
These results are simply spectacular
Daraxonrasib or Chemotherapy in Previously Treated Metastatic Pancreatic Cancer | New England Journal of Medicine https://t.co/a52WwDQ2Ju