She was instrumental in fostering an environment that fueled public hostility toward doctors as a profession. As a result, many individuals began recording out-of-context videos and using them to pressure and intimidate healthcare professionals, leading to unnecessary harassment and significant psychological stress on medical staff.
A fundamental question remains: why were Assistant Commissioners (ACs) and Deputy Commissioners (DCs) placed in supervisory roles over teaching hospitals when they often lack the necessary healthcare, infection control, and hospital management training required for such responsibilities? This has resulted in frequent disruptions and harassment of healthcare workers, with officials often uncertain about what standards they should be assessing or how modern healthcare systems function.
Knee-jerk reactions such as suspending healthcare professionals may create headlines, but they do not solve underlying problems. Effective healthcare management requires proper root cause analysis, identification of systemic deficiencies, and implementation of sustainable solutions.
For example, if a patient presents with suspected leukemia at many government hospitals in Rawalpindi, there may be no functioning in-house facilities for essential diagnostic investigations such as flow cytometry, molecular testing, or cytogenetic analysis. Without access to these investigations, how can an accurate diagnosis be established? When physicians arrange such tests externally to ensure proper patient care, they are often criticized rather than supported.
Similarly, even for common conditions such as diabetes mellitus, many modern evidence-based therapies—including empagliflozin, semaglutide (Ozempic), and tirzepatide (Mounjaro)—are frequently unavailable in the public healthcare system. Patients are often limited to older, inexpensive medications despite international guidelines recommending broader therapeutic options for appropriate candidates. Such systemic deficiencies cannot be addressed through administrative theatrics or punitive measures.
Unfortunately, many of these actions appear designed for political optics rather than meaningful healthcare reform. They have contributed to the deterioration of an already strained healthcare system.
Having worked in both the Gulf region and the West, I have observed that patient privacy is treated as a fundamental principle. It would be considered unacceptable for administrative personnel with no direct role in patient care to freely enter clinical areas, interact with patients, or participate in ward rounds. Strict infection prevention and confidentiality standards are enforced.
It is therefore concerning to witness situations where non-clinical officials move from bed to bed, shaking hands with patients and touching multiple surfaces without following proper hand hygiene protocols. Such practices not only compromise patient privacy but may also increase the risk of transmitting infections from one patient to another. Healthcare systems should be strengthened through evidence-based policies, professional governance, respect for patient confidentiality, and support for healthcare workers—not through public humiliation, administrative interference, or politically motivated publicity exercises.
Here is health minister totally unaware of ground realities this is a problem in Pakistan where a person with no knowledge becomes a minister and wants to stay in news by hook and crook , the rules in Pakistan are strong and no unqualified person can become a doctor, the HIV control is a system failure of public health authorities and quacks who use , used syringes that are re packaged with no standardized products surgical equipment and unavailable blood tests in the hospital like Elisa . Unsafe sexual practices and making HIV taboo with no doctor in future will touch them with fear of persecution. These type of thoughts also prevailed in America then they saw nobody was willing to treat borderline cases who can deteriorate with these cases moving to other states resulting in false improvement in data . In the end patient suffer . Doctors in Pakistan are underpaid and overworked they should be given resources and protected rather than fed to hyenas .
@saleemspeaks2 Tea has no known side effects it contains theophylline which is a mild stimulant and bronchodilator unlike cigarettes which are cause for cancer and cardiovascular disease . In short this person is lying
Big week for breast cancer at #ASCO26. A few highlights from the meeting:
Metastatic
TROPION-Breast02 + ASCENT-03 (TNBC, PD-L1 ineligible): Two practice-changing Trop2 ADC options for 1L. Subsequent analyses confirm benefit. 2 good options.
VIKTORIA-1 (HR+/HER2-, PIK3CA-mutated, 2L post-CDK4/6i): Gedatolisib + fulvestrant beat alpelisib with a much cleaner toxicity profile. Triplet did not add anything with palbociclib. Less hyperglycemia, less diarrhea. Stomatitis remains a challenge. Will be a nice doublet option if approved. IV drug.
SERENA-6 (HR+/HER2-): Switching to camizestrant when ESR1 mutation is detected on ctDNA, before progression, yielded 51% ctDNA clearance vs 1.9%. Compelling biology. Let’s see what the FDA does.
persevERA (HR+/HER2-, 1L): Giredestrant + palbociclib did not beat letrozole + palbociclib (33.1 vs 28.2 mo, p=0.15). The 1L SERD moment has not arrived yet. Metastatic SERD benefit appears limited to ESR1-mutant disease.
Early Stage
lidERA (HR+/HER2-): First new adjuvant endocrine therapy in decades. Giredestrant cuts recurrence risk about 30% across pre and postmenopausal patients in subgroup analyses. Premenopausal patients need OFS. FDA submission underway.
KEYNOTE-522 at 7 years (TNBC, stage II-III): EFS 78.3% vs 69.8%, OS 85.1% vs 77.2%. The benefit is durable and real. But real-world irAE rates up to 54%. We need a biomarker to identify who can safely skip immunotherapy.
OPTIMA (HR+/HER2-, node-positive): Chemo omission non-inferior in low genomic risk node-positive patients including N2 using Prosigna. Practice changing for postmenopausal patients. For premenopausal, the key insight is that chemo benefit in low genomic risk patients is largely driven by ovarian suppression, not cytotoxicity. Still need more premenopausal N2 data. Enroll to OFSET.
OASIS-4 (HR+, on ET): Elizanetant improves hot flashes AND sleep across tamoxifen, AI, and GnRH agonist therapy. Non-hormonal and safe for HR+ patients. An adherence tool we have really needed.
REDUSE (bone mets): Denosumab every 12 weeks after induction is non-inferior to every 4 weeks for skeletal-related events, with less hypocalcemia, less ONJ, and more than 50% reduction in drug costs. Smarter de-escalation with no efficacy tradeoff.
GLP-1 RAs: Real-world data showing 43% reduction in metastatic progression and 30% mortality reduction in HR+/HER2- patients on ET + CDK4/6i. Still observational, but the tumor GLP-1 receptor expression data suggests this is more than just a metabolic effect. Prospective studies needed.
Grateful for the science.
#BreastCancer #BCSM #Oncology #MedTwitter
Its very unfortunate that we have people with your mindset , that is why I moved out , modern day is all about connectivity right now I am tweeting this in airplane above Atlantic , Bussiness don’t go to places where there are high taxes and ease , whenever I landed in Islamabad the WIFI doesn’t work it asks for a local number or international number for registration which doesn’t receive SMS. That is not what you experience in Dubai , Istanbul, O’Hare or Riyadh the connectivity is super smooth and nowadays people use hotspot to connect their laptops and IPads they use Airdrop , I clouds , etc it’s better for you to use your samsung with zero security protection we outside are better off without your primitive colonial mindset.
That is why no investor wants to come to pakistan because of these century old mindset of governance, as soon as you land in dubai the immigration officer gives you a sim with data and connections so that you don’t have a problem while as soon as I land in pakistan your connection to the world is lost . I phone gets the work done like no other system at present its such a remarkable ecosystem. That is why gulf and in the west 90 percent of population prefer apple ecosystem.
Those who are in Apple ecosystem, iPhone is a must if you go to usa , gulf almost 90 percent have iPhones even security guards except for egypt and pakistan no other country has tax on phones , and egypt followed after pakistan , it’s very easy to get work done when you have I phone plus a mac in this time it’s not a luxury it’s a necessity and one major downside of taxation is that it results in capital flight and stagnation of economy that is what’s causing economic hardships in Pakistan and uk . Ethopia which has very low taxation has invited capital while its neighbors like egypt are struggling. . These old mindset of taxations should change as it only funds redundant bureaucracy and funding incompetent governments.
@DrNaeemMeoMD Unfortunately 99 percent of media and officials in high positions have zero understanding of how health care works . Problem is CM and PM why they are scumming to undue pressure and should stand with truth.
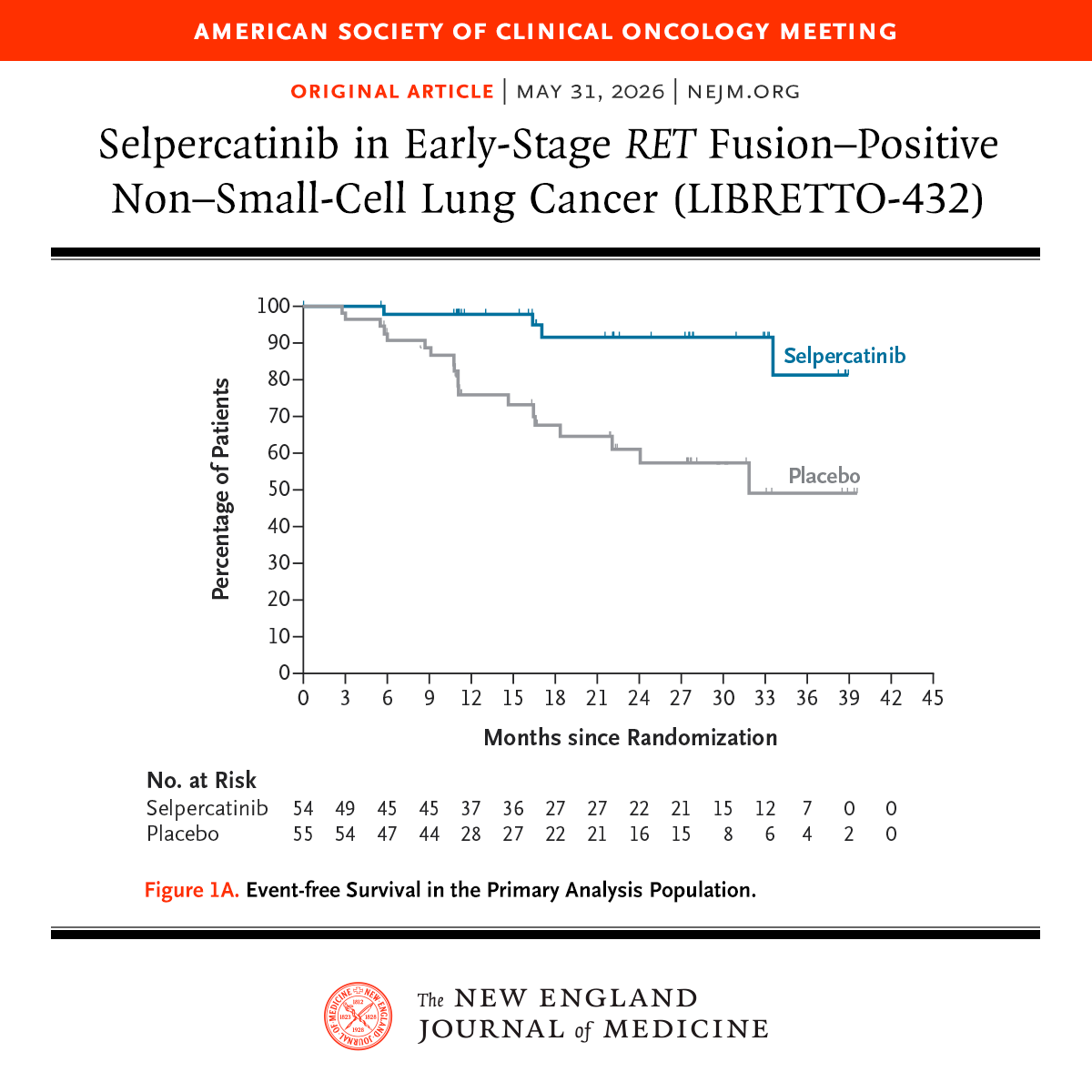
Presented at #ASCO26:
Among patients with 𝘙𝘌𝘛 fusion–positive non–small-cell lung cancer, adjuvant selpercatinib led to longer event-free survival than placebo. Adverse events of grade 3 or higher included elevated liver-enzyme levels. Full phase 3 LIBRETTO-432 trial results: https://t.co/o3iLF3tu6p
@ASCO
#ASCO26
ER+, HER2- breast cancer management is becoming less about “one-size-fits-all” and more about precision escalation vs precision de-escalation.
The future is clear:
🧬 Biomarkers decide who gets chemo
💊 CDK4/6 inhibitors move earlier
🩺 Endocrine therapy intensifies in high-risk disease
⚖️ Obesity and supportive care become survival interventions
Key themes from ASCO 2026:
▪️ Anthracyclines may still matter in selected genomically high-risk patients
▪️ Some node+ patients may safely avoid chemotherapy
▪️ OFS + AI remains critical for high-risk premenopausal disease
▪️ Adjuvant abemaciclib and ribociclib continue reshaping standards
▪️ Oral SERDs are entering early breast cancer
▪️ Weight management may become part of oncologic care itself
Breast oncology is shifting from anatomy-driven to biology-driven treatment selection.
Which biomarker do you think will have the biggest impact in early ER+ breast cancer over the next 5 years? 👀
@OncoAlert@ASCO@myesmo@esmo_open@larvol
#OncoTwitter #MedTwitter #BreastCancer #bcsm #PrecisionOncology
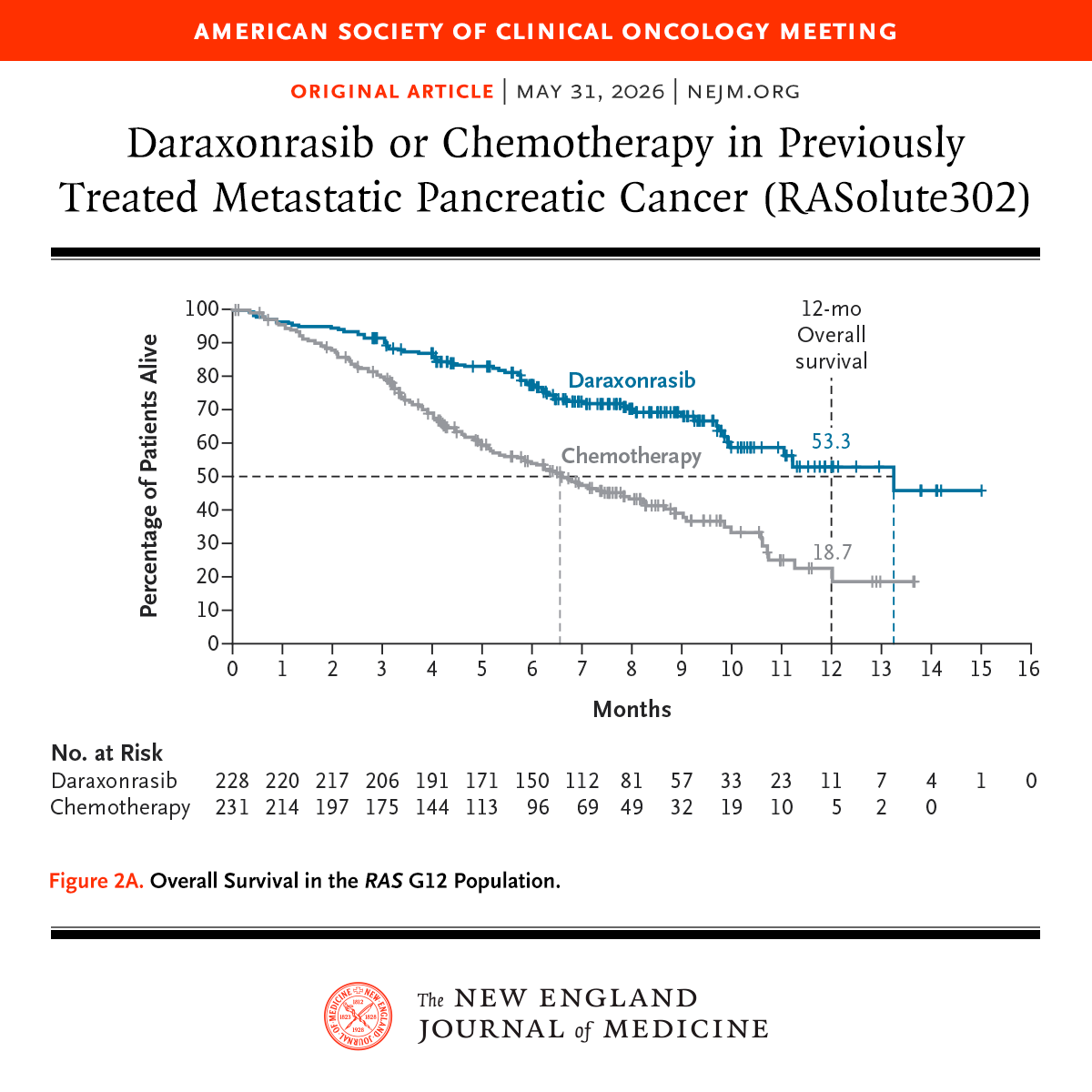
Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
#ASCO26
Can lower-intensity therapy outperform “7+3” in the real world for AML patients at high risk of induction mortality?
A prospective Indian study from Tata Memorial Hospital compared AZA+VEN vs intensive 3+7 induction in de novo AML patients.
🧪 Study population
• 154 patients with de novo AML
• 3+7: n=73
• AZA+VEN: n=81
• AZA+VEN group had older age, worse PS, more adverse-risk disease, and significantly more baseline fungal infections
📌 Key findings
✅ Similar induction mortality
• AZA+VEN: 7.5%
• 3+7: 8.2%
✅ Lower toxicity with AZA+VEN
• Febrile neutropenia: 77.7% vs 95.9%
• MDR sepsis: 8.6% vs 32.8%
• New fungal pneumonia: 14.8% vs 27.4%
✅ Lower time toxicity
• Median healthcare contact:
19 vs 26 days
✅ Lower financial burden
• ~19% lower median treatment cost
⚠️ Tradeoff:
Lower CR/MRD-negative rates with AZA+VEN, likely reflecting the much poorer-risk baseline population.
In LMIC settings where infections, delayed admissions, and poor PS are common, AZA+VEN may be emerging as a pragmatic frontline option for selected high-risk AML patients.
Will this change induction strategies in resource-constrained settings?
@ASCO@OncoAlert@myesmo@ASH_hematology@TataMemorial
#AML #Leukemia #HemOnc #MedTwitter
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO