HematoloOncologist, BMT Physician, Fellow traveller. Science Enthusiast. Freethinker. In love with nature and myself. Humanity is my religion. Eden's Dad.
After ASCO, its' #EHA2026 season- AND THIS YEAR, I AM READING #MULTIPLEMYELOMA DIFFERENTLY.
Not as a list of exciting abstracts.
But as a blueprint for what focused myeloma care must actually deliver.
➡️ A few EHA 2026 themes I am watching closely:
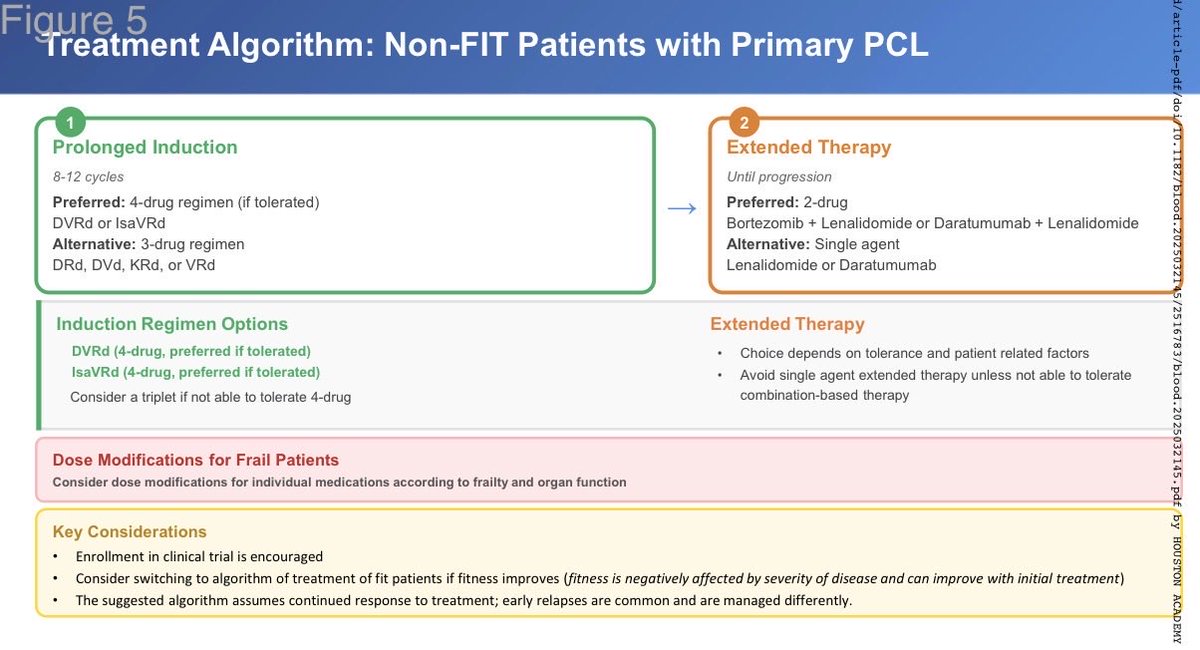
▪️ 1. Frontline myeloma: depth is important, but patient selection is everything.
CEPHEUS, IDEAL and DREAMM-9 continue the global movement towards deeper frontline responses.
For us, the best frontline strategy is not just the most powerful regimen.
It is the most appropriate, deliverable and sustainable one.
▪️ 2. Frailty and renal dysfunction cannot be side notes.
AGMT MM04 wth isatuximab-Rd in elderly NDMM, and iberdomide–daratumumab- dexamethasone analysed by renal function, are very relevant to our real-world patients.
Many patients do not come to us as “trial-perfect” patients.
They come with anemia, renal dysfunction, infections, bone disease, frailty, delayed diagnosis & financial limitations.
▪️ 3. Relapsed myeloma: sequencing is becoming the real science.
MonumenTAL-3, MajesTEC-9, MajesTEC-3, SUCCESSOR-2, DREAMM-7/9 and CAMMA-2 all point to the same direction.
The relapse clinic is becoming target-based.
For us, many patients may not get unlimited lines of therapy.
The sequence we choose today may decide what remains possible tomorrow.
▪️ 4. AL amyloidosis deserves its own pathway.
LINKER-AL2 with linvoseltamab in relapsed/refractory systemic AL amyloidosis is important beyond the molecule.
The bigger challenge for us is not just access to newer therapy.
It is earlier diagnosis and faster referral.
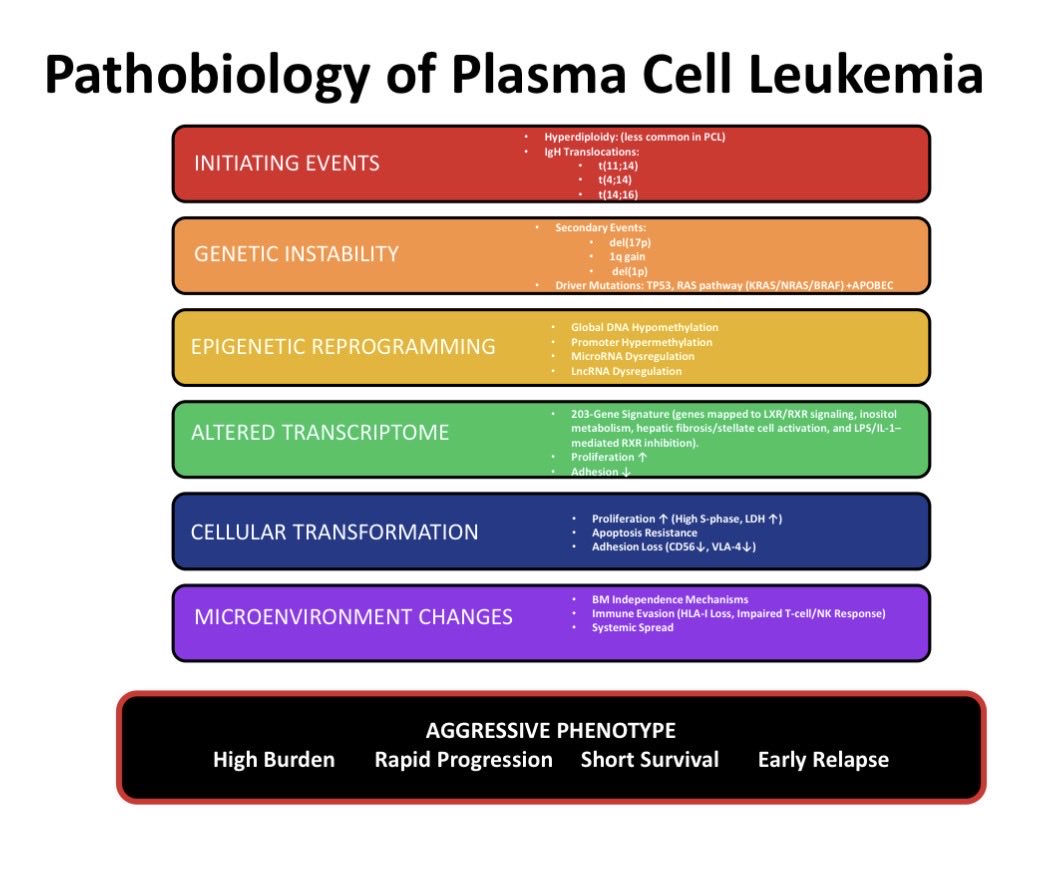
▪️ 5. Biology cannot remain optional.
The whole-genome sequencing/immunotherapy-resistance abstract is an important reminder: Relapse has biology.
We need to ask better biological questions before we choose the next treatment.
As EHA 2026 begins globally, we also launch the Centre of Excellence for Myeloma & Lymphoma at Fortis Gurugram on 11th June. This week feels special.
#mmsm #EHA2026
One of the hardest conversations in #Multiplemyeloma, now with a NEW DATE.
Pleased to share the revised date for our upcoming session with Dr Shaji Kumar sir, Mayo Clinic on:
ULTRA-HIGH-RISK AND HIGH-RISK MYELOMA: Recognizing Dangerous Biology Early and Choosing Action Before the Disease Outruns Us
In High-Risk myeloma, the challenge is not only identifying risk on paper but also knowing when biology should alter strategy.
📅 21 May 2026
⏰ 6:00- 7:00 PM IST
🌍 7:30- 8:30 AM Rochester time
▪️Registration link - https://t.co/QLGLdkx9sg
If you have any questions to discuss, please DM me. 📩
#Highriskmyeloma #mmsm #multiplemyeloma
@myelomaMD@IndMyAcGp@IMFmyeloma@Myeloma_mSMART@theMMRF@MM_Hub@RahulDoc2
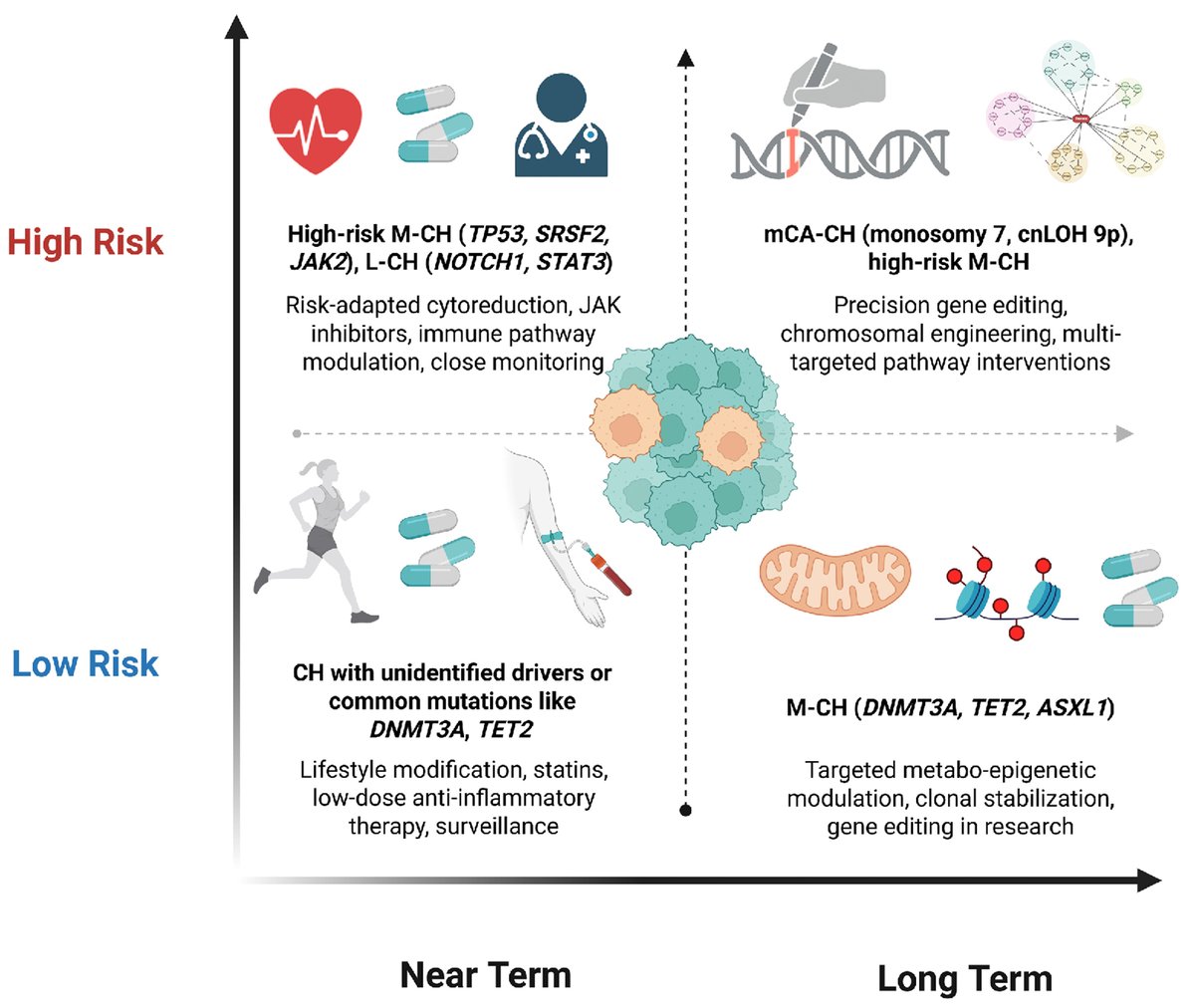
Review series on clonal hematopoiesis: how should clinicians approach clonal hematopoiesis in practice?
This review outlines current strategies for risk assessment, monitoring, and clinical decision-making.
https://t.co/GLf7CKmA1Q
Review series on clonal hematopoiesis: can clonal hematopoiesis be targeted therapeutically?
This review explores emerging strategies aimed at modifying clonal expansion and disease risk.
https://t.co/brJ65j6gDj
@mehak_trehan So many BCMA targeted therapies now. Teclistamab, Elranatamab now, Blenrep and CARTs soon. We need to find an ideal sequencing of these immunotherapies available, which I think is a serious dilemma in the coming days. With Elrana now in market, the prices will also come down.
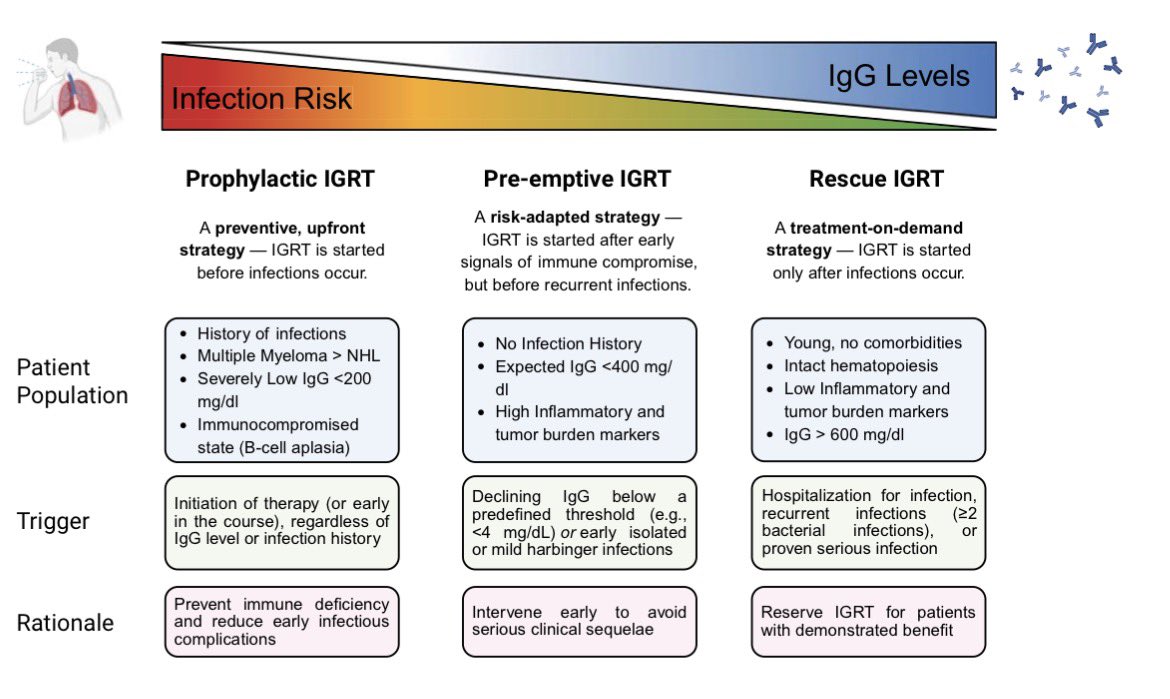
Our attempt to summarize infection PPx for bsAbs across diseases & targets succinctly… Thanks @KRejeski@JoshuaHillMD@BloodPortfolio for this!
Relevant to both lymphoma and myeloma.
BCMA bsAbs are unique… use true IVIG PPx, don’t wait for Gr3+ infection or arbitrary IgG ⬇️!
Lambda 2522 → <1.34 mg/L.
In weeks.
That’s talquetamab bridging in aggressive EMD.
Got the patient to CAR-T.
Ended MRD-negative.
Speed is therapy.
#MultipleMyeloma#Talquetamab#CART
1/
In NDMM, is Daratumumab the new norm - or are we letting PFS excitement outrun LMIC reality?
Because yes: if the endpoint is PFS, Dara is winning.
But if the endpoint is value, the debate is very much alive. #mmsm
When frontline myeloma data evolve faster than access, sequencing becomes more than science : it becomes strategy! ✨
Join us for an Expert Roundtable on:
Sequencing Daratumumab and Transplant in Newly Diagnosed Multiple Myeloma Across LMIC Settings
Chaired by @VincentRK , with panel experts from India, Vietnam, Myanmar, Bangladesh, and Nepal.
1 April 2026 | 7:00 PM IST
Registration link - https://t.co/WhCpfD43Jd
Looking forward to a thoughtful discussion on what matters in the real world: who benefits, when to intensify, and how LMIC realities shape decisions.
@MirghSumeet@RahulDoc2@nikhil91sjmc@DrPMPGI@Charanpreet_14
#MultipleMyeloma #Myeloma #Hematology #HemOnc #LMIC #mmsm #MedTwitter
Key Myeloma therapy update for 2025
1) Newly diagnosed: Start treatment with quads, if possible. (Dara-VRd or Isa-VRd).
2) Auto Transplant: can be deferred for standard risk patients, especially if good response to induction. But collect and store stem cells for future use.
3) Maintenance: Doublet maintenance with Dara/ Len or bortezomib/ Len for high risk myeloma. Either Single or Doublet maintenance for standard risk.
4) Use new IMWG IMS risk stratification
5) First relapse: standard triplet therapy is fine for most. CART in first relapse mainly for functional high risk (progression or early relapse with induction).
6) When using CART, disease burden should be controlled and minimal to reduce risk of serious toxicity.