At just 15 years old, Laurent Simons earned a PhD in quantum physics from the University of Antwerp. Now, the teenage prodigy has set his sights on one of humanity’s greatest challenges: solving the problem of aging.
Rather than pausing after his remarkable achievement, Simons has already begun a second PhD, this time combining medical science with artificial intelligence. His ultimate ambition is to deepen our understanding of aging and disease in order to extend healthy human lifespan.
Simons views death as a complex puzzle composed of pieces from biology, physics, and engineering. He plans to tackle it from multiple disciplines, leveraging powerful AI tools to detect patterns in biological systems that might otherwise remain hidden.
His academic journey has been extraordinarily accelerated. He completed high school at age 8, earned a bachelor’s degree by 12, and finished both a master’s and a PhD in quantum physics before most people begin university. His doctoral research explored exotic states of matter, such as Bose-Einstein condensates, where atoms behave as a single quantum entity at temperatures near absolute zero — work that has important implications for quantum computing and advanced sensing technologies.
Now shifting his focus toward biology, Simons joins a growing field where AI is accelerating medical breakthroughs, from early disease detection and protein modeling to faster drug discovery. In aging research, scientists are investigating ways to repair cellular damage, clear dysfunctional cells, and better understand the mechanisms of aging.
Experts caution that truly “solving” aging is one of the most difficult challenges in science. While lifespan extension has been achieved in simple organisms and mice, translating those results to humans remains uncertain and will likely require decades of work.
Still, Laurent Simons’ bold vision highlights an exciting trend in modern science: major advances are increasingly occurring at the intersection of disciplines, and a new generation of thinkers is pursuing ambitious goals with unprecedented speed and creativity.
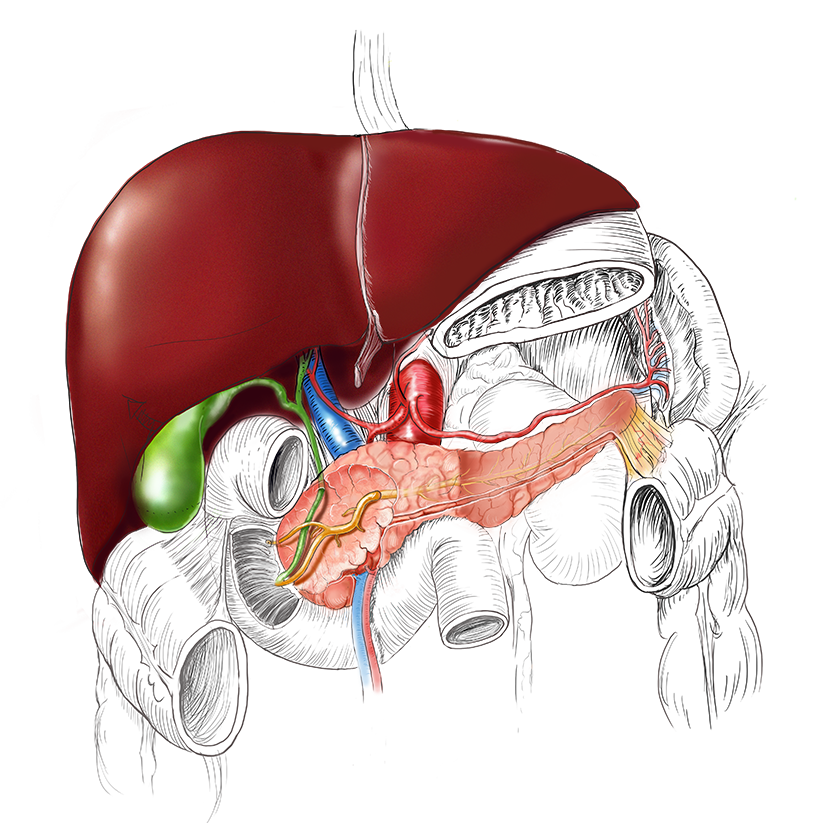
Nuevo video💻en el #videoatlas: "Trasplante de páncreas: pasos técnicos del implante pancreático"
Se presentan los pasos técnicos del implante pancreático en un trasplante de forma detallada y estandarizada.
🔗https://t.co/8cEixVv4vL
@laparostato@Curro_Blanco@pedromontalbann
Short 🧵for those interested in trauma on the mathematics of nonoperative management (NOM) of splenic injury -
And specifically: an argument explaining why you cannot have even ONE death from bleeding in a patient undergoing NOM in your *entire career*.
(1/ )
Revisiting one of my most popular🧵:
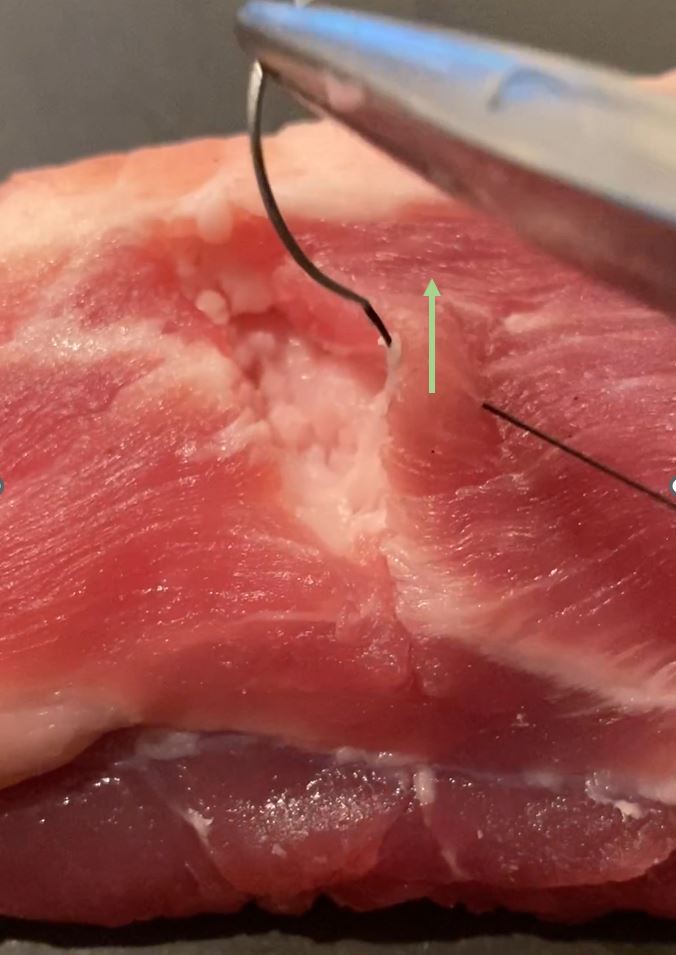
Ways in which you can inadvertently damage fragile tissues when approximating them with sutures.
These ideas are important mostly when the tissue is friable, because this is when you won't get away with using sloppy technique.
(1/ )
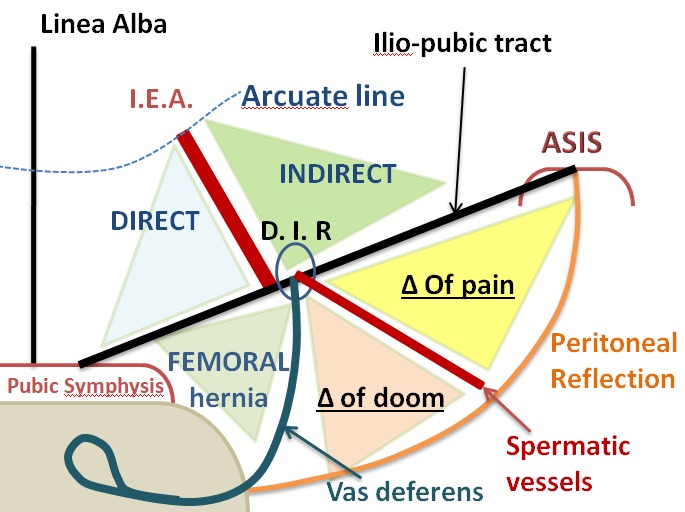
Master the surgical anatomy of laproscopic inguinal hernia.
Key concepts: Direct vs Indirect hernia, Femoral hernia, Triangle of Doom, Triangle of Pain, Iliopubic tract, Inferior epigastric vessels, and ASIS landmarks.
A quick visual guide on this high-yield topic.
A lot of people in academic medicine explain things in an overcomplicated fashion, in part to create a certain mystique around themselves and give others the impression that they understand things at some higher level than the average practitioner is able to.
It works especially well if the person sounds confident when they speak, because the listener will usually not have enough mastery of the subject to question them on it. People think that when they can’t understand what’s being said, that the problem is with themselves. Entire careers are built on this dynamic.
As learners, you have to recognize that this behavior is often false. True geniuses do exist, but are rare. The prevalence of individuals that truly understand things that no one else can is definitely much less than 1 per department.
The 2 take-home messages from this are:
1) In general you want your teachers to spend most of the time making things reductive; in other words, making them seem simpler, not more complex.
2) the confidence with which someone says a thing has little correlation to whether it is true or not. Being a good salesperson helps one’s career in medicine as much as it does in other fields, and you have to recognize when the person talking to you is bluffing.
🚨Se acaba de publicar la primera guía de la AHA/ACC sobre embolia pulmonar aguda.
Y tiene 75 páginas 📄
Te hemos resumido los 10 puntos clave que destacan las guías, con ilustraciones y explicaciones.
Dentro hilo 👇🏼1/12
"Hot" Laproscopic Cholecystectomy
🔴Principles remain the same
🔴Know bailout options
➡️Subtotal
🔴Gallbladder decompression
🔴Identification of Rouviere's sulcus if present
🔴Endo pledget very useful in these cases
🔴Suction/irrigation
➡️blunt dissection
🔴Demonstrate CVS
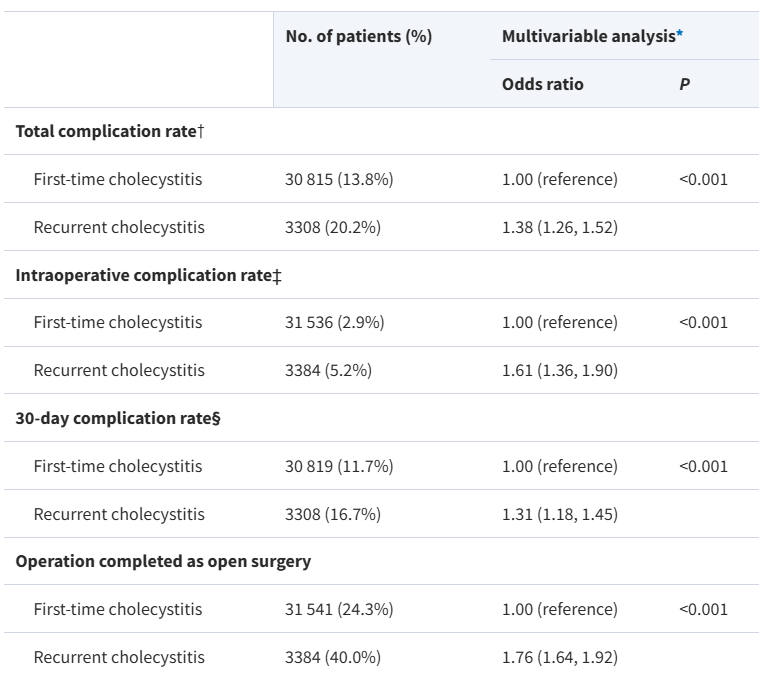
Early cholecystectomy for recurrent versus first-time cholecystitis: nationwide population-based study
➡️https://t.co/PmL1pvRW0K
This population-based cohort study from Sweden found that patients undergoing early cholecystectomy for recurrent cholecystitis had higher rates of complications than those operated on during their first episode. Those with recurrent cholecystitis had increased risks of bile duct injury, intestinal perforation, prolonged surgery, and conversion to an open procedure. The findings support early surgical intervention during the initial episode to reduce the risk of adverse outcomes associated with recurrence.
👏👏👏Magnus Edblom , Lars Enochsson , Hanna Nyström , Gabriel Sandblom , Urban Arnelo , Oskar Hemmingsson , Ioannis Gkekas
#SoMe4Surgery #MedTwitter #SurgEd #Surgery @BJSAcademy@BJSurgery #some4hpb
Monthly focus on HPB surgery
🔗 Check it out here https://t.co/QBpDuL59EL
These videos provide the latest evidence-based techniques and surgical insights to enhance your clinical practice.
#surgery#minimallyinvasive#hpbsurgery#innovation#laparoscopy
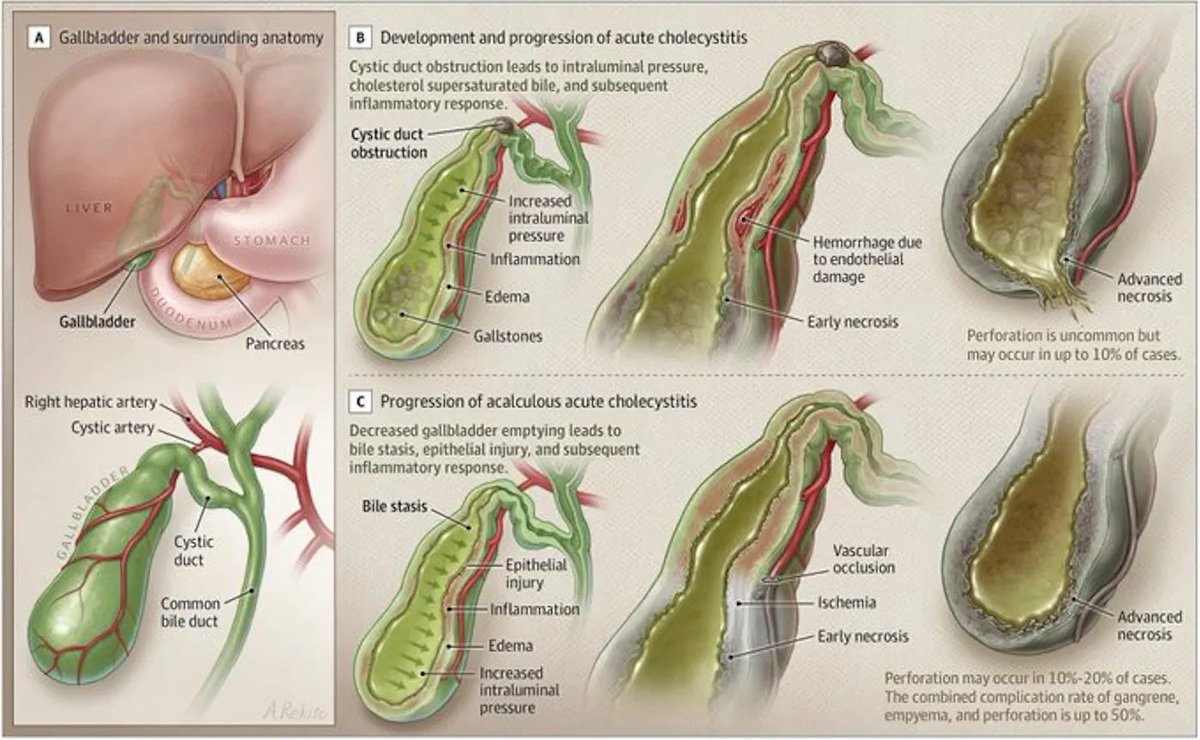
ACUTE CHOLECYSTITIS - Timing of Surgery Changes Everything
DIAGNOSIS: Gallstone obstruction causes 90-95% of cases. Ultrasound shows 81% sensitivity, 83% specificity.
Early vs late laparoscopic cholecystectomy
EARLY SURGERY (1-3 days):
- 11.8% complications
- 5.4 day hospital stay
- Lower costs
LATE SURGERY (>3 days):
- 34.4% complications
- 10.0 day hospital stay
- Higher costs
BOTTOM LINE: Early lap chole cuts complications by two-thirds and halves length of stay.
SOURCE: J. Gallaher and A. Charles. JAMA. 2022;327(10):965-975
Read the full review: https://t.co/46j43ZpuHM
🔥 Surgical History Sunday 🔥
I have an actual technique 🧵coming soon, but in the meantime, I found a few interesting Harvey Cushing historical tidbits to share:
First: he apparently made the following comment about technique (as related by Moynihan):
(1/ )
Students and residents often wonder why our practice patterns on ’Issue X’ are not always in direct agreement with whatever the latest study on Issue X says.
Usually, this is because opinions on Issue X are not static, but instead are swinging on a pendulum over the years.
Redo🧵(originally from 2023) for students about using forceps to 'set down' the suture threads in a running suture, so that they are evenly spaced (L picture) instead of irregular (R picture).
We'll see a simple way to do this, and what may happen if it isn't done.
(1/)