@aribindi@ross_prager High dose adrenaline causes alpha effects and vasoconstriction. Learned this from the Paris Team that routinely limits their administration to 3 x 1mg boluses. My anecdotal experience resonates with this.
Monoclonal antibodies are not named as "mabs" anymore👇
Suffixes/stems
As the previous INN nomenclature scheme for monoclonal antibodies (mAb), this new INN mAb nomenclature scheme is used for all substances that contain an immunoglobulin variable domain that binds to a defined target, and that is composed of only immunoglobulin-derived pharmacologically active components. The suffix is preceded by an infix that indicates the target class.
However, in contrast to the previous INN mAb nomenclature scheme, the new INN mAb nomenclature scheme divides the substances that contain an immunoglobulin variable domain into four groups, there being three groups for monospecific immunoglobulins and one for bi- and multi-specific immunoglobulins, independent of their type, shape and form.
---
Group 1
-tug for unmodified immunoglobulins
Monospecific full length and Fc unmodified[1] immunoglobulins of any class. Molecules which might occur as such in the immune system. Including:
IgG, IgA, IgM, IgD, IgE
only allelic variants
Glycoengineering without mutation
C-terminal lysine deletion without any other mutation in the Fc region
---
Group 2
-bart for antibody artificial
Monospecific full length immunoglobulins with engineered constant domains (CH1/2/3).
Monospecific full length immunoglobulins that contain any point mutation introduced by engineering for any reason anywhere (hinge, new glycan attachment site, mixed allelic variants which would not occur in nature, altered complement binding, altered FcRn binding, altered Fc-gamma receptor binding, etc.)
e.g. IGHG4 with S>P mutation, stabilized IgA
---
Group 3
-mig for multi-immunoglobulin
Bi- and multi-specific immunoglobulins regardless of the format, type or shape (full length, full length plus, fragments)
---
Group 4
-ment for fragment
All monospecific domains, fragments of any kind, derived from an immunoglobulin variable domain
(all monospecific constructs that do not contain an Fc domain)
@WCGHWEMS - join our Annual EMS Research Day. Your participation and engaging conversation is the fuel required during our pursuit for clinical excellence
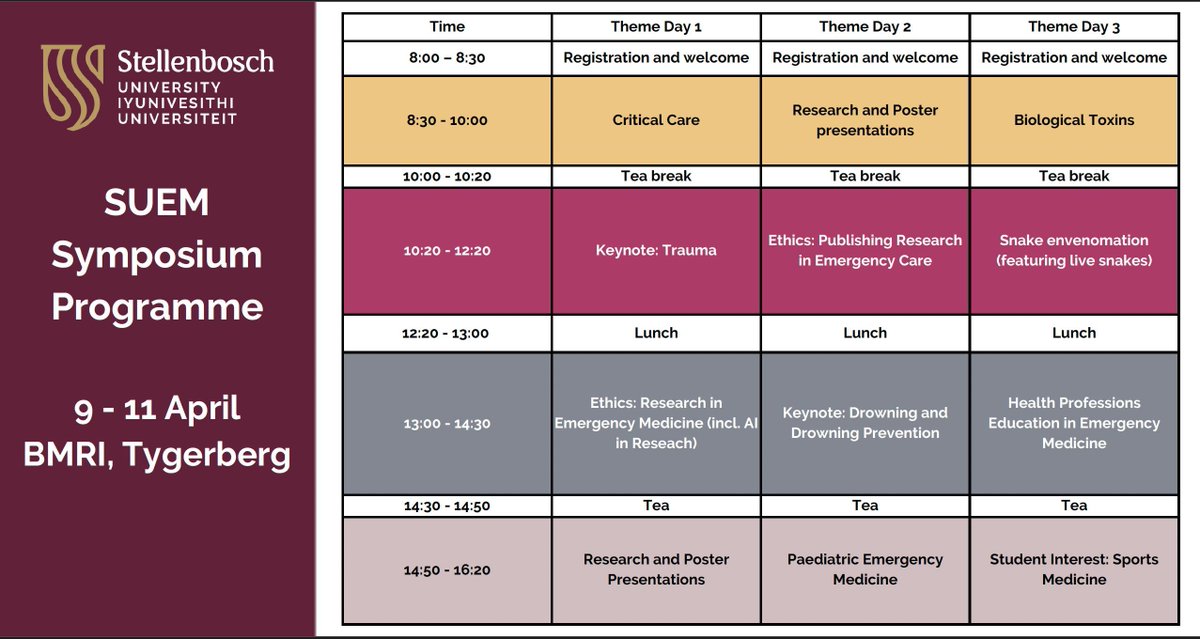
Register for the #SUEM25 symposium and take advantage of the early bird special, featuring abstract, poster presentations, trauma, ethics sessions and much more!
Deadline for early bird is 31 January and deadline for abstracts is 14 February
Register at:
https://t.co/lqyF9cDudW
⚠️ Bleomycin & anaesthesia⚠️
Do you know what precautions are required in patients who have been exposed to bleomycin?
Exposure to high FiO2 at any time post-bleomycin exposure may trigger life-threatening pneumonitis.
@DrSusannahP
#AnSky #MedSky #OncSky
https://t.co/I8ZYKZZXVE
Have you heard about the script that saves you time and money? Grab an exclusive discount for the most intelligent script in SA.Redeem your 50% discount today on a web browser at https://t.co/sDNQP6v0zz
Use the referral code below upon checkout:
VLOK142
Early 40s male with chest pain and collapse, looks horrible, SBP 80, lactate 7.
Previous large PE with pulmonary hypertension on echo 2 months ago, discharged on apixaban
POCUS on arrival shows:
🔍 Mastering the Complexities of Ischemic Stroke: A Comprehensive Diagnostic Approach
When faced with an ischemic stroke or TIA, it’s crucial to accurately identify the underlying cause to tailor the most effective treatment. This flowchart breaks down the essential steps in differentiating between cryptogenic stroke and its subtypes: ESUS (Embolic Stroke of Undetermined Source) and Lacunar Stroke.
Key Insights:
1.🔎 Lacunar Stroke Diagnosis:
•The ARCADIA criteria guide us in diagnosing lacunar strokes. Look for subcortical infarcts within the distribution of small penetrating arteries, with lesions less than 1.5 cm on CT or T2-MRI, or less than 2.0 cm on DWI MRI.
•Always consider the presence of atrial cardiopathy or systemic embolism, as this can significantly influence the management strategy.
2.🩺 ESUS Pathway:
•For ESUS, after thorough cardiac monitoring, the absence of atrial fibrillation directs us to investigate other potential sources, including carotid web, complex aortic plaque, non-stenotic carotid plaque, PFO, or occult cancer.
•Treatment options vary: from antiplatelet agents and statins to PFO closure or anticoagulation therapy—each tailored to the identified source.
3.💓 Atrial Cardiopathy:
•Pay attention to specific markers like PTFV1, NT-proBNP levels, and left atrial diameter index to diagnose atrial cardiopathy.
•In cases without atrial fibrillation, start with antiplatelet agents and keep an eye on the upcoming results from the ARCADIA & ATTICUS trials to refine your approach.
Teaching Point:
This structured approach ensures that we’re not just treating the stroke, but addressing its root cause. By applying these diagnostic criteria, we can better prevent recurrent strokes and optimize patient outcomes.
#StrokeAwareness #Neurology #Cardiology #IschemicStroke #ESUS #LacunarStroke #AtrialCardiopathy #StrokePrevention #CriticalCare #HealthcareInnovation
As part of the upcoming FCEM Part II examination, I have collected some useful research in this collection using Read by QxMD: FCEM II (South Africa) https://t.co/RGpWjZV0L3
Open to collaboration and contribution
#SouthAfricanEmergencyCare#EMSSA
What an incredible publication!
Pain is such a universal human experience but continues so poorly understood and managed. This book has a huge impact.
Well done @JoParkRoss and @RomyParker1
Published today! Free & open access!
Understanding Pain unravels the physiology, assessment and treatment of pain centred around patient stories.
Access here: https://t.co/ujocEgj7NR
1/n
Such a great initiative by National Department of Health!
This promises to be a fantastic session with the extra-ordinary, inspiring and marvelous @cunningham_char
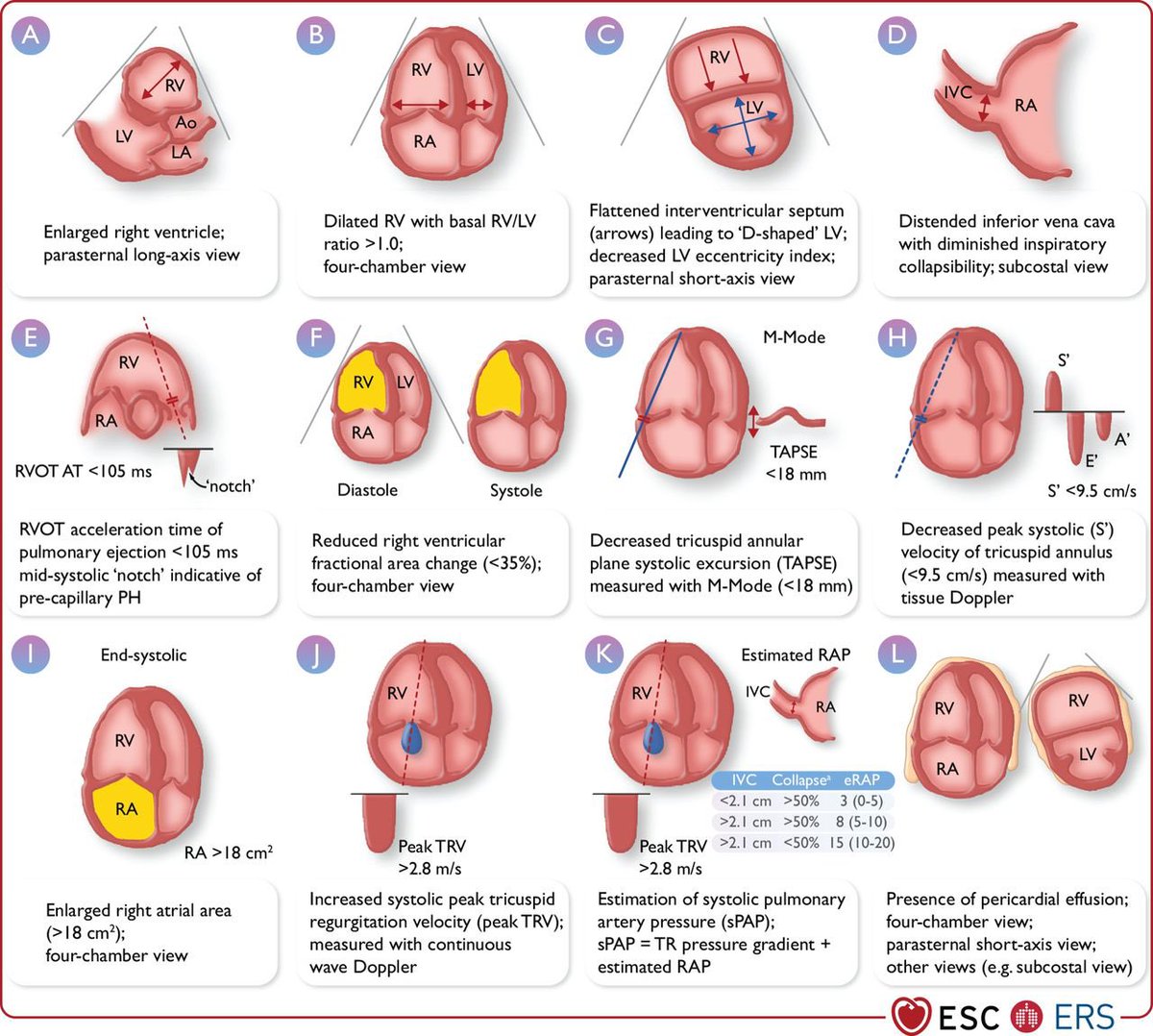
July series for new #ICU#Nephrology fellows:
Cardiac #POCUS parameters in the assessment of pulmonary hypertension
#echofirst#FOAMed#Nephpearls
Click 'ALT' for abbreviations
Courtesy: 2022 ESC/ERS pulm HTN Guidelines
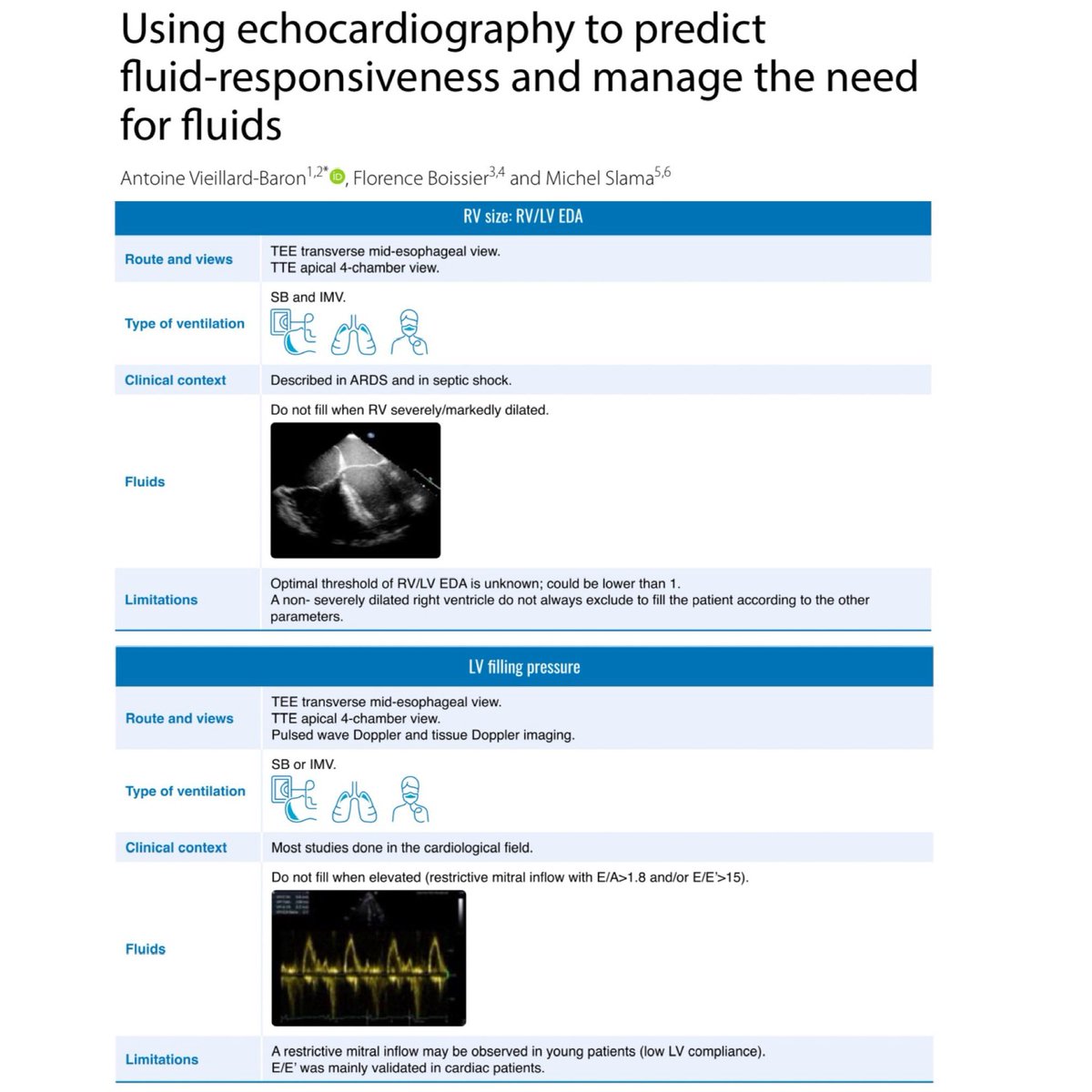
As resuscitationists keep searching for the holy grail of volume status and fluid responsiveness, we have trekked into the world of echocardiography. This paper adds some nunchuck skills to our bow-staff skills. 🎩 tip to the authors.
https://t.co/4Ise540F2X
























![docakx's tweet photo. Monoclonal antibodies are not named as "mabs" anymore👇
Suffixes/stems
As the previous INN nomenclature scheme for monoclonal antibodies (mAb), this new INN mAb nomenclature scheme is used for all substances that contain an immunoglobulin variable domain that binds to a defined target, and that is composed of only immunoglobulin-derived pharmacologically active components. The suffix is preceded by an infix that indicates the target class.
However, in contrast to the previous INN mAb nomenclature scheme, the new INN mAb nomenclature scheme divides the substances that contain an immunoglobulin variable domain into four groups, there being three groups for monospecific immunoglobulins and one for bi- and multi-specific immunoglobulins, independent of their type, shape and form.
---
Group 1
-tug for unmodified immunoglobulins
Monospecific full length and Fc unmodified[1] immunoglobulins of any class. Molecules which might occur as such in the immune system. Including:
IgG, IgA, IgM, IgD, IgE
only allelic variants
Glycoengineering without mutation
C-terminal lysine deletion without any other mutation in the Fc region
---
Group 2
-bart for antibody artificial
Monospecific full length immunoglobulins with engineered constant domains (CH1/2/3).
Monospecific full length immunoglobulins that contain any point mutation introduced by engineering for any reason anywhere (hinge, new glycan attachment site, mixed allelic variants which would not occur in nature, altered complement binding, altered FcRn binding, altered Fc-gamma receptor binding, etc.)
e.g. IGHG4 with S>P mutation, stabilized IgA
---
Group 3
-mig for multi-immunoglobulin
Bi- and multi-specific immunoglobulins regardless of the format, type or shape (full length, full length plus, fragments)
---
Group 4
-ment for fragment
All monospecific domains, fragments of any kind, derived from an immunoglobulin variable domain
(all monospecific constructs that do not contain an Fc domain)](https://pbs.twimg.com/media/G-tL5F9bQAEKvvc.jpg)