“Getting prior authorization reform at the federal level would be so impactful…” The #SeniorsAct is just that, a bipartisan bill that would help #FixPriorAuth for pts across the country.
Write to Congress and tell them to act NOW: https://t.co/PahCggHQWk
#ASCOAdvocacy
First-Line Nivo + Low-Dose Ipi for MSI Advanced Gastric or Esophagogastric Junction Cancer
@JCO_ASCO
https://t.co/9cnpkDcqRh
🔎Phs II NO LIMIT
👉ORR 62.1%, 10.3% CR, DCR 79.3%
👉mPFS 13.8 mo
👉gr ≥3 TRAEs 37.9%
👉interesting translational program
@myESMO
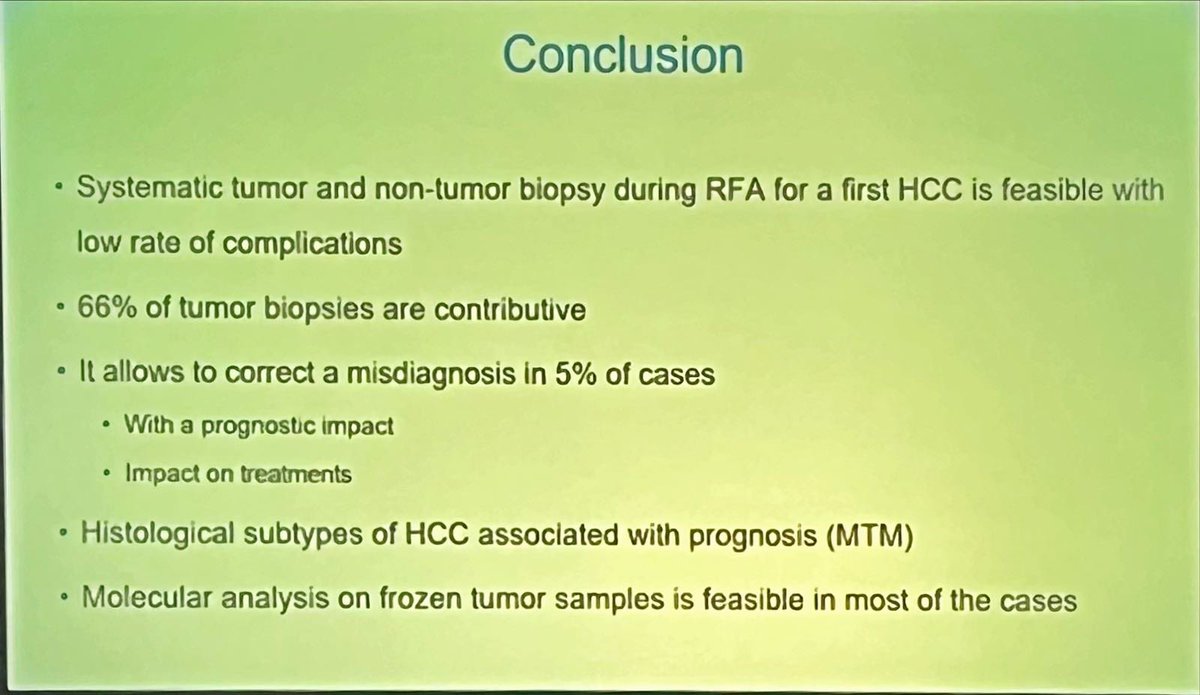
Liver #biopsy in suspected #HCC data presented at @EASLnews#LiverCancerSummit 2025 in Paris by Blase et al
5% are other histology - some being #CCA (this has huge implications for those individual patients!)
No tumour seeding identified 😉
Personally, in favour of biopsy 🙋🏻♀️
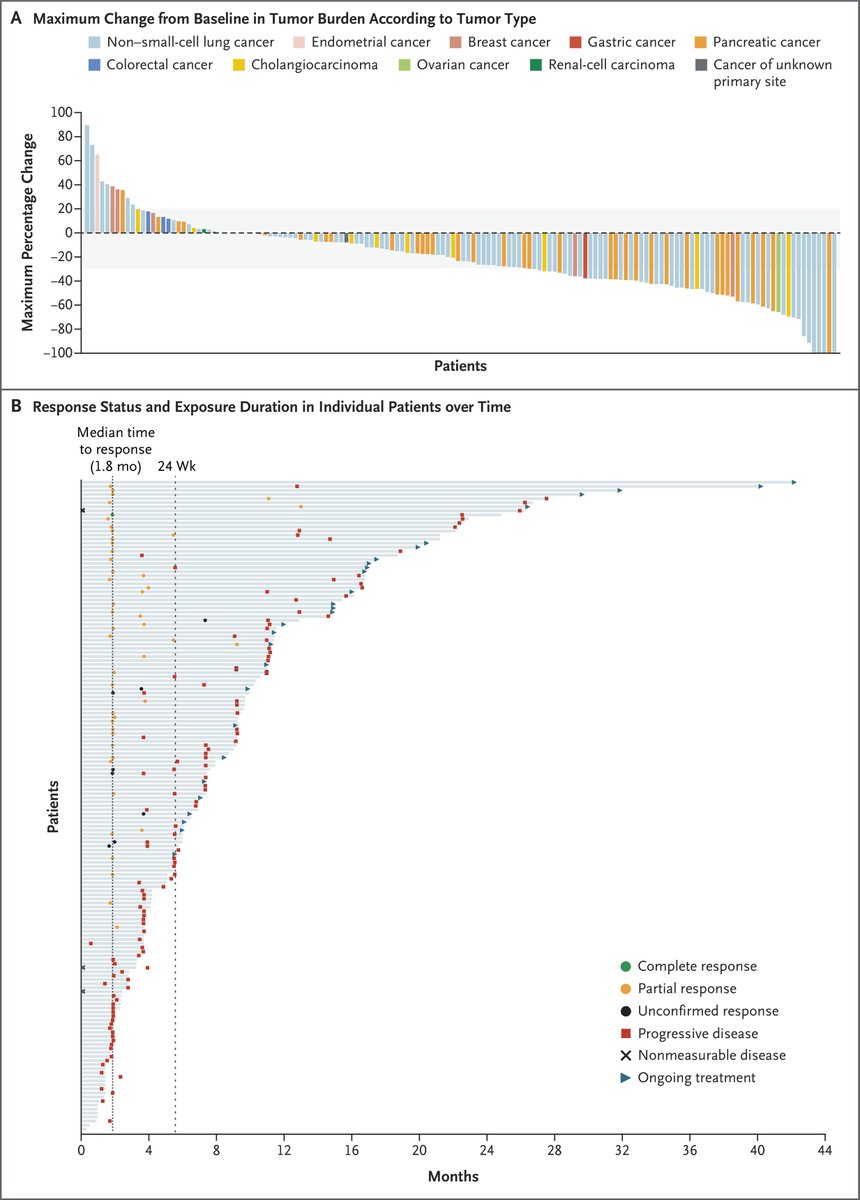
Efficacy of Zenocutuzumab in NRG1 Fusion–Positive Cancer
@NEJM
https://t.co/6ZJP3uCU5K
🔎Ph2-2, 204 pts, 12 tumor types
👉 bispecific antibody against HER2 & HER3,
👉ORR 30%, DoR 11.1 mo, mPFS 6.8 mo
👉ORR 40% in #PDAC, 20% in BTC
🧐Effective..
@myESMO@EASLedu@ILCAnews
See also 👇
Impact of pre-transplant immune checkpoint inhibitor use on post-transplant outcomes in HCC: A systematic review and individual patient data meta-analysis
Just published today in @JHepatology
https://t.co/Wfv9EEHbel
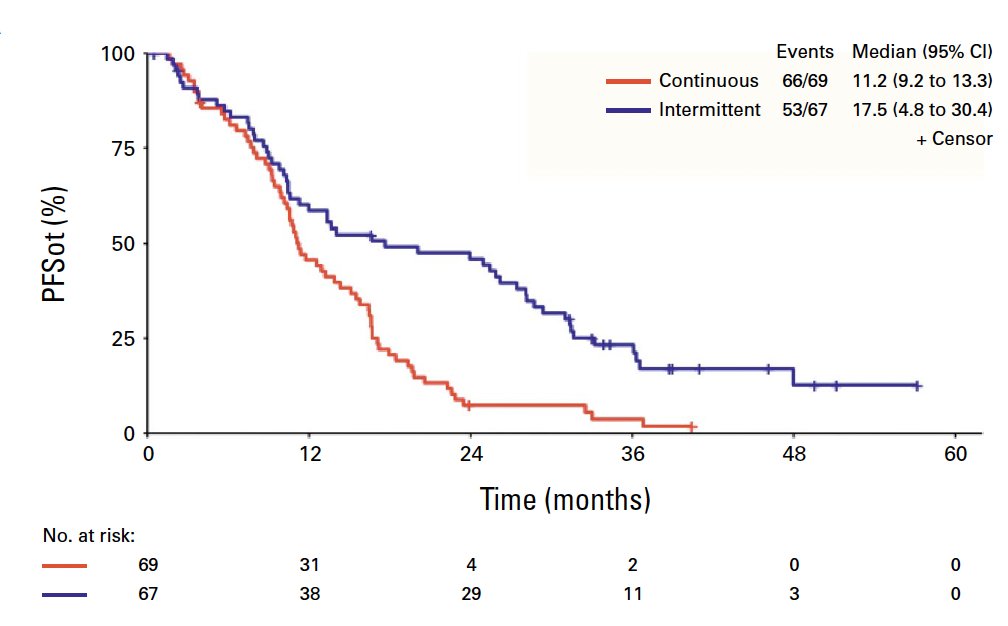
Intermittent or Continuous Panitumumab + FOLFIRI for RAS and BRAF WT CRC
@JCO_ASCO
https://t.co/z6tMwFjBnM
🔎IMPROVE phs-3
👉ORR 68.1% vs 61.2%,
👉mPFS 11.2 vs 17.5 mo, left-sided w/ delayed resistance
👉mOS 36.3 vs 35.1 mo
🧐Deescalation is feasible, less tox
@myESMO
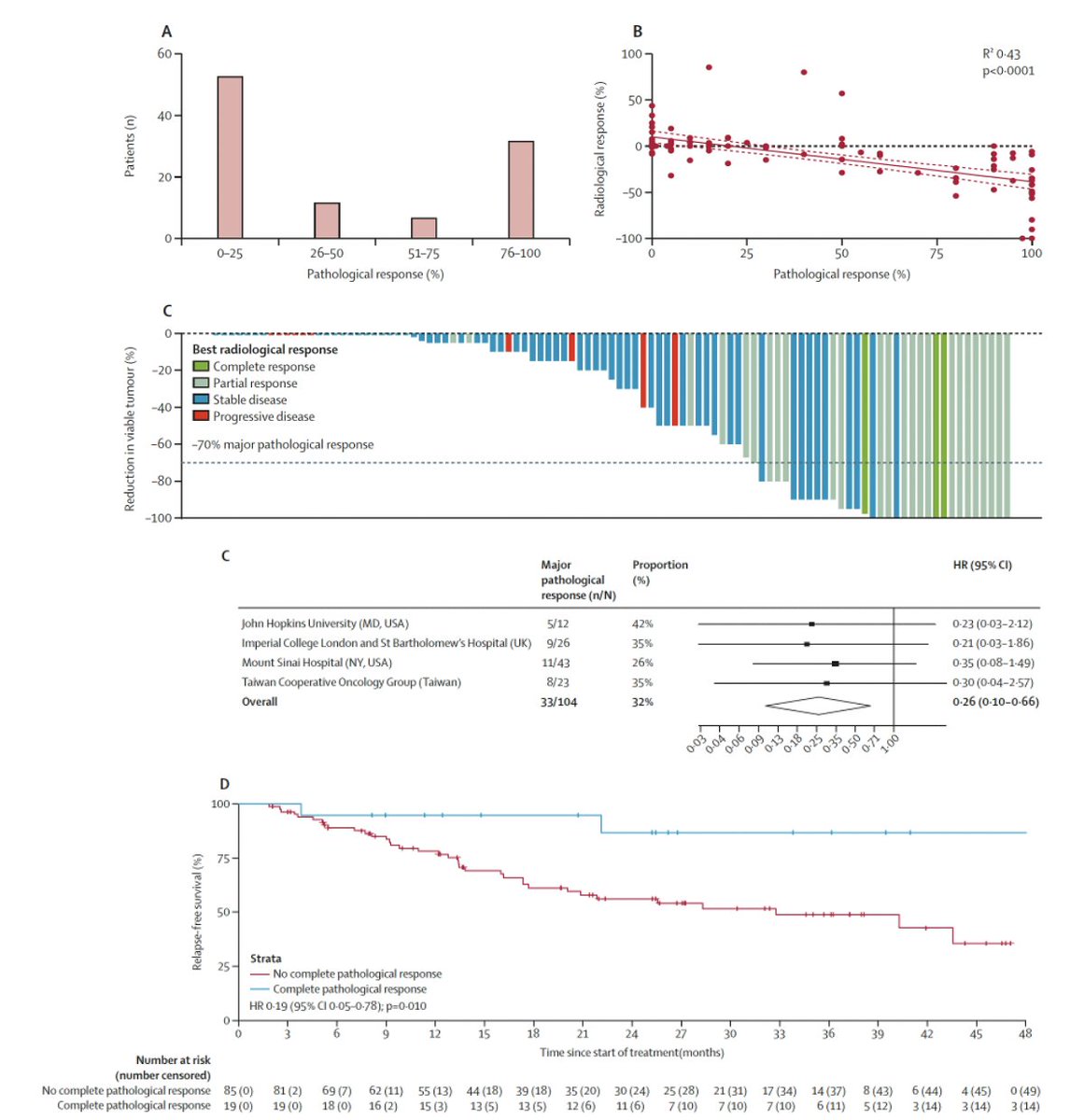
Pathological response following neoadjuvant immune checkpoint inhibitors in HCC: a cross-trial, patient-level analysis
@TheLancetOncol
https://t.co/0vZEXh9Qxj
👉111 pts, 1.4 mo neoadj. 💊
👉MPR: 32%, PCR 18%
👉Best threshold 90%
🧐Neoadj ICI is the way to go
@ILCAnews@EASLedu@myESMO #livertwitter
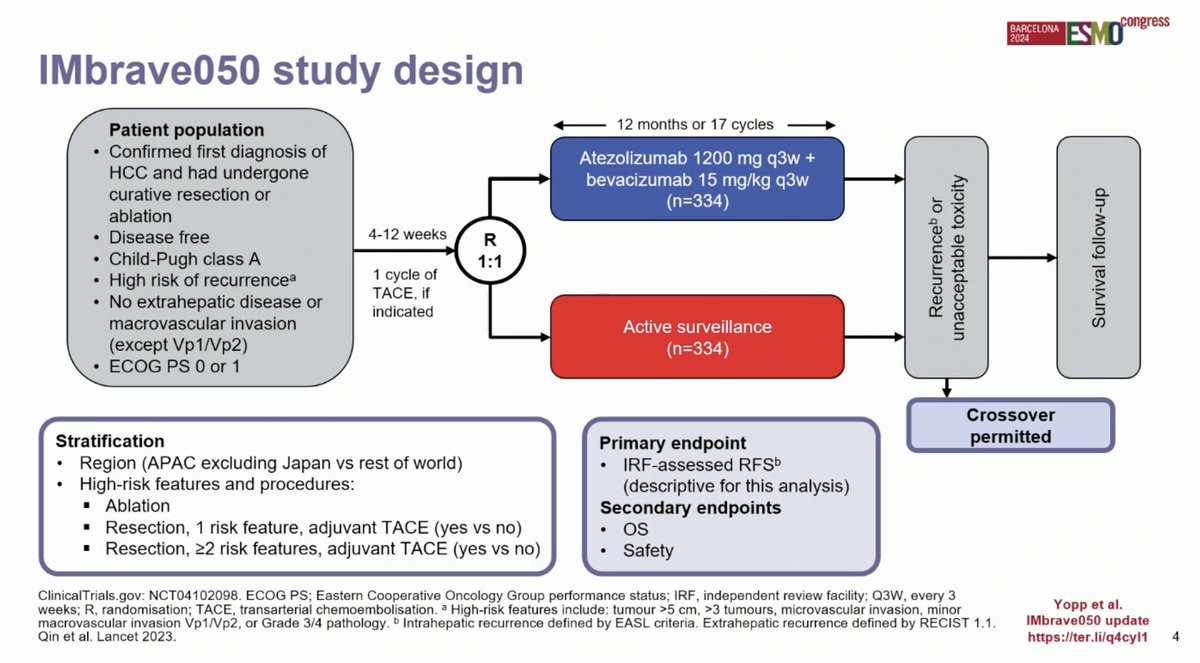
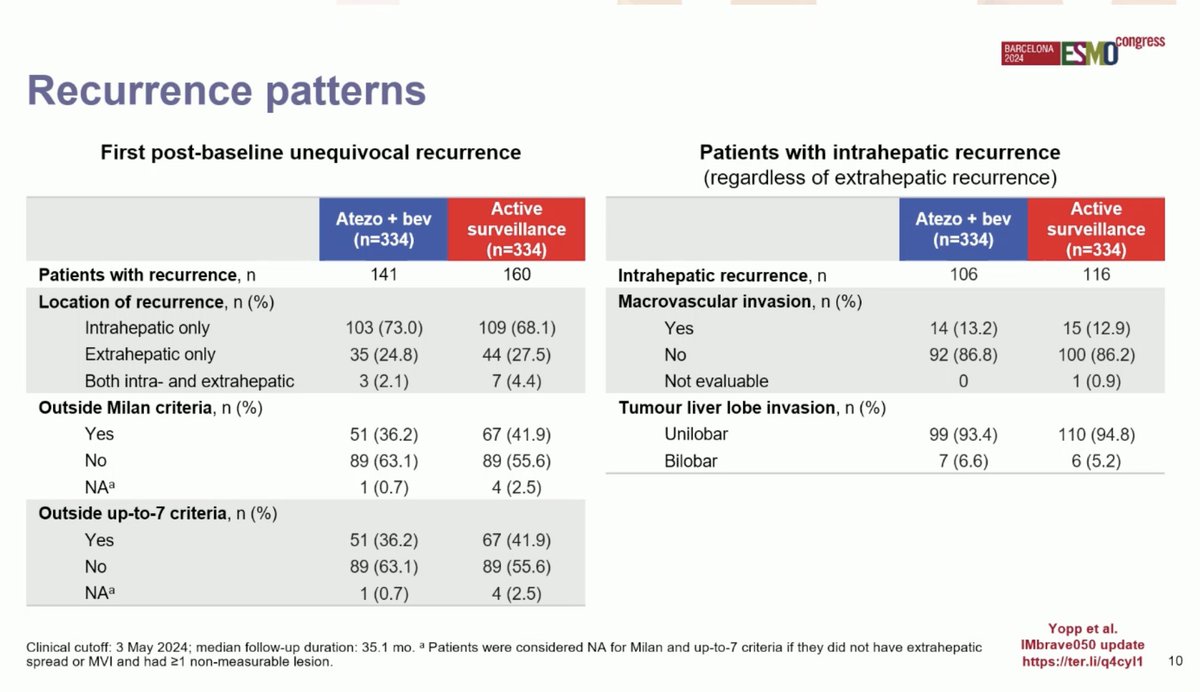
Updated data for atezo + bev vs surveillance in resected or ablated high risk HCC
#ESMO24
🔎IMbrave050
👉RFS 33.2 vs 36 mo, HR 0.9
👉OS: HR: 1.26
🧐Benefit not sustained! Disappointing..
🧐Caveat of (too) early read outs…
@myESMO#ESMOAmbassadors@ILCA@EASLedu
Anlotinib plus penpulimab vs sorafenib as 1L for HCC
#ESMO24
🔎Phs III ALTN-AK105-III-02
👉mPFS 6.9 vs 2.8 mo
👉mOS 16.5 vs 13.2 mo
🧐In line w/ prior anti-VEGF/ICI trials, not better...
🧐Who many VEGF/ICI combos do we need in 1st line?
@myESMO#ESMOAmbassadors@ILCA@EASLedu
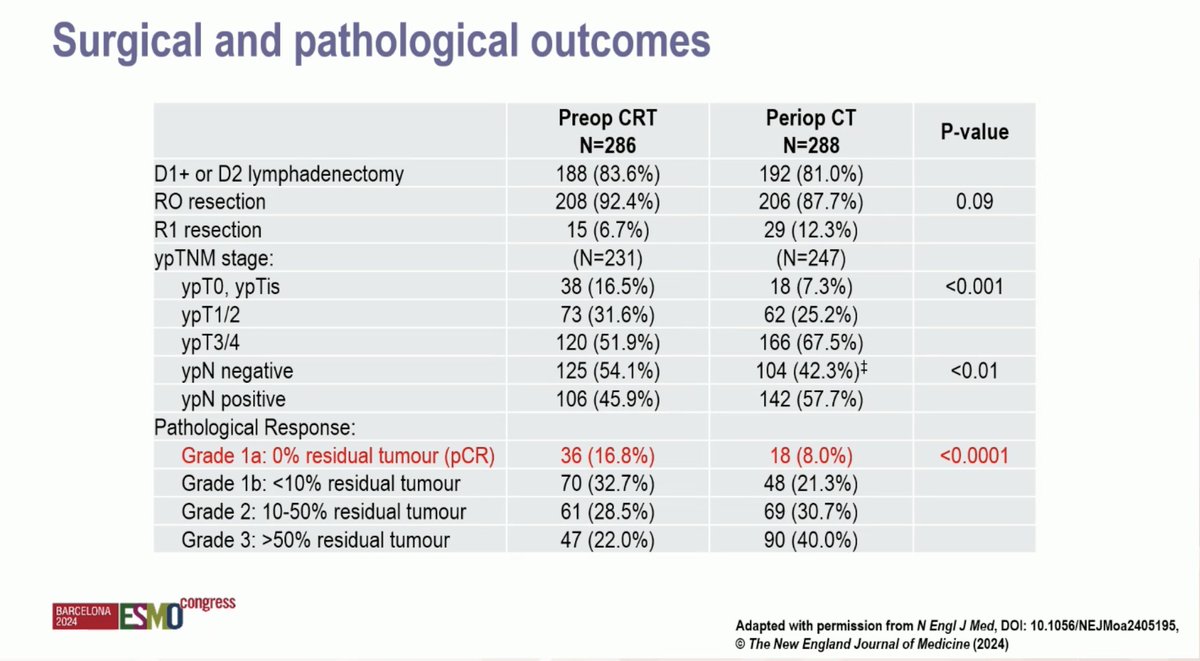
Periop CTx with or without preop CRT for resectable gastric cancer
#ESMO24
🔎AGITG TOPGEAR phs-III, 574 pts
👉 33% FLOT
👉pCR 167vs 78%
👉PFS 31 vs 31 mo
👉mOS 46 vs 49 mo
🧐Adding preOP CRT improves pCR rate & downstaging, but not survival
@myESMO#ESMOAmbassadors
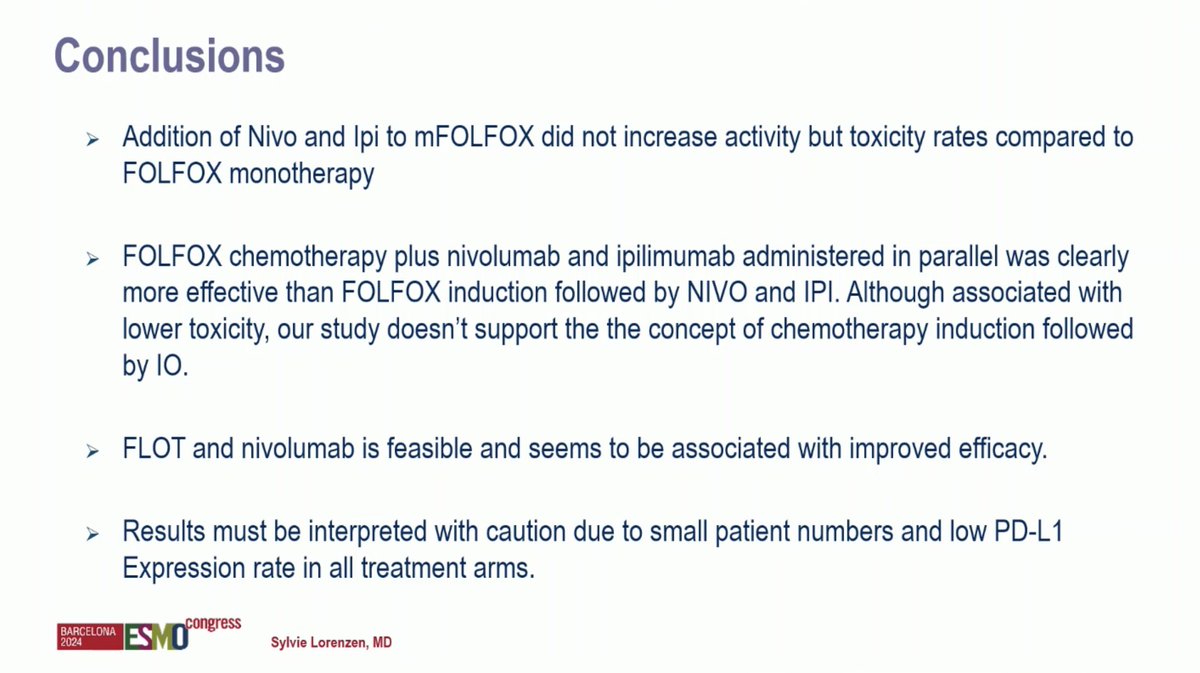
mFOLFOX plus/minus Nivo & Ipi vs FLOT + nivolumab in metastatic G/GEJ adenocarcinoma
#ESMO24
🔎IKF-AIO-Moonlight trial
👉ORR 46 vs 32 vs 47 vs 56%
👉PFS: 5,8 vs 4 vs 6,6 vs 7 mo
👉mOS: 10 vs 7,6 vs 12,5 vs 14,6 mo
🧐Only FLOT + Nivo seems feasible & effective
@myESMO #ESMOAmbassadors
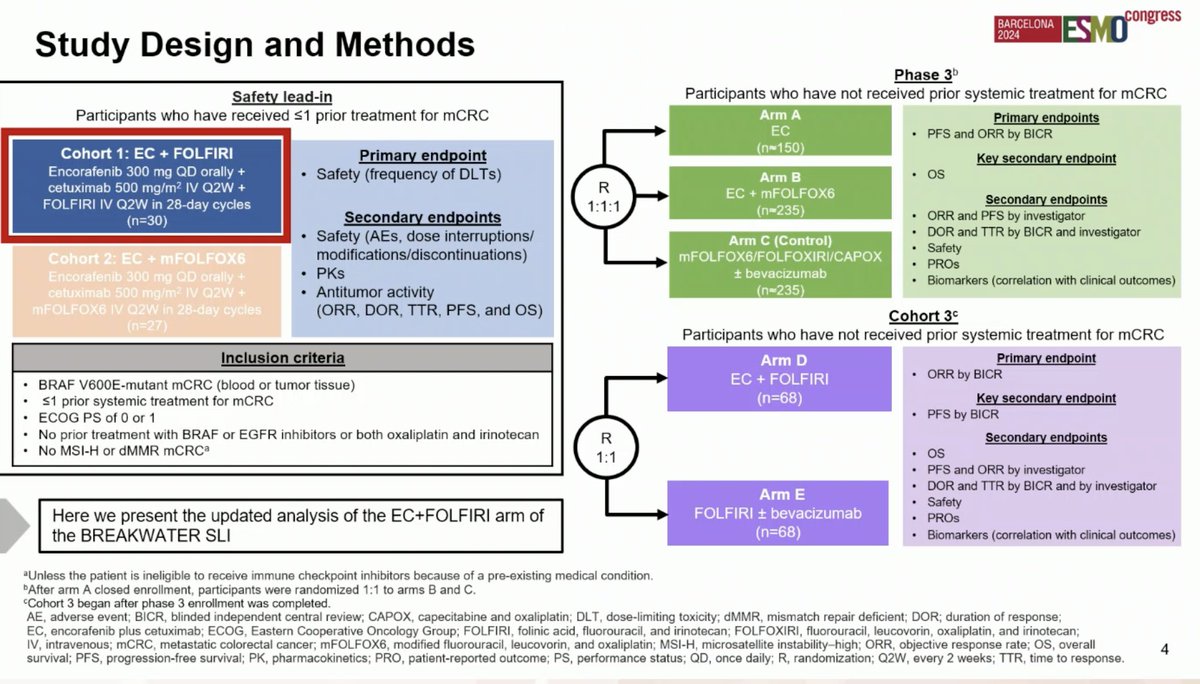
Encorafenib + cetuximab + FOLFIRI for BRAF V600E-mCRC
#ESMO24
🔎BREAKWATER safety lead-in, 30 pts, 1L and 2L
👉mPFS NE vs 12.6 mo
👉mOS NE vs 19.7
👉AE ≥3 63%, mainly GI tox
🧐Promising efficacy in 1L, no new safety signal
@myESMO#ESMOAmbassadors
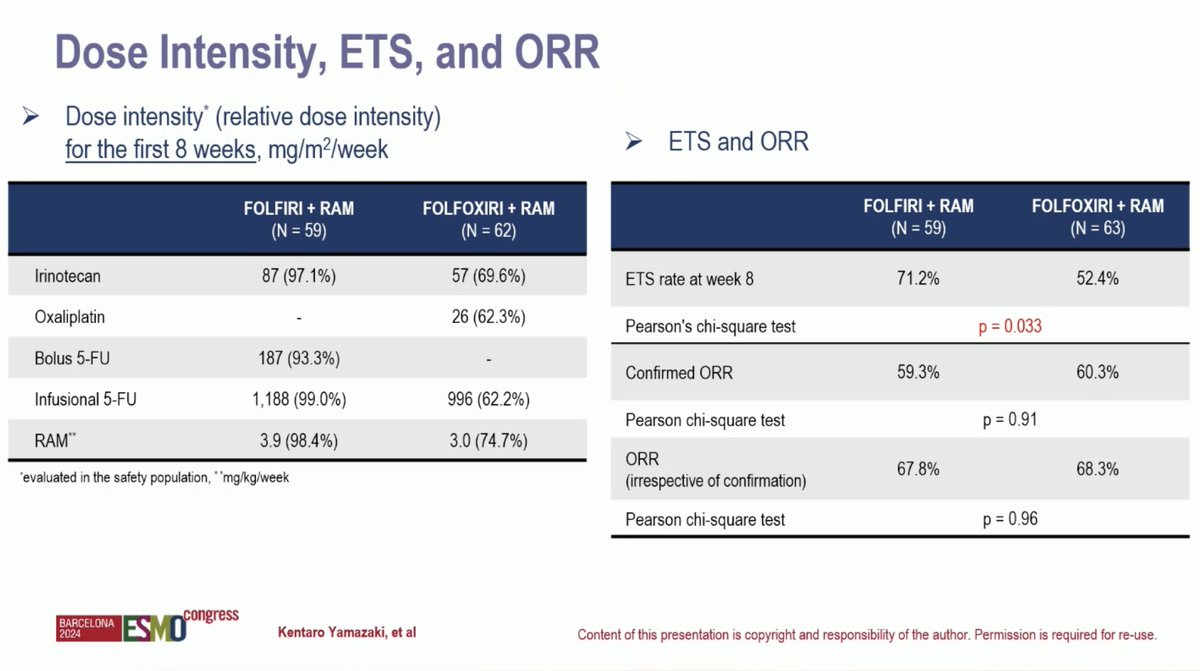
FOLFIRI plus ramucirumab vs FOLFOXIRI plus RAM as 1L treatment for mCRC
#ESMO24
🔎RECAST phs 2, 122. pts,
👉ORR 60 vs 60%
👉mPFS 11 vs 10.5 mo
👉mOS 32 vs 28 mo
👉Surgery 25 vs 15%
🧐No benefit for FOLFOXIRI, numerically worse...
@myESMO#ESMOAmbassadors
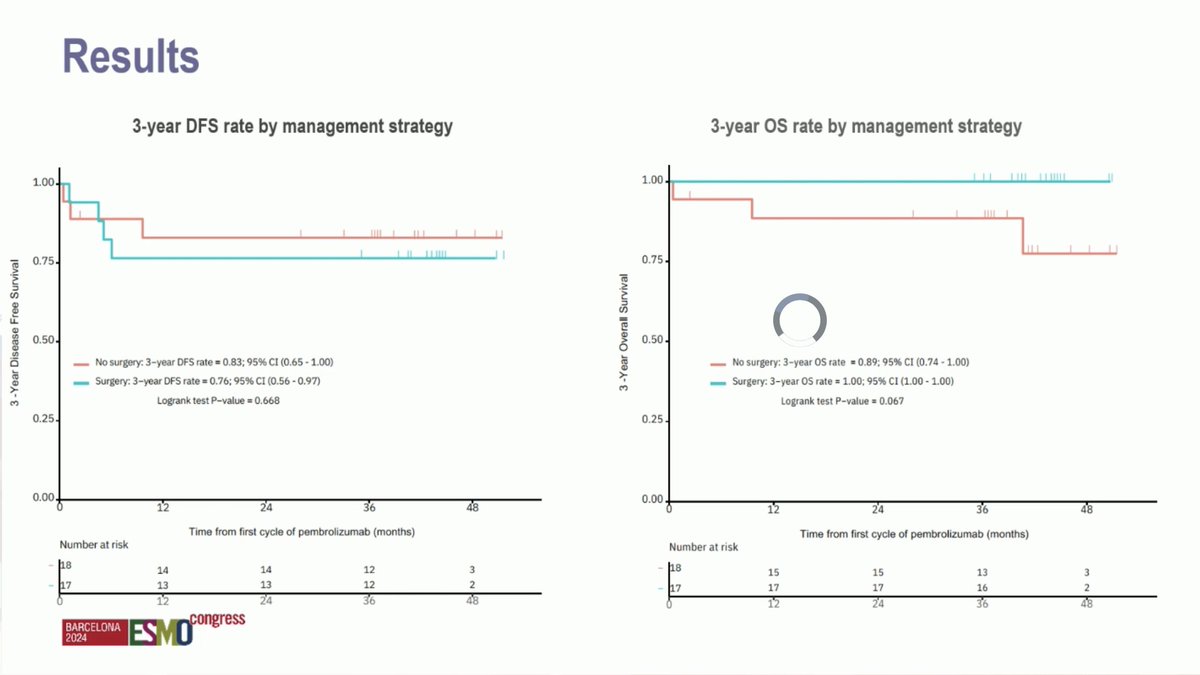
LT survival & organ preservation with pembrolizumab in localized MSI solid tumors
👉17/17 resected patients remain cancer free
👉14/18 non-operative patients alive with organ intact
👉Clearence of ctDNA predict outcome
👉Excellent RFS & OS
@myESMO#ESMOAmbassadors