Buen trabajo que parece mostrar cuál es el nivel ideal de potasio seríco en pacientes con IC.
No parece lo mismo según el perfil del paciente
https://t.co/FXG28oX9Ju
The gap between evidence and practice:
• BB: proven 1996 → use rate 73%
• ARNI: proven 2014 → use rate 67%
• MRA: proven 1999 → use rate 36%
• SGLT2i: proven 2019 → use rate 34%
• All 4: use rate 18%
This is the defining implementation failure of modern cardiology.
How do you handle patient selection for VA ECMO in pulmonary embolism? See our systematic review & guide to patient selection in @JCFINT!
🚦Green/Yellow/Red triage: Structured guidance to avoid futile cannulation while acting early.
🫁Why avoiding sedation/intubation is vital to prevent cardiovascular collapse.
🩸Hybrid ECMO with clot removal strategies.
👉https://t.co/s3BbsrTvp0
We quantitatively assessed the degree of echogenicity in the proximal and mid segments of both coronary arteries to determine its additional diagnostic value in 109 patients with clinically suspected Kawasaki disease.
Read our @JournalASEcho article: https://t.co/fYoKY23ayt
🌳 DECISION/DIGIT-HF/DIG — Study-level meta-analysis (~9,000 patients)
When you pool all the digitalis glycoside RCT evidence, the picture becomes much clearer. Presented by Kevin Damman at #HeartFailure26
📊 Primary endpoint (CV death or first worsening HF event):
• DIG (1997): HR 0.85 [0.79–0.91]
• DIGIT-HF (2025): HR 0.85 [0.71–1.02]
• DECISION (2026): HR 0.83 [0.66–1.05]
• OVERALL: HR 0.85 [0.80–0.90], P < 0.001 ✓
I² = 0% — zero heterogeneity
📊 Secondary endpoints:
✅ First worsening HF event: HR 0.75 (0.75–0.81), P < 0.001
❌ CV death: HR 0.99 (0.92–1.07), P = 0.81
✅ All-cause death or worsening HF: HR 0.85 (0.80–0.90), P < 0.001
❌ All-cause death: HR 0.97 (0.90–1.04), P = 0.41
🔑 The meta-analytic verdict:
✅ Digitalis reduces HF events & composite outcomes significantly
❌ No mortality benefit (CV or all-cause)
✅ Zero heterogeneity — consistent effect across all three trials, eras, and doses
The drug works for congestion & worsening HF. It doesn't extend life. That's the honest summary of ~30 years of evidence.
#Digoxin #DIG #DIGITHF #DECISION #MetaAnalysis #HeartFailure2026 #CardioTwitter
Unexplained dyspnea? Here’s the new ESC framework for diagnosing HFpEF — and it goes way beyond a basic echo 🧵
From Landsteiner et al., Eur Heart J 2026, a stepwise domain-based approach
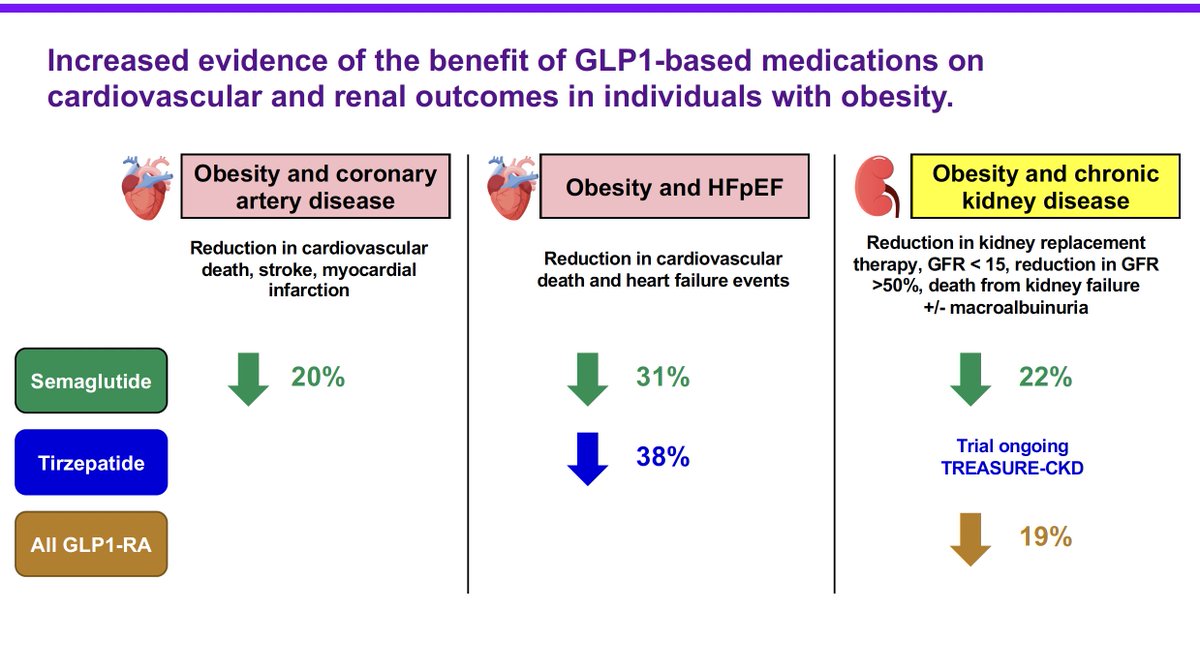
Fantastic summary of #obesity care at the intersection of ❤️ disease and kidney disease from @MWeintraubMD at the @columbia@Weillcornell Obesity #Medicine Conference 👉 https://t.co/PglY7gk82X
If you missed this, on-demand recordings will be available after the course ends tomorrow!
#CKD #CVD #cardiotwitter #health #metabolism #CKM
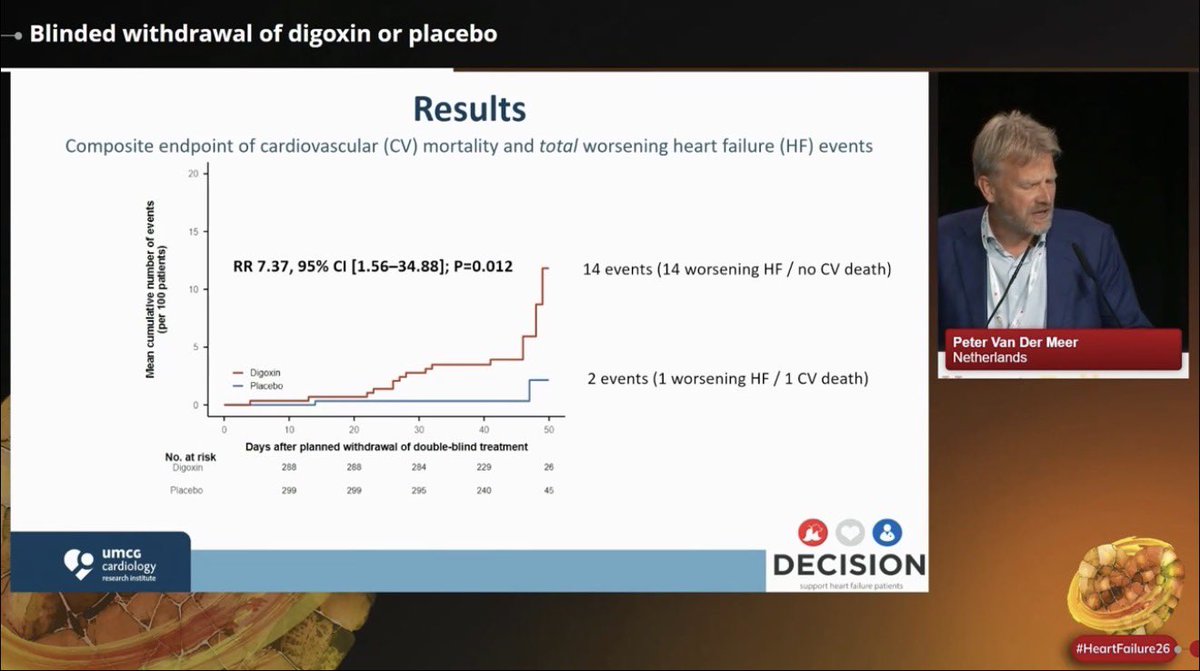
🫀 What happens when long-term low-dose #digoxin is suddenly withdrawn?
Blinded withdrawal analysis from the #DECISION trial presented at #HeartFailure26 by Prof. Peter van der Meer:
📍Digoxin withdrawal was associated with a ~7x increase in worsening HF events over just 6 weeks
📍14 worsening HF events occurred after digoxin withdrawal vs only 2 events in placebo withdrawal
📍Withdrawal was accompanied by: ⬆️HR,⬇️ SBP, ⬆️NT-proBNP, ⬇️eGFR
📍⚠️caution when stopping long-term low-dose digoxin in pts with HF & LVEF <=50%
@escardio@HFA_President@jozinetm
The potassium concern with MRAs — how real is it? 🫀
#HeartFailure26 | Anne-Christine Ruwald
Jhund et al. Lancet 2024
Across RALES, EMPHASIS-HF, TOPCAT and FINEARTS-HF:
⚠️ Severe hyperkalaemia (>6.0 mmol/L):
• RALES: 4% vs 1% (OR 3.75)
• EMPHASIS-HF: 3% vs 2% (OR 1.37)
• TOPCAT: 2% vs 1% (OR 2.53)
• FINEARTS-HF: 3% vs 2% (OR 2.07)
Real signal — but absolute rates remain low (<5%) across all trials.
✅ The other side of the coin — hypokalaemia (<3.5 mmol/L):
• MRA halved hypokalaemia rates: 7% vs 14% (FINEARTS-HF: 5% vs 10%)
This matters. Hypokalaemia in HF is dangerous — arrhythmias, sudden death.
MRAs increase hyperkalaemia risk modestly, but significantly protect against hypokalaemia.
The net potassium balance may actually favour MRA use in selected patients — particularly those at risk of low potassium on loop diuretics.
Monitor potassium. Don’t fear MRAs.
#MRA #Finerenone #HFpEF #Hyperkalaemia #HeartFailure #Cardiology #ESC #HeartFailure26
⚠️ Low BP in HFrEF — should it stop us from using GDMT? Data says: probably not.
From COPERNICUS, PARADIGM-HF, RALES/EMPHASIS-HF & DAPA-HF:
✅ Carvedilol beneficial even at SBP 85–95 mmHg
✅ Sacubitril/Valsartan consistent across all BP strata
✅ MRA & SGLT2i similarly effective in low BP groups
Low SBP is a reason to be careful — not a reason to stop. 💡
#HeartFailure26 #HF2026 #HFrEF #GDMT #Cardiology
🙌 Our last manuscript is out.
👉“Safety of Very Low LDL-Cholesterol:
Ten Common Concerns, Misconceptions, and Evidence-Based Clarifications”
📍Very low LDL-C levels continue to generate debate, fear, and misinformation in clinical practice.
📍In this review, we critically examined 10 of the most frequent concerns related to intensive LDL-C lowering:
— Cognitive decline
— Hemorrhagic stroke
— Cancer
— Cataracts
— Hormonal dysfunction
— Diabetes risk
— Muscle symptoms
— Older adults
— Sex differences
— Overall cardiovascular benefit
📍The key message is clear:
RCTs, meta-analyses, and genetic evidence consistently support the safety profile of very low achieved LDL-C levels in appropriately selected high-risk patients.
📍Some adverse effects are real — particularly statin-associated dysglycemia and muscle symptoms — but their absolute risk is generally modest compared with the magnitude of ASCVD risk reduction.
📍Therapeutic inertia and misinformation remain major barriers in preventive cardiology. Evidence-based communication matters.
📍Lower LDL-C. Earlier. Longer. Safer than many still believe.
☝️Proud to collaborate with outstanding colleagues from Latin America, Europe, and beyond in this international effort.
🔗 https://t.co/zEMcECn9El
@society_eas@ATHjournal
Are all MRAs equal? Short answer: no. 🫀
#HeartFailure26 | Anne-Christine Ruwald
Harrington JL et al. JACC Heart Fail. 2025;13(10):102637
Steroidal MRAs (spironolactone, eplerenone) vs Non-steroidal MRAs (finerenone, balcinrenone, aparenone, esaxerenone)
Key differences:
🔵 Steroidal MRAs:
• Higher binding in kidneys vs heart
• More off-target binding → increased side effects (gynecomastia, hyperkalemia)
• Clinical data: benefit in HFrEF ✅ | Role in HFpEF unclear ❓
🟠 Non-steroidal MRAs:
• More even distribution between heart and kidneys
• More potent MR antagonism
• Clinical data: Role in HFrEF unclear ❓ | Benefit in HFpEF ✅
The pharmacological differences are not trivial — tissue distribution, specificity, potency, and tolerability all differ.
Fascinating inversion: sMRAs work in HFrEF, ns-MRAs work in HFpEF. Same target, different patients, different drugs.
The MRA class is not one-size-fits-all.
#MRA #Finerenone #HFpEF #HFrEF #HeartFailure #Cardiology #ESC #HeartFailure26
🫀🧠Atrial fibrillation detected after stroke or TIA (AFDAS): A systematic review and meta-analysis
📊AFDAS common but prevalence varied depending on monitoring duration and modality
Read more here!👇 https://t.co/NJjK1CLz35 @ghassaba03
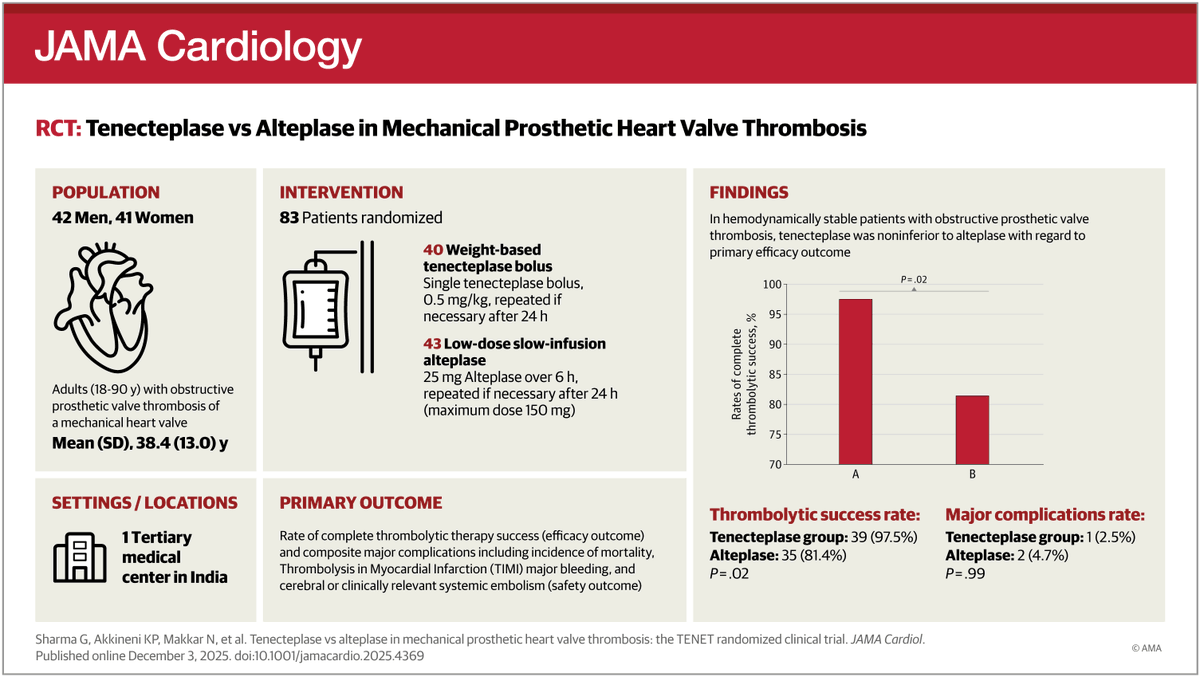
RCT: Among patients with obstructive prosthetic heart valve thrombosis, tenecteplase achieved higher complete thrombolytic success (97.5%) than alteplase (81.5%) and a shorter hospital stay. https://t.co/5XoQ6k29v2
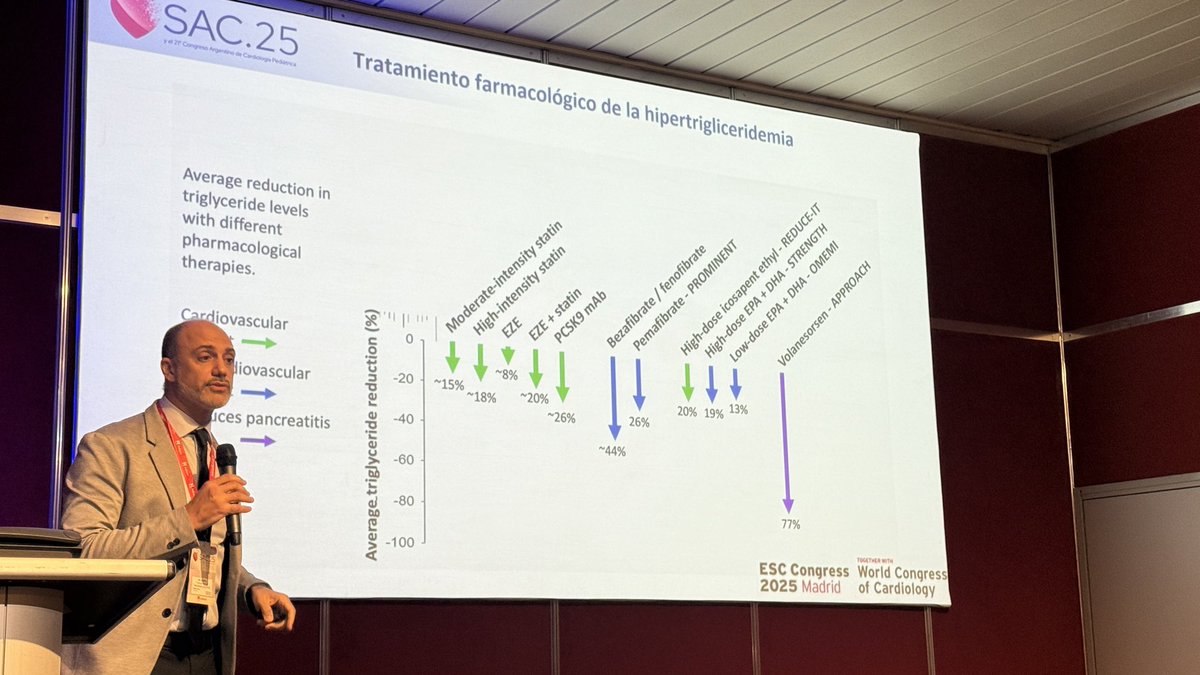
Congreso #SAC25
Los únicos fármacos que reducen triglicéridos y que demostraron beneficio 🫀 son aquellos que incluyen estatinas (⬇️LDL) e eicosapento de etilo
LOS FIBRATOS NO HAN DEMOSTRADO BENEFICIO CARDIOVASCULAR
Dr. @ezeforte@SAC_54






![drbennisahmed's tweet photo. 🌳 DECISION/DIGIT-HF/DIG — Study-level meta-analysis (~9,000 patients)
When you pool all the digitalis glycoside RCT evidence, the picture becomes much clearer. Presented by Kevin Damman at #HeartFailure26
📊 Primary endpoint (CV death or first worsening HF event):
• DIG (1997): HR 0.85 [0.79–0.91]
• DIGIT-HF (2025): HR 0.85 [0.71–1.02]
• DECISION (2026): HR 0.83 [0.66–1.05]
• OVERALL: HR 0.85 [0.80–0.90], P < 0.001 ✓
I² = 0% — zero heterogeneity
📊 Secondary endpoints:
✅ First worsening HF event: HR 0.75 (0.75–0.81), P < 0.001
❌ CV death: HR 0.99 (0.92–1.07), P = 0.81
✅ All-cause death or worsening HF: HR 0.85 (0.80–0.90), P < 0.001
❌ All-cause death: HR 0.97 (0.90–1.04), P = 0.41
🔑 The meta-analytic verdict:
✅ Digitalis reduces HF events & composite outcomes significantly
❌ No mortality benefit (CV or all-cause)
✅ Zero heterogeneity — consistent effect across all three trials, eras, and doses
The drug works for congestion & worsening HF. It doesn't extend life. That's the honest summary of ~30 years of evidence.
#Digoxin #DIG #DIGITHF #DECISION #MetaAnalysis #HeartFailure2026 #CardioTwitter](https://pbs.twimg.com/media/HH9IuVlWQAAeeEr.jpg)
![drbennisahmed's tweet photo. 🌳 DECISION/DIGIT-HF/DIG — Study-level meta-analysis (~9,000 patients)
When you pool all the digitalis glycoside RCT evidence, the picture becomes much clearer. Presented by Kevin Damman at #HeartFailure26
📊 Primary endpoint (CV death or first worsening HF event):
• DIG (1997): HR 0.85 [0.79–0.91]
• DIGIT-HF (2025): HR 0.85 [0.71–1.02]
• DECISION (2026): HR 0.83 [0.66–1.05]
• OVERALL: HR 0.85 [0.80–0.90], P < 0.001 ✓
I² = 0% — zero heterogeneity
📊 Secondary endpoints:
✅ First worsening HF event: HR 0.75 (0.75–0.81), P < 0.001
❌ CV death: HR 0.99 (0.92–1.07), P = 0.81
✅ All-cause death or worsening HF: HR 0.85 (0.80–0.90), P < 0.001
❌ All-cause death: HR 0.97 (0.90–1.04), P = 0.41
🔑 The meta-analytic verdict:
✅ Digitalis reduces HF events & composite outcomes significantly
❌ No mortality benefit (CV or all-cause)
✅ Zero heterogeneity — consistent effect across all three trials, eras, and doses
The drug works for congestion & worsening HF. It doesn't extend life. That's the honest summary of ~30 years of evidence.
#Digoxin #DIG #DIGITHF #DECISION #MetaAnalysis #HeartFailure2026 #CardioTwitter](https://pbs.twimg.com/media/HH9IuVkXEAQLVom.jpg)
![drbennisahmed's tweet photo. 🌳 DECISION/DIGIT-HF/DIG — Study-level meta-analysis (~9,000 patients)
When you pool all the digitalis glycoside RCT evidence, the picture becomes much clearer. Presented by Kevin Damman at #HeartFailure26
📊 Primary endpoint (CV death or first worsening HF event):
• DIG (1997): HR 0.85 [0.79–0.91]
• DIGIT-HF (2025): HR 0.85 [0.71–1.02]
• DECISION (2026): HR 0.83 [0.66–1.05]
• OVERALL: HR 0.85 [0.80–0.90], P < 0.001 ✓
I² = 0% — zero heterogeneity
📊 Secondary endpoints:
✅ First worsening HF event: HR 0.75 (0.75–0.81), P < 0.001
❌ CV death: HR 0.99 (0.92–1.07), P = 0.81
✅ All-cause death or worsening HF: HR 0.85 (0.80–0.90), P < 0.001
❌ All-cause death: HR 0.97 (0.90–1.04), P = 0.41
🔑 The meta-analytic verdict:
✅ Digitalis reduces HF events & composite outcomes significantly
❌ No mortality benefit (CV or all-cause)
✅ Zero heterogeneity — consistent effect across all three trials, eras, and doses
The drug works for congestion & worsening HF. It doesn't extend life. That's the honest summary of ~30 years of evidence.
#Digoxin #DIG #DIGITHF #DECISION #MetaAnalysis #HeartFailure2026 #CardioTwitter](https://pbs.twimg.com/media/HH9IuVjW0AMEda7.jpg)






























![drbennisahmed's tweet photo. 🌳 DECISION/DIGIT-HF/DIG — Study-level meta-analysis (~9,000 patients)
When you pool all the digitalis glycoside RCT evidence, the picture becomes much clearer. Presented by Kevin Damman at #HeartFailure26
📊 Primary endpoint (CV death or first worsening HF event):
• DIG (1997): HR 0.85 [0.79–0.91]
• DIGIT-HF (2025): HR 0.85 [0.71–1.02]
• DECISION (2026): HR 0.83 [0.66–1.05]
• OVERALL: HR 0.85 [0.80–0.90], P < 0.001 ✓
I² = 0% — zero heterogeneity
📊 Secondary endpoints:
✅ First worsening HF event: HR 0.75 (0.75–0.81), P < 0.001
❌ CV death: HR 0.99 (0.92–1.07), P = 0.81
✅ All-cause death or worsening HF: HR 0.85 (0.80–0.90), P < 0.001
❌ All-cause death: HR 0.97 (0.90–1.04), P = 0.41
🔑 The meta-analytic verdict:
✅ Digitalis reduces HF events & composite outcomes significantly
❌ No mortality benefit (CV or all-cause)
✅ Zero heterogeneity — consistent effect across all three trials, eras, and doses
The drug works for congestion & worsening HF. It doesn't extend life. That's the honest summary of ~30 years of evidence.
#Digoxin #DIG #DIGITHF #DECISION #MetaAnalysis #HeartFailure2026 #CardioTwitter](https://pbs.twimg.com/media/HH9IuVlW4AAVYD8.jpg)