Why we shouldn't write only EPS.
That word is convenient, but clinically it is not enough.
Acute dystonia, akathisia, drug-induced parkinsonism and tardive dyskinesia may all follow dopamine-receptor blocking drugs, but they are not the same problem and should not be treated as one.
The simplest way I understand them is this:
Antipsychotics are prescribed mainly for their effect on dopamine signalling involved in psychosis.
But the drug does not act only there.
When dopamine D2 signalling is also reduced in the nigrostriatal system, movement can change.
What appears depends on the patient, the drug, the dose, the speed of dose escalation and the duration of exposure.
Soon after starting or increasing the drug, a patient may develop a painful twisted neck, jaw spasm or upward deviation of the eyes.
That is acute dystonia.
The exact mechanism is more complex than simply low dopamine, but an acute dopaminergic-cholinergic imbalance within the basal ganglia is a useful clinical model.
Another patient becomes slow.
The face loses expression.
The arms stop swinging.
There is rigidity, tremor or a short-stepped gait.
That is drug-induced parkinsonism.
Here the nigrostriatal dopamine blockade produces a Parkinson-like motor state.
Then there is the patient who cannot sit.
He keeps moving his legs, gets up repeatedly and walks around the room.
He may call it anxiety because he has no better word for it.
This is akathisia.
Its biology is not completely understood, but clinically the danger is clear:
Akathisia is frequently mistaken for agitation or worsening psychosis.
Increasing the antipsychotic in that situation may worsen the very problem we are trying to treat.
Months or years later, some patients develop repeated mouth, tongue, facial, truncal or limb movements.
That is tardive dyskinesia.
Chronic dopamine-receptor blockade may produce maladaptive changes in motor circuits, including dopamine-receptor hypersensitivity, but this is not the whole story.
Tardive dyskinesia is probably multifactorial.
That is why one explanation cannot account for every patient and why treatment differs from acute dystonia or parkinsonism.
So I no longer stop at the word EPS.
I ask:
What exactly is the movement?
When did it begin in relation to the drug?
Was there a recent dose increase?
Can the patient voluntarily suppress it?
Is there inner restlessness?
Is the patient slow, rigid, twisted or producing extra movements?
And most importantly:
Could my treatment for one movement disorder worsen another?
Before the patient speaks, I watch them enter the room, sit down, keep their hands on the lap, move the tongue and walk back to the door.
The prescription tells me what the patient received.
The movement examination tells me what the brain is experiencing.
Never treat EPS as one diagnosis.
Name the movement first.
#Neurology #Psychiatry #MovementDisorders #ClinicalMedicine #Neurotwitter #MedX
62% of Indian resident doctors work more than 36 hours at a stretch. 86% report severe sleep deprivation. 97% earn less than an entry level civil servant. 76% are assaulted while on duty.
We can call ourselves civilised only when we learn to treat our doctors like they treat us.
If a corporator thinks it’s okay to beat up a doctor, then the next time there’s a pothole in a road in his area, is it okay to beat him?
Asking for several friends
🧵 “Doctor, why is my BP still 190/110 despite 4 medicines?”
Because sometimes hypertension is NOT the disease.
It’s the symptom.
Clinical cases that reveal the hidden causes of SECONDARY HYPERTENSION 👇
A friend who had checked his Lp(a) -328 ( extreme elevation) got a Coronary calcium score (CAC) of Zero
Turns out that CAC only detects calcified plaque, which is usually more stable. The plaque most likely to cause an MI is more often soft, and a non-calcified plaque. That plaque can rupture long before it calcifies.
A zero CAC score does NOT rule that out.
To detect both calcified and soft plaque , you need a CCTA (Coronary CT Angiography). It shows plaque type, stenosis, and actual arterial narrowing.
Hence, if you are symptomatic , have strong risk factors, or elevated Lp(a), a zero CAC should not end the conversation.
Elevated Lp(a) especially promotes soft plaque formation, the exact kind CAC misses.
Comments?
I have outgrown a lot of friends and it's not even that they are bad friends. But people don't show up for you like you show up for them, so something has to give. Some friendships are only for a season, and that’s okay.
@DoctorLFC@nihardesai89 Udaipur was founded (in 1559) as a strategic backup capital by Maharana Udai Singh amidst the Aravalis when he was advised to move from Chittorgarh for safety. Although known as City of Lakes, all the beautiful lakes are man-made, heavily engineered through dams and canal systems
I once heard a line from Shah Rukh Khan that stayed with me;
“Jab time aapka bura chal raha ho, tab zyada haath-pair maarne ki ya har cheez par react karne ki zarurat nahi hoti. Bas shaant ho kar baith jao. Bura time hai, woh apne aap nikal jayega. Jo bhi aapka kaam hai, bas woh karte raho, lekin panic mat karo, overreact mat karo, aur har problem ko zabardasti turant fix karne ki koshish mat karo.”
And honestly, this might be one of the most practical pieces of wisdom.
When things go wrong, our instinct is to panic, react, overthink, and try to control everything.
But many times the smartest move is simply patience.
1. Stay calm
2. Keep doing your work
3. Don’t overreact
4. Let the bad phase pass
Because time changes everything.
Sometimes the storm doesn’t need you to fight it, it just needs you to sit still until it passes.
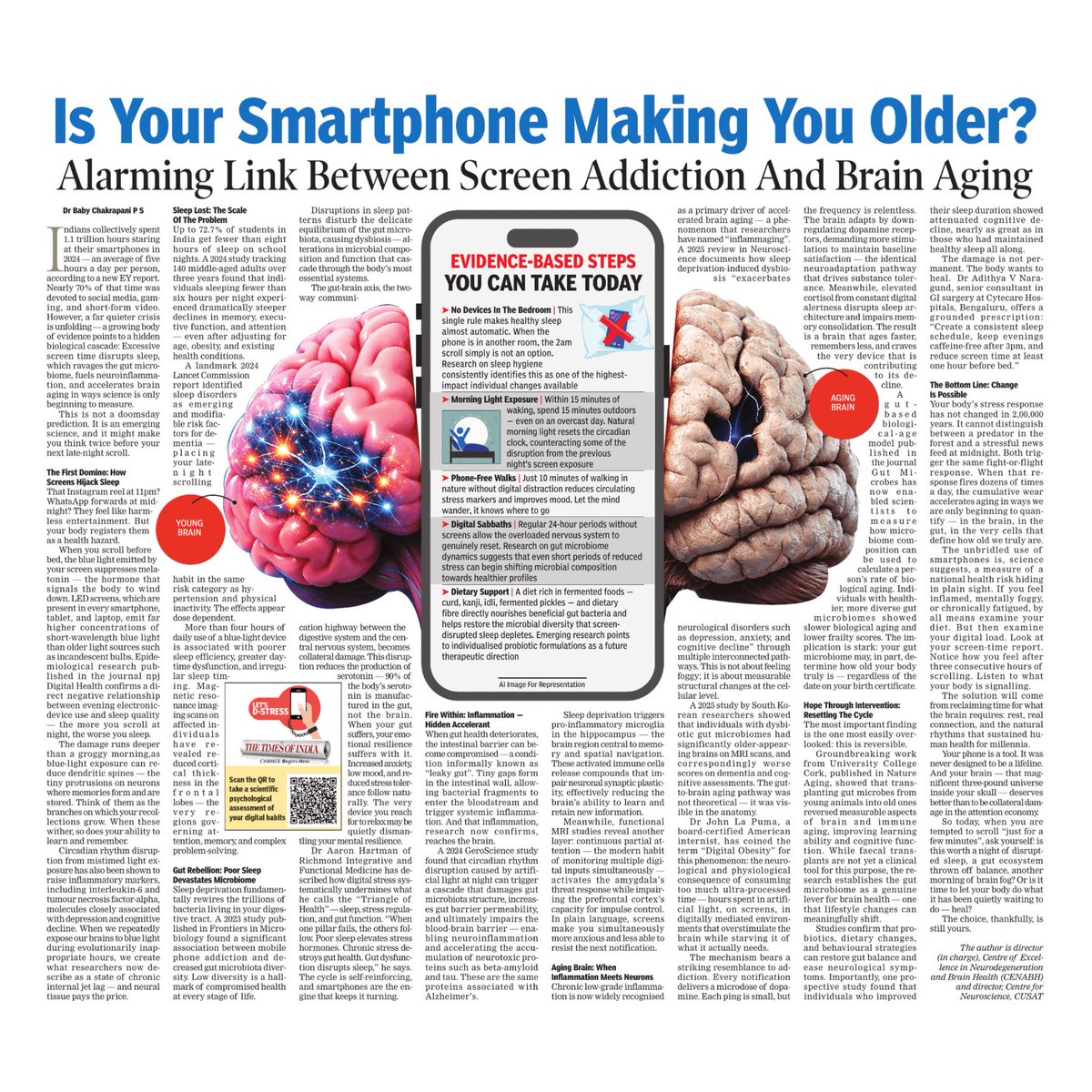
Could excessive screen time be doing more than just affecting your sleep?
Emerging research points to links between digital overuse, poor sleep cycles, inflammation and even accelerated brain ageing, making mindful screen habits more important than ever.
Read the story.
Take the scientific psychological assessment of your digital habits: https://t.co/vsgHBePlkW
#LetsDStress #TheTimesofIndia #DigitalWellbeing #ScreenAddiction #BrainHealth