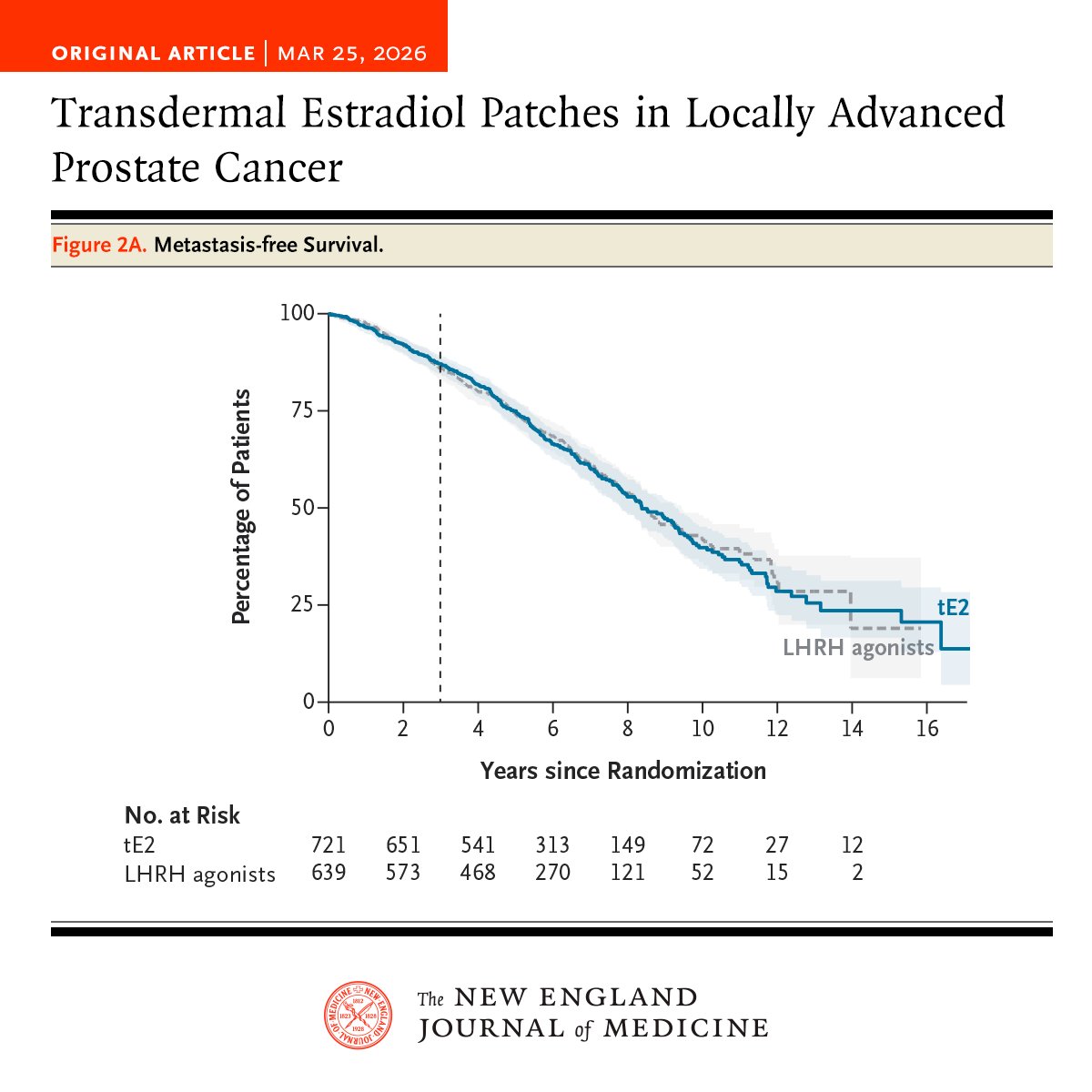
Among men with locally advanced prostate cancer, transdermal estradiol was noninferior to LHRH agonists for 3-year metastasis-free survival and led to a lower incidence of hot flashes but a higher incidence of gynecomastia. Full results of the STAMPEDE-1 and PATCH trials: https://t.co/sKJ6Sr6WiW
@PBlanchardMD Another question is whether prolonging neoadjuvant therapy could increase pCR and offer potential bladder preservation approaches to more patients. Trials are needed to address the implications of EV-P in such approaches.
Bladder preservation would justify the cost/tox.
@MikeSerzanMD@TiansterZhang I am surprised by the fact that the control arm didn't have the option of a docetaxel triplet as in PEACE-1. Not sure how many of us would treat BRCA mHSPC (especially high V) with abi alone. Not me...
Also for OS analysis, do we have the % of subsequent PARPi use in control arm?
Transdermal estrogen vs ADT seem equivalent in efficacy for hormone sensitive prostate cancer. Different tox profile (lower hot flashes, no bone tox, but higher gynecomastia).
@tompowles1 presents positive data for Niagara in muscle invasive bladder cancer. Of course, access to IO in the control arm upon progression would be interesting to see...
Similarly, is this superior to adjuvant only?
@Tony_Calles reminds us that the FDA will be strict about trial design to ascertain the value of each part (no vs adjuvant) of therapy in NSCLC moving forward. #ESMO2024
Post surgical ctDNA clearance is associated with improved EFS in localized NSCLC in AEGEAN, as presented by Martin Reck @myESMO#ESMO2024
Will ctDNA make its way into routine care?