SOHO trial in NEJM:
🏙️ Multicenter RCT comparing high-flow nasal cannula vs. low-flow oxygen among patients with acute hypoxemic respiratory failure (mostly pneumonia)
🏙️ Inclusion criteria required a respiratory rate >25 and substantial hypoxemia (P/F <200)
🏙️ No difference in the primary endpoint of mortality (not surprising, the mortality endpoint is nearly always neutral in modern RCTs evaluating the nuances of supportive care).
🏙️ HFNC reduced the rate of intubation and increased the number of ventilator-free days.
🏙️ No significant signals of harm from HFNC.
This is similar to the FLORALI trial (by the same group of investigators). However, FLORALI showed *improvement* in mortality, whereas the current study didn't.
Why do these studies disagree about mortality?
The FLORALI trial found no mortality difference between HFNC versus conventional oxygen among ALL PATIENTS. However, it DID find a mortality difference in the *subgroup* of patients with P/F <200.
So this is a classic tale in critical care - a subgroup analysis from one trial subsequently fails to replicate. (At least, in terms of the mortality benefit.)
But chasing mortality in these trials is a fool's errand. Overall, the SOHO trial still supports the use of HFNC in acute hypoxemic respiratory failure (in terms of reduced intubation and improved ventilator-free days).
Using HFNC for sick pneumonia patients is already standard care, so I don't see this changing practice very much. Keep calm and HFNC on. 🌬️
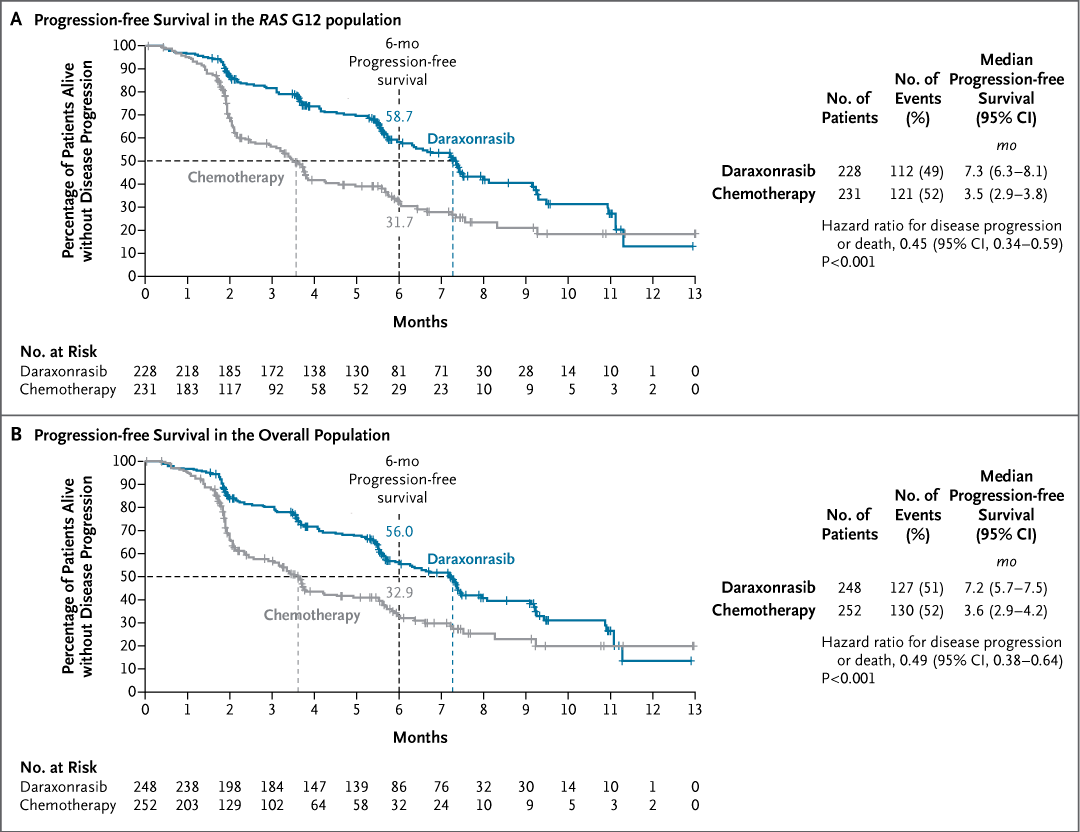
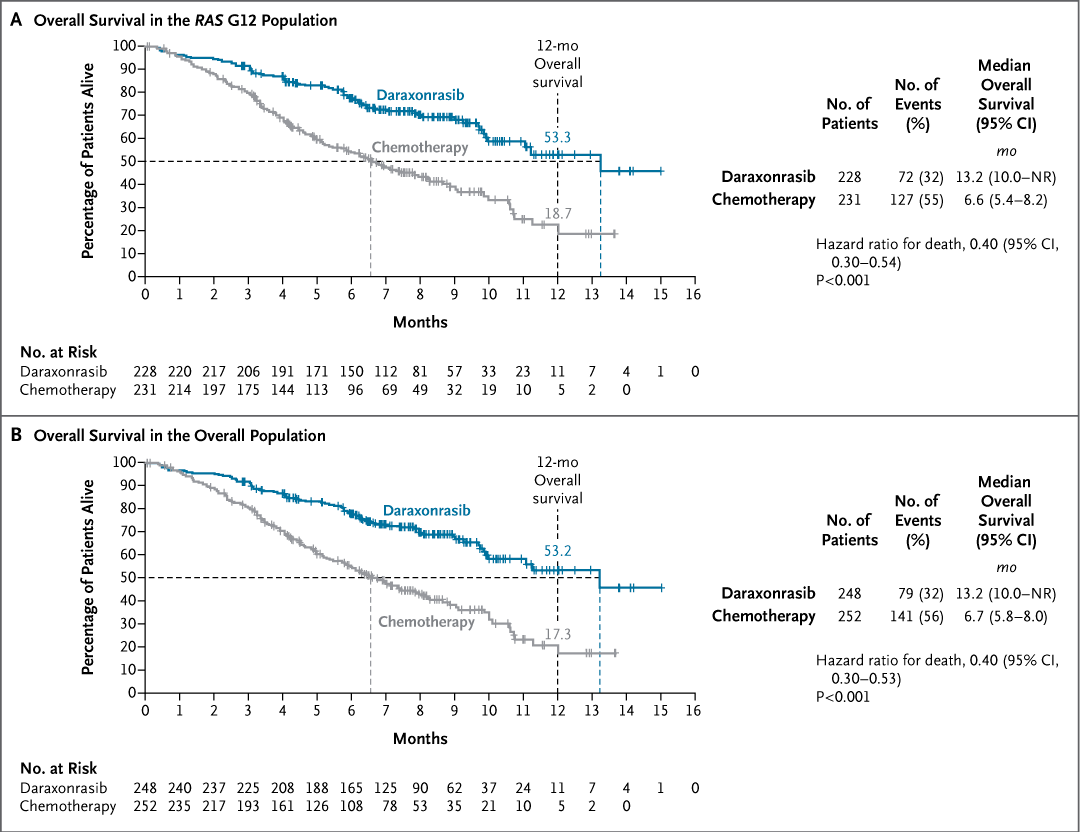
Original Article: Daraxonrasib or Chemotherapy in Previously Treated Metastatic Pancreatic Cancer (phase 3 RASolute 302 trial) https://t.co/y4G27hfORg
#ASCO26 | @ASCO
NEJM: New research reveals a massive concentration in medical malpractice: just 1% of all physicians account for 32% of all paid claims🩺⚖️
It seems risk isn't random—it's highly concentrated among a small group of practitioners.
Full study: https://t.co/4tcx4F5VWF @EricTopol
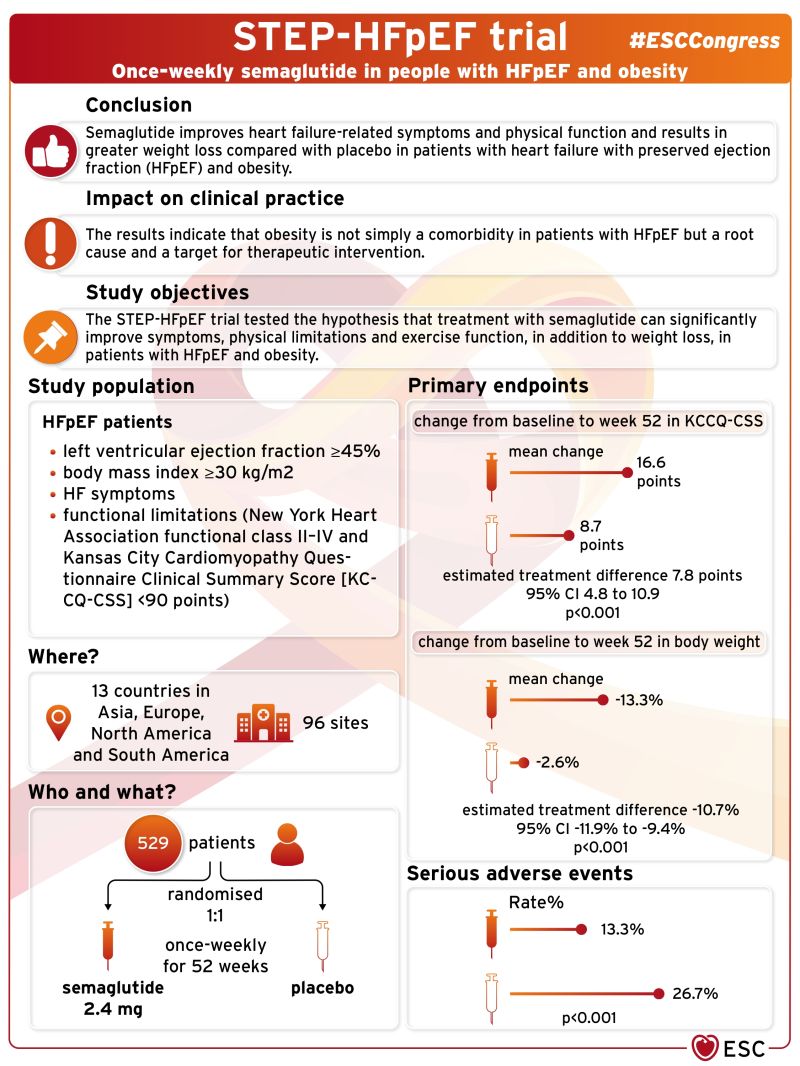
#Semaglutide improves heart failure-related symptoms and physical function and results in greater weight loss compared with placebo in patients with #HFpEF and #obesity#STEP-HFpEF trial
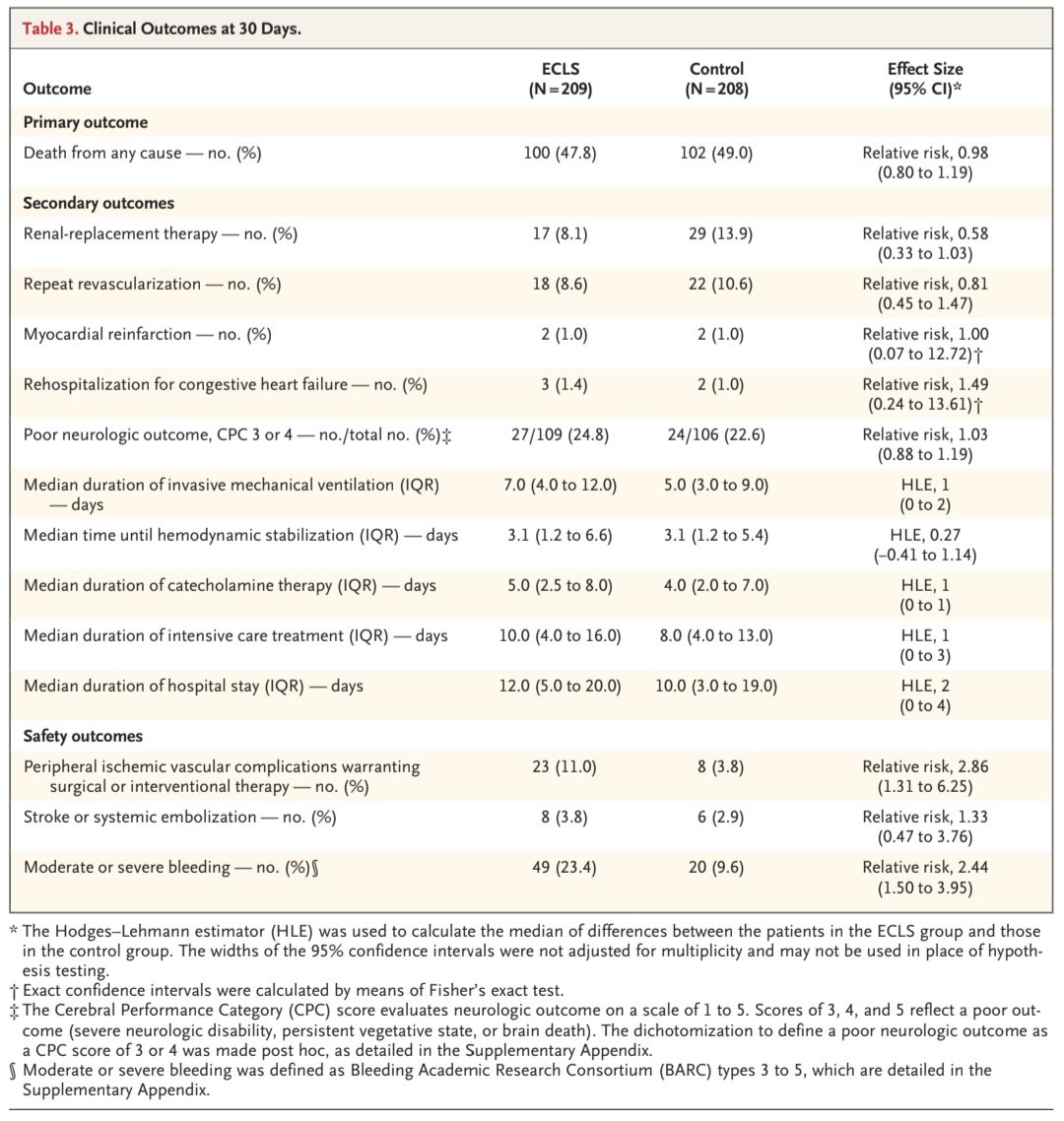
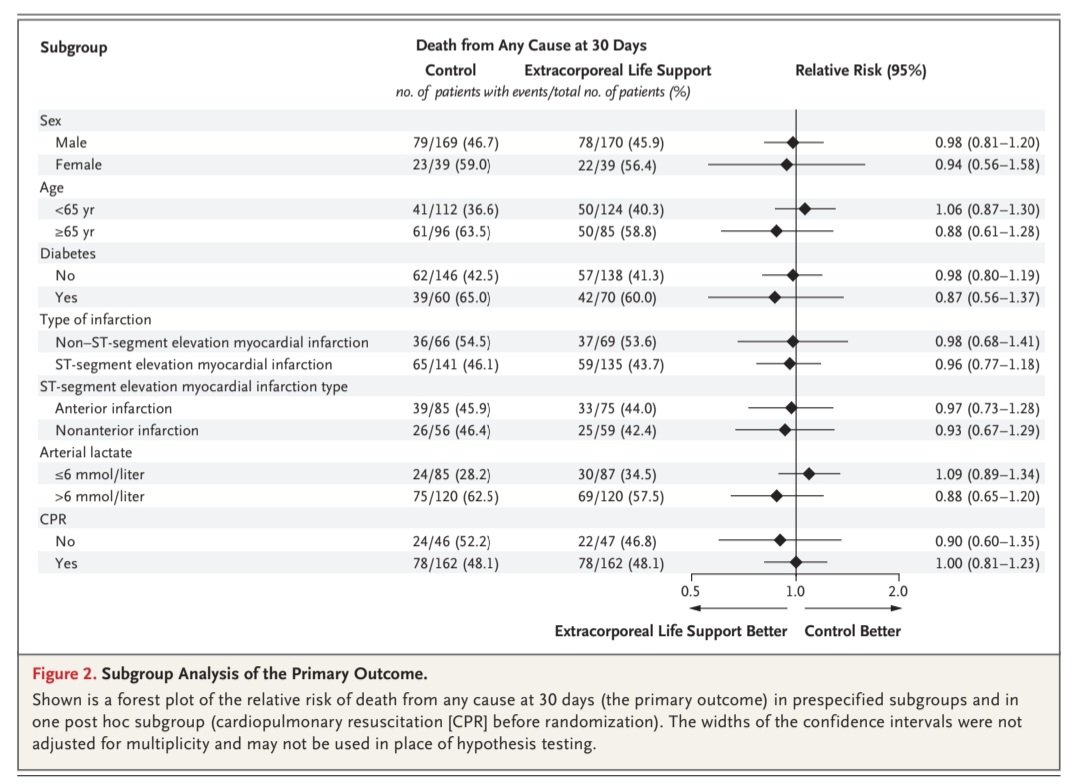
Soporte vital extracorporeo en choque🫀 por IAM.💥
✨️ECLS-SHOCK trial📈 @NEJM
🟢209👥️Tto médico+ECLS 🆚️ 209👥️Tto médico
⛔️Sin diferencias en outcome1️⃣:☠️🫀RR 0.98
🚫ECLS se asoció con más complicaciones, ⤴️hemorragias (RR 2.44) y eventos vasculares periféricos (RR: 2.86).
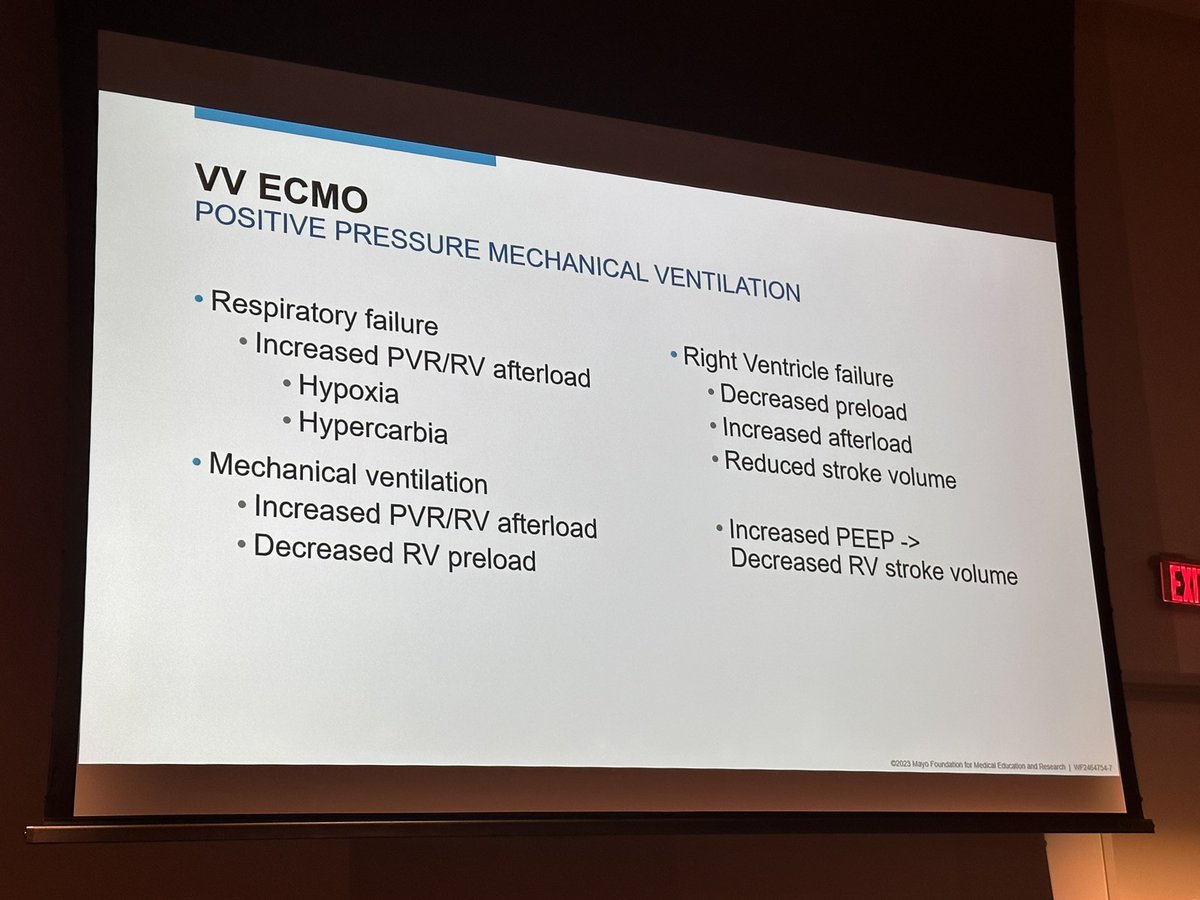
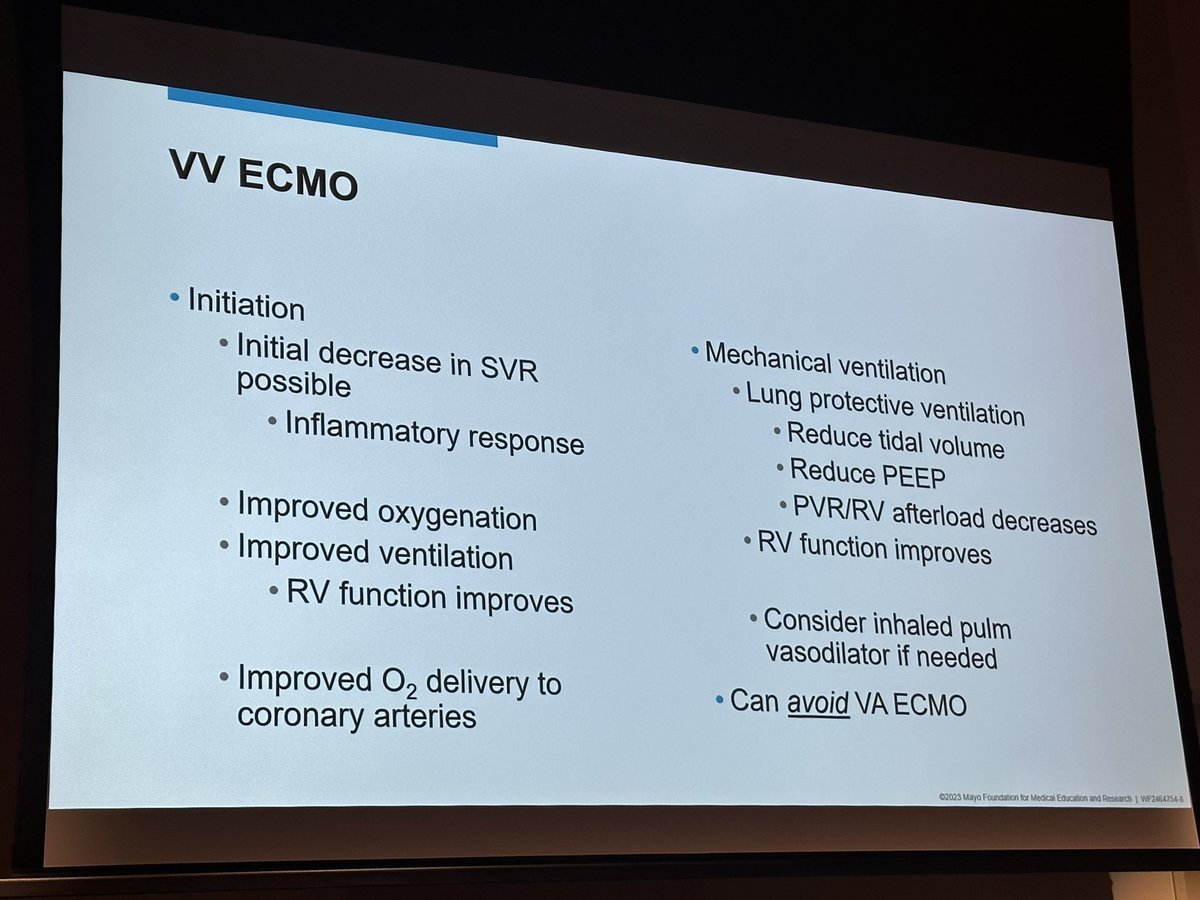
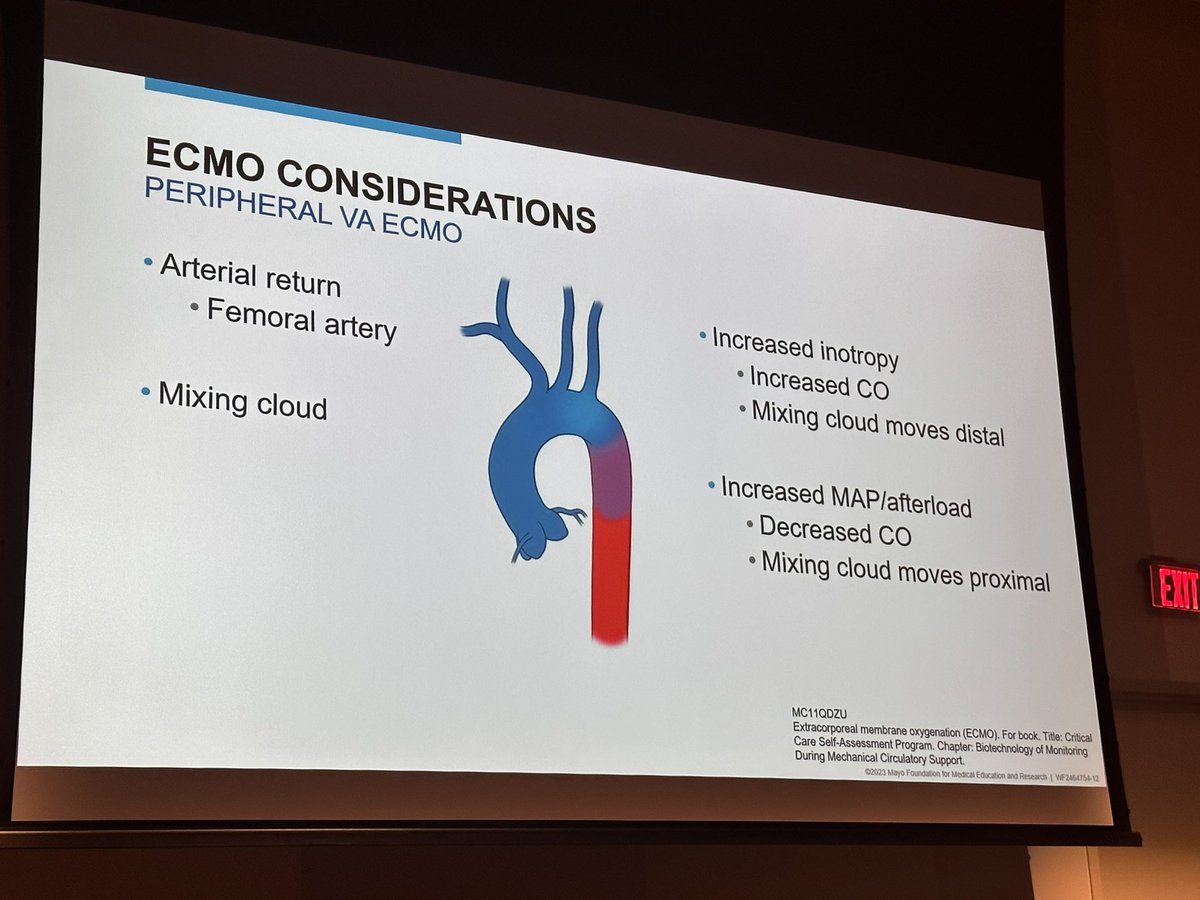
Try to avoid converting to #VA-ECMO from #VV-ECMO for primary respiratory failure with appropriate lung protective ventilation and respecting RV function
@MayoPCCM@MayoAnesthesia@EricaWittwer
✅️Rosuvastatina 20 mg es el más📈potente y con misma eficacia que estatina intensidad moderada + ezetimibe.
🚫Requiere ajuste renal y puede causar ⬆️LRA a dosis altas por tiempos prolongados⏩️ STICS trial.
✅️Atorvas y fluvastatina no requieren ajuste renal.
@OOllarvide 👌
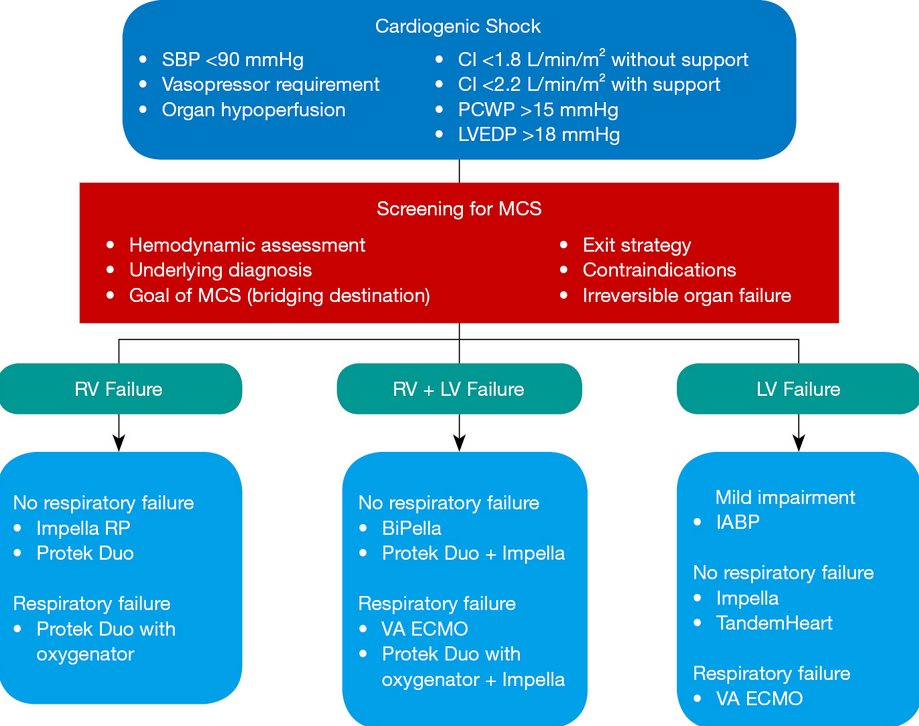
Today's paper of the day is by Alfred Wong on short-term mechanical circulatory support (IABP, Impella, ECMO, TandemHeart)
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2023