Electrophysiologist specializing in complex ablations with special interest in atrial fibrillation as well implantation of all devices (pacemakers,ICDs,CRT)
@YGandye@Salome59131093 Great work! So proud of your progress! You are proving that the Madaktari mission of training rather than just doing is really working!! I am very proud to be part of your team
@YGandye@Salome59131093 Incredible week of cases as Madaktari Africa team of David Singh and Dr Nitish Badwar did an amazing group of cases including the first cases of Conduction system pacing in sub Saharan Africa, multiple complex PVC and WPW cases,pacers ICDs. @YGandye@drdavidsingh , @madaktari
Ep cases @Jakaya kikwete cardiac insititute. Given the complexity of the Ep field and manpower scarce, in aggregate, we target at least 50% (50% assistence) of cases done annually by local team starting on July 2025. Alot of support needed in similar manner Madactari Africa does
Persistent Atrial Fibrillation With Successful #Convergent Ablation
@Drmattsackett and colleagues present a case of persistent #AFib and the successful restoration of sinus rhythm with convergent ablation. Read the case study from our April issue here: https://t.co/A66OiWIwek
Working together with madactari africa to treat clients at Jakaya kikwete cardiac institute (JKCI) . 6 patients had heart rhythm disorder cured 100%. 2 clients implanted high power device, 6 received pacemaker implant and 2 replaced new devices. What a successs!
@purerfellner Nicely done study. Can you share any more detail about what additional areas were ablate in the substrate modification group? Percentage of posterior wall vs anterior wall etc?
@EduFrancoDiez@pjsm83@Arritmias_HRC@cris_lozano What defines type II vs type I biatrial flutter? If I do an anterior mitral line because of anterior scar I always ensure that Bachman bundle connections are eliminated so as to pre this development. But requires much more extensive anterior ablation
@PrashSanders@ALFIEEP1@peterkistler3@drluissaenz Was there a restudy to see if PWI was durable? Did it fail to improve bc of recurrent PW conduction which is not uncommon even with exit block w high output pacing?
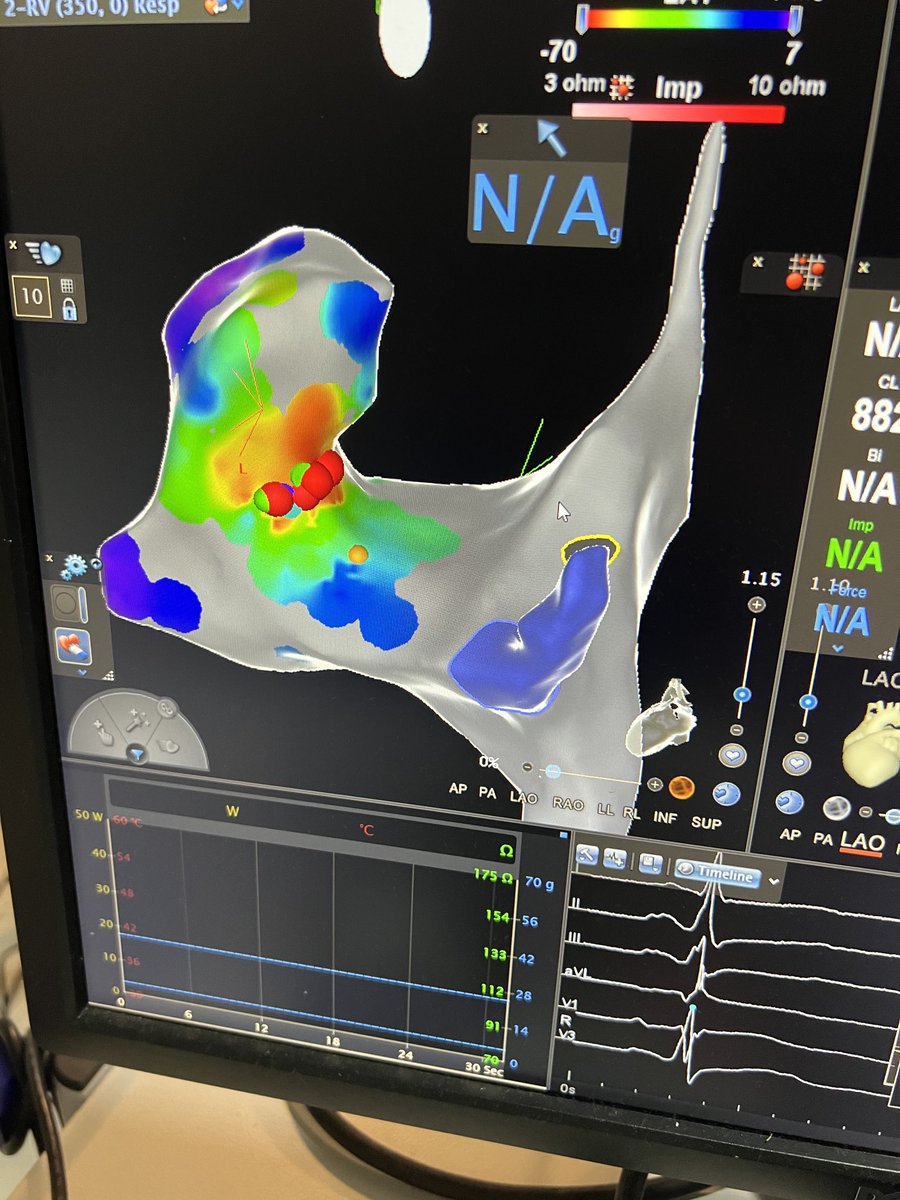
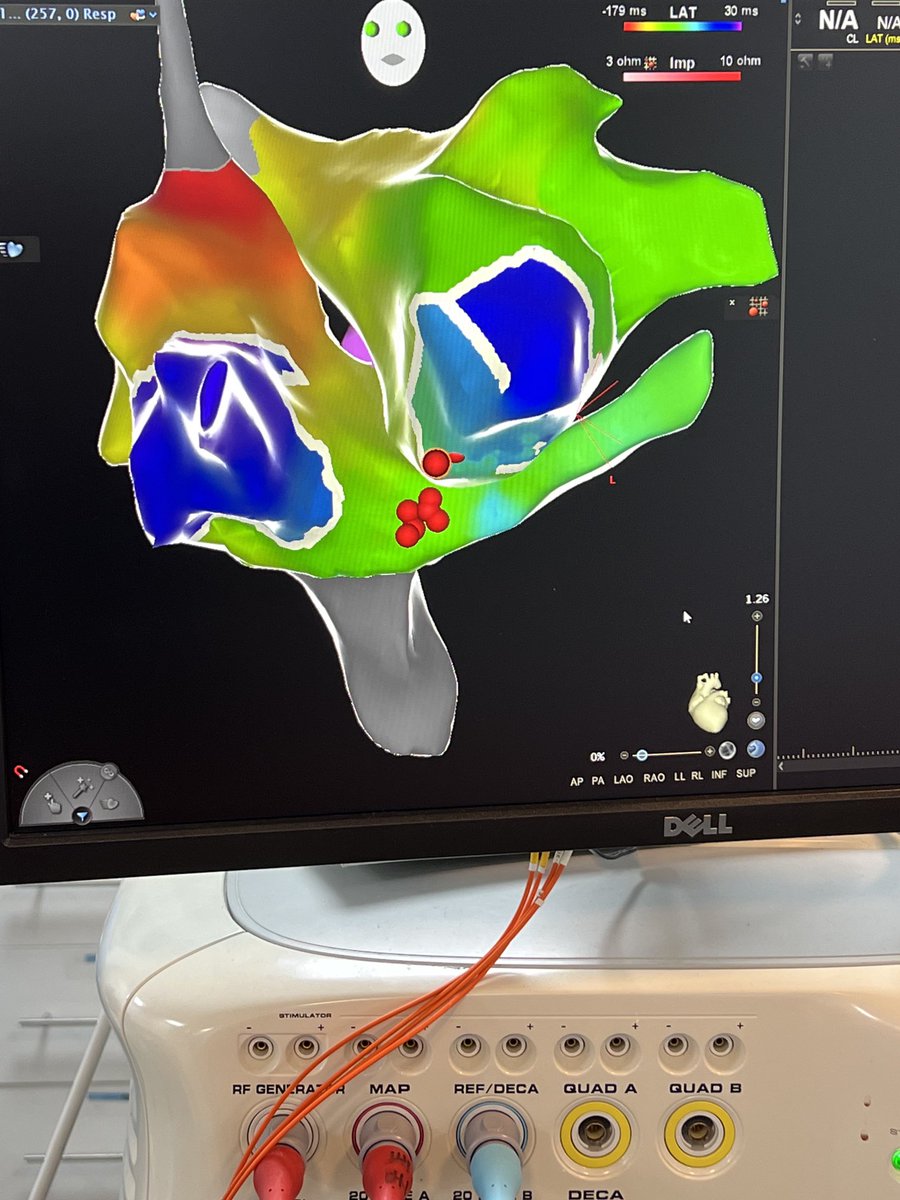
LA flutter around LSPV using ridge and carina gone in 3 seconds. Initial ablation 2005 w 50W, 8mm tip,ostial segmental isolation. Incredible technology upgrades in 17 yrs. Excellent mapping by Cam Bennett #afib,#carto#centrahealth
@GVenkataramanEP Real for sure. But not an indication for a pacemaker. Had recent bc similar case. Sleep study showed severe OSA and “syncope” resolved with CPAP. This finding suggests OSA but doesn’t necessarily correlate with conduction system disease or need for pacing
We returned to the to JKCI in Tanzania this month! Pictured here are the Madaktari & JKCI team members from the trip. Thank you everyone that contributed their time, talent, and treasure towards our return to Tanzania after an almost two-year hiatus due to the pandemic!
@pjsm83 @MiguelVldrbno @PhilippKrisai@FYang_EP @BrettGidney @FrischMd@bisbal_EP@MoisesManero Similar case recently. Injected directly the sheath without a balloon. Just ensured as good occlusion as I could obtain with the sheath. Worked perfectly. Isthmus blocked
@mcfinlay@ALFIEEP1 Agree that I like ability to control rate to improve catheter stability. Similar to controlling respirate and TV. Better stability equals better lesions. And still utility in testing for AT/afl. Am I the only one still looking beyond PVI on first ablation?