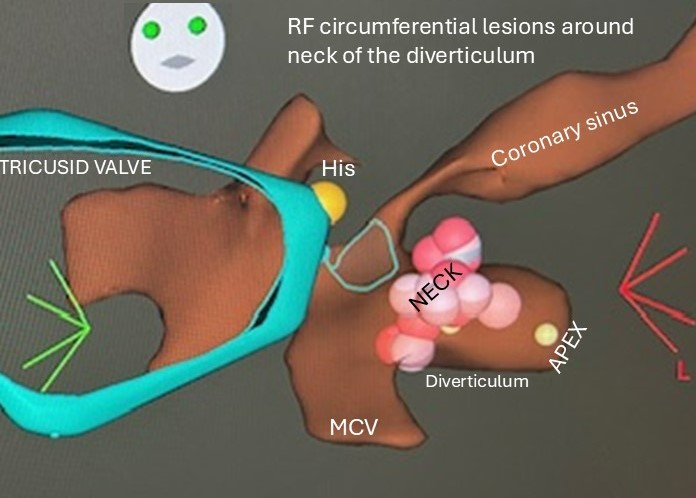
#EPeeps - tough case👇
⚡️VF triggering pathway from CS diverticulum. Neck >5mm from PLV.
🥉Took 3 goes to get rid of it. Bumped each time - gave limited RF - back in 24hr.
🔥 Encircled neck (30W-20sec) with irrigated RF and its FINALLY gone! @LiverpoolEP#Alwayslearning
#EPeeps - epi RF ablation in transverse sinus to terminate peri-mitral flutter and block anterior mitral & LA roof lines @LiverpoolEP
Epi access with CO2 insufflation post CS exit @JohnSilberbauer 🙏
Excited for EPIC-AF @AbbottCardio - redo PVI vs redo PVI + Endo/epi lines 🤔
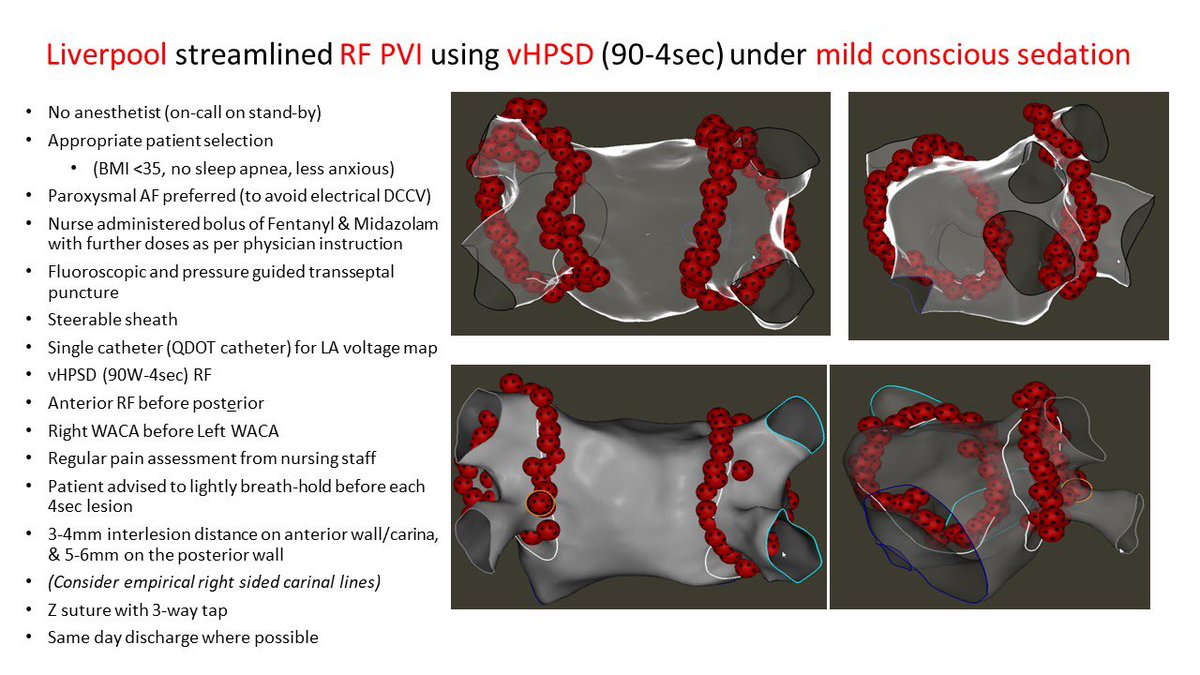
We found similar impedance drops + contact force as 50W/10-15sec lesions under GA, inferring that catheter stability may be similar under sedation with RF restricted to 4secs.
With 👍 12-month freedom from AF recurrence, a nice alternative where anaesthetic support is limited.
#EPeeps – is GA/deep sedation available for every AFib ablation in your centre? 🤔
…No❓
We discuss our “@LiverpoolEP Streamlined Approach” to RF PVI under mild conscious sedation using 90W/4sec #QDot @BiosenseWebster
Now online open access @JCardioEP
https://t.co/WOIzBHJyXT
📢When imaging meets #EPeeps
"RVOT ablation close to an anomalous right coronary."
Read👇 @HRS_CaseReports how we @LiverpoolEP used #CARTOSEG + #CARTOSOUND @BiosenseWebster to visualise the anomalous RCA, just 1mm from the posterior RVOT
👏Dr Pete Calvert
https://t.co/3YAC9iVY8Z
#EPeeps#ablateVT
Do you set your bipolar voltage LV substrate maps to 0.5-1.5mV?
We @LiverpoolEP describe an alternative approach using CARTO Ripple Map to differentiate scar (=no ripple bars/red) from borderzone @BiosenseWebster
Open access @JCardioEP
https://t.co/8vigO5HfSS
#EPeeps
Delighted to share #EHRA2022 abstract
"Using Ripple Mapping + PentaRay @BiosenseWebster to differentiate post-infarct scar from borderzone on a bipolar voltage map during VT ablation" #NoMore050to150mV
Congrats to @DibbendhuK & team @LiverpoolEP
https://t.co/ptXGyMps6D
#EPeeps Excited to learn more of @AbbottCardio#EnsiteX ingenious Omnipolar vectors timing independent activation mapping. My first use in this CTI gap @LiverpoolEP.
I wonder how the vector is assigned when a large far-field EGM is seen in low voltage scar 🧐. @aportasanchez
#EPeeps
-Watch Vid 4 (2mins) - Ripple Map in stable VT.
-Bars in diastole reveal the conduction channel. Adjusting the voltage display defines its anatomical location in relation to scar <0.15mV
-RF-1 term⚡️
👏@gkatritsis & team
Free download ends today
https://t.co/7Cj9ElPW6i
#EPeeps - what do you recommend?
40M, CHA2DS2VASC=0, paroxysmal AFib (symptoms x1 per week, last few hours), plan for first time PVI under conscious sedation. Normal LA size.
(Note: ESC AF GL 2020 “>3 weeks NOAC in pt WITH stroke RF”. No recommendations for those without RF)
Our Ablation Index guided 50W #AF ablation paper published in @ESC_Journals
Excellent 12-month results, safety (zero steam pop)
Much shorter Abl and procedure times than AI-guided 35-40W
https://t.co/KZsZvxFgYH
@jongichun @BorisSchmidt5 @LHCHFT#EPeeps
1/3
#EPeeps
In case you’ve not seen this Carto feature yet - to compare timings of any mapped points, highlight the points as “ripple marking” (coloured bars👇) & 👀 the EGMs in the “ripple viewer”
Was useful in this VE abl (comparing timings from RVOT, LVOT & GCV)
@BiosenseWebster