🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
I review the statistics in ~200 manuscripts a year for some of the top urology journals in the world.
Here's what I actually do — and the mistakes I see in almost every paper. 🧵
What an emotional day. Last prostate clinic and one stop for @prokarurol before his retirement. Friend, mentor, colleague. 28 yrs service. Innovator, technology enthusiast and true legend of urology. We will all miss him.
An excellent long weekend at EAU @Uroweb
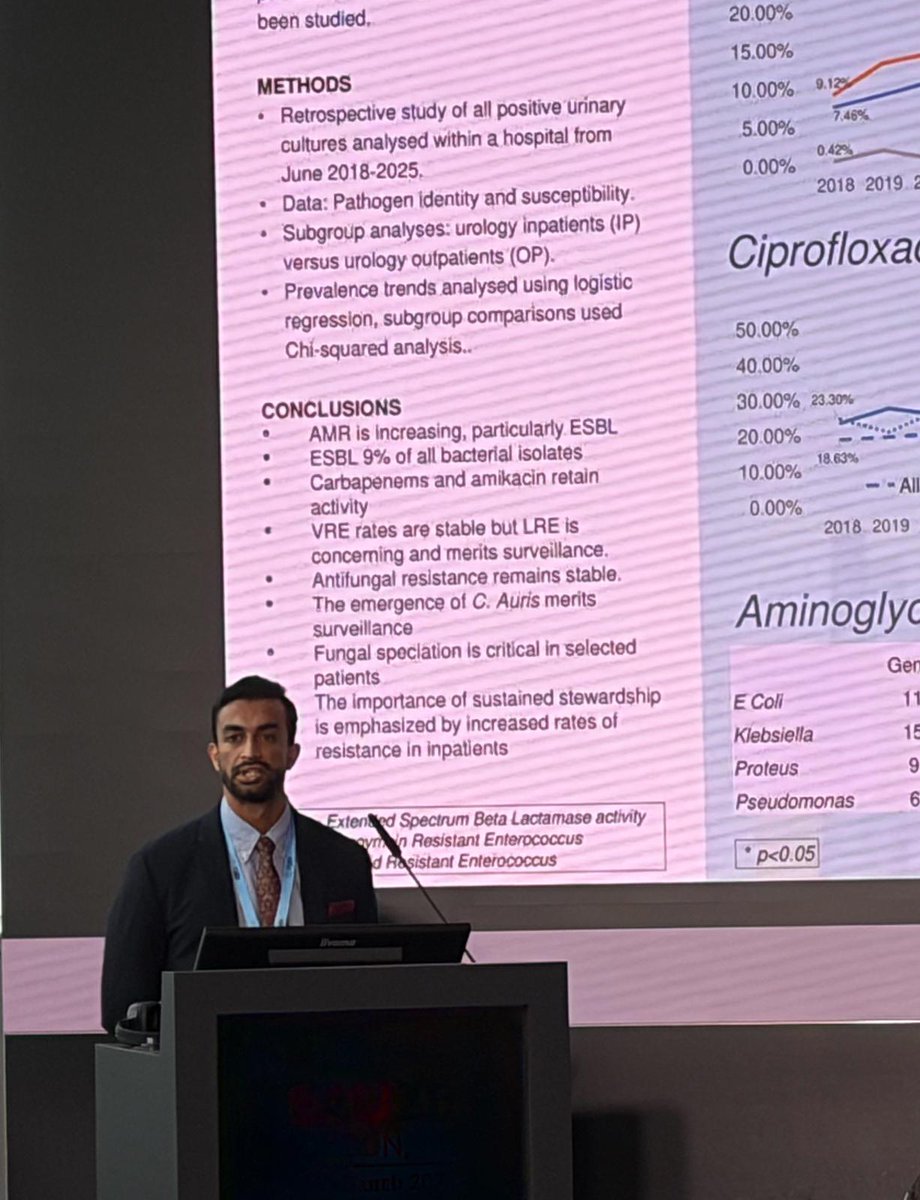
Grateful for opportunity to present The UROME Study
📈ESBL rising year on year
⚠️ESBL in 9% of all bacterial isolates
⏩️VRE remained stable
☣️Emergence of C. Auris
🧫Fungal speciation important
@GuysUrology
Live operating from @GuysUrology at EAU @Uroweb
FANS RIRS with @thomastailly
-2300m3 1100HU stone, 11/13Fr FANS with 7.5Fr scope, Magneto laser, fluid 120cm above patient, suction at -60
@dasgupta telesurgery RARP London > Gibraltar
It has been a pleasure showing around the selected Japanese Urology Association residents @suzuken3001@hirokit__ and Takashi Okamura for their exchange with EAU @Uroweb. The tour included @GuysUrology observing ureterolysis and nephrectomy.
What an honour to deliver my presidential address at the start of my year as @RoySocMed Urology Section President on Friday. Thanks to all those who came and have supported me 🙏
Looking forward to a great academic programme this year.
The UK 🇬🇧 PUrE RCT1 LOWER POLE STUDY for the stone <10mm now published…
https://t.co/yxf4vlA1jM
This link will give FREE ACCESS to the article for 50 days…
This is just the beginning - such a vision requires collective effort. If you're driven by tackling foundational questions about our long-term future and want to contribute, we'd love to connect. To learn more - https://t.co/DbaVq3WZiH