@benhibbertMDPhD@anish_koka@GreggWStone Yes! Id argue that the direct financial and industry COI is only a slice of picture. It is human nature for researchers and clinical trialists to want their work to be meaningful and transformative. Letting them decide if their work gets that nod in the guidelines is COI
Conflict of Interest with Industry was handled very differently 2018 vs. 2026.
The 2018 guideline preamble explicitly states that all writing committee members were required to be free of recent and relevant industry-related conflicts.
The 2026 guideline states that writing committee members are required to recuse themselves from voting on sections to which their specific relationships with industry apply.
So the ACC/AHA shifted from a blanket "no relevant conflicts allowed on the committee" policy (2018) to a recusal-based model (2026) where conflicted members can serve but must recuse from relevant votes.
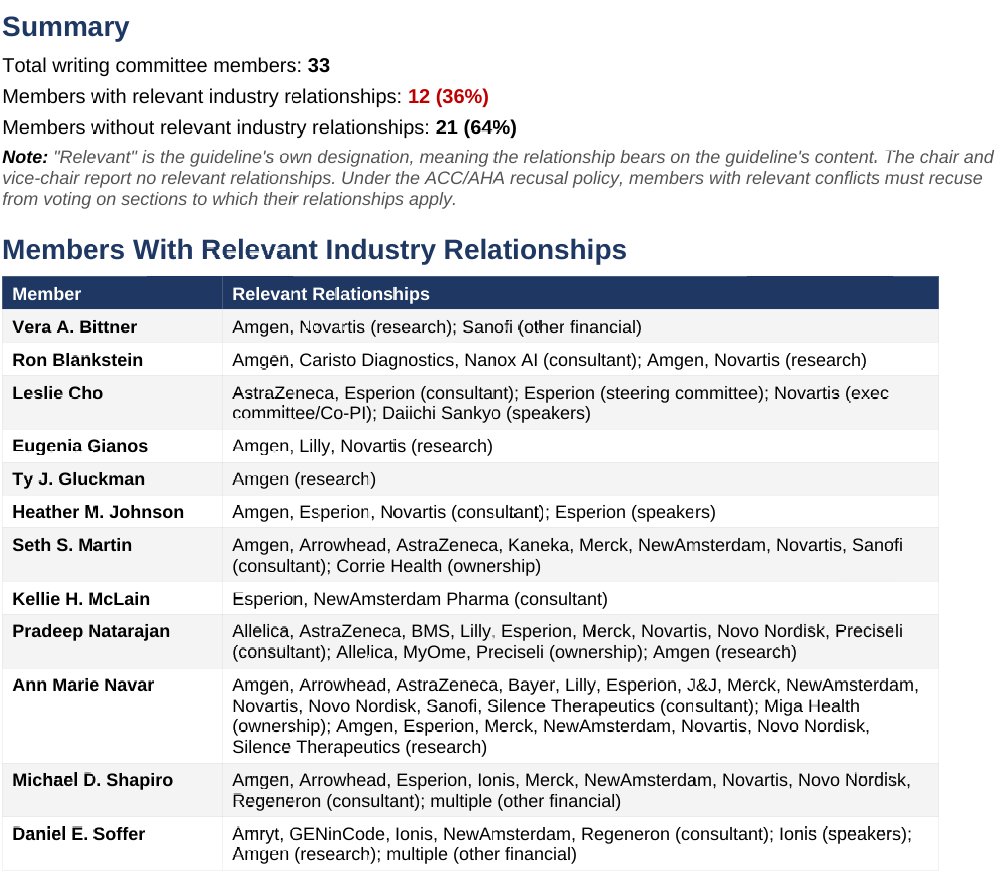
Take a look yourself.. of the 33 total members, 12 disclose relevant industry relationships. The column showing how many committee members have relevant ties to each company makes the concentration of relationships around PCSK9 inhibitors, Lp(a)-lowering agents, genetic risk profiling, and the new pipeline drugs pretty hard to miss.
The guideline states that members are required to recuse from voting on sections to which their relationships apply, but the actual recusal record — who recused from which votes —I can't find publicly.
So we know who has relevant conflicts and with which companies, but we don't know whether those individuals actually recused from the specific recommendation votes where their conflicts were most direct — for example, whether Blankstein recused from CAC scoring recommendations, whether Natarajan recused from the genetic testing/PRS sections, or whether members with Amgen/Novartis/Esperion ties recused from the PCSK9 inhibitor, bempedoic acid, or inclisiran recommendations.
But even if assume everyone recused themselves from voting, did they also recuse themselves from the discussion before the vote happened?
It's an important question because the most troubling, recommendations happen to relate to Coronary calcium testing, genetic testing, routine Lp(a) testing, and expanding pcsk9inhibitors to ever broader populations... which just happens to be where the concentration of COI lives.
Happy to hear from anyone with more knowledge of how the sausage was made. DMs open!
@drjohnm This is one of the few tests that, on a population level, nearly guarantees more procedures, more intervention in stable disease, with no mortality benefit. Doctors, hospitals and health systems are financially incentivized to make that a certainty. PSA comes to mind as parallel
@drjohnm Strongly considering dropping all societal memberships based on this guideline. Too much bias. Guidelines have just become a clever game to put more $$$ into their members/advertisers pockets. Not about science and hardly even veiled at this point.
@drpablocorral@rblument1 No disrespect to the main authors or their body of research but it’s a major introduction of bias when the all of the main authors are citing their own career defining research to make recommendations. Guidelines need to move toward independent EBP panels to gain better cred
@type1typea@drjohnm Lack of calcified plaque does not exclude non-calcified plaque. If risk is high (think older, uncontrolled diabetic, obese, active smoker), and calcium score is low or zero, risk remains high. Noncalcified plaque causes heart attacks and strokes, not calcified (typically)
@MichaelRyanRuiz IU scoring looks pretty good. Much better than when they played Ohio State and scored 13 points a few weeks ago. Cant remember how many points Miami scored against Ohio State but it couldn’t be as much as this elite IU team did, and so this title game is a foregone conclusion
@CMichaelGibson Need to move toward paying for the value of the service provided (to the patient and the system) and not just the volume or how complex the service is to do. If primary care delivers exceptional prevention and outcomes they should be paid better. If they don’t, paid less well.
@MKIttlesonMD Perfect as long as you consider CC as part of the HPI. The CC tells the audience the framework of how to think about the details in the HPI. Too often trainees list 10 medical conditions before mentioning that the patient came in for chest pain. Start with chief complaint
@AlfredoERodrig2@GreggWStone This trial proved that it does have a placebo effect, as the incremental improvement in anginal symptoms are significantly less than that reported in non-sham controlled trials. It also proved that it has an actual/real effect as well. Both are apparently true