Presented at #ASCO26:
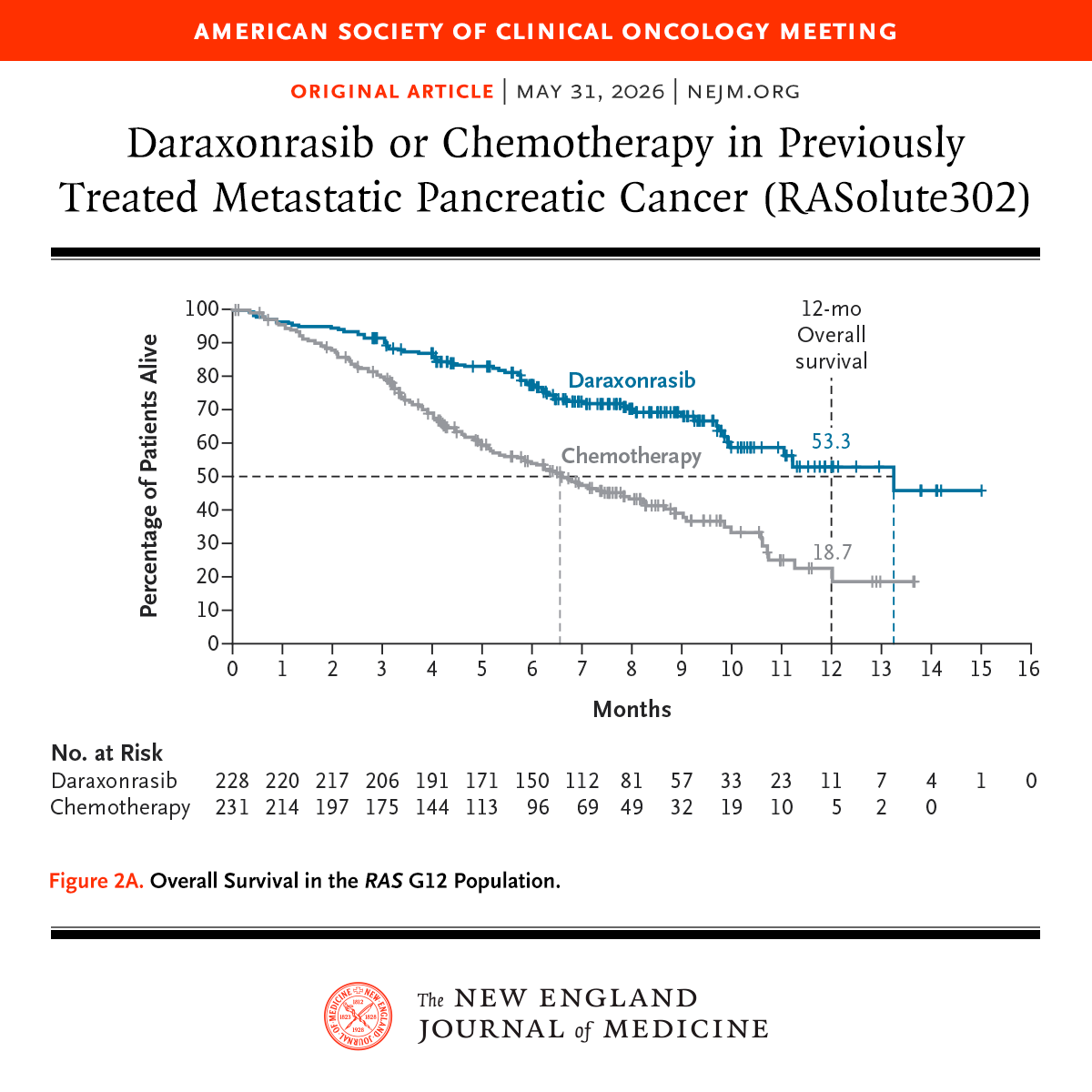
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
Brian Wolpin, MD, MPH, presents positive results from the RASolute 302 trial showing a substantial prolongation of survival for patients with previously treated metastatic pancreatic cancer, regardless of RAS mutation status, taking daraxonrasib, an investigational oral RAS(ON) multi-selective inhibitor, compared with chemotherapy. #ASCO26
1/8
— The First Lesson as a Surgeon, Inherited from Dr. Yamamoto —
🎯 Let’s start with a question.
There’s a small circle drawn on a piece of paper in front of you.
“Put a dot inside this circle.”
How do you do it?
A: Slowly and carefully, making sure it never goes outside.
B: Quickly — just a quick flick, focusing on speed.
Which is the “right” answer?
Dr. Michael DeBakey and his protege Dr. Denton Cooley once formed the world’s most elite heart surgery team at Baylor.
On April 4, 1969, Cooley implanted the first Total Artificial Heart (TAH) without DeBakey’s permission.
DeBakey claimed Cooley "stole" the device from his research lab while DeBakey was out of town.
Cooley argued it was a desperate "bridge to transplant" to save a dying patient; DeBakey called it a "childish" bid for glory.
The move triggered a federal investigation and an immediate, irreparable split in their professional relationship.
Cooley left Baylor to build the Texas Heart Institute (THI), creating two rival surgical empires on the same Houston block.
Despite working doors away from each other, the two legends didn't speak for nearly four decades.
In 2007, a 99-year-old DeBakey and an 87-year-old Cooley finally shook hands and reconciled just before DeBakey’s death.
In @BJSurgery Commission on SI-NETs:❓what to do with peritoneal disease?
Complex & often missed
From the experts:
✅ Use PCI
✅ CRS if can achieve >90% debulking
❌ HIPEC not recommended
⚠️ PRRT risk in high peritoneal burden
All here https://t.co/4eWzoIIMEG
@spartelli
Resect primary SI-NET if liver mets aren't resectable?
@BJSurgery Commission: most often, yes
🔑 Patients cope with symptoms: "asymptomatic" is rarely real
🔑 Long survival = long window for complications
🔑 Resection ⬇️unplanned admissions/surgeries
📝https://t.co/6zAzuKpOUJ
In clinic with SI-NET: is liver resectable? operate on the primary? touch the liver? how?
🌍experts came together in @BJSurgery commission to tackle the hardest SI-NETs surgical questions👉🏻https://t.co/6zAzuKph5b
Will be breaking it down this week - keep 👀 out!
@spartelli
During Easter 1982 the bacteria that causes most stomach ulcers and can lead to gastric cancer was first discovered.
Robin Warren (left) and Barry Marshall (right) tried and failed to grow the organism several times. It was only when the agar plates were left in the incubator over the five-day Easter holiday that numerous colonies of the bacterium developed. It became clear that a new bacterial genus had been isolated, which was eventually named Helicobacter pylori.
In 2005, Marshall and Warren were awarded the Nobel Prize in Physiology or Medicine for their discovery: https://t.co/8s8TWpF1jh
HIPEC finally shows a signal in T4 colon cancer.
But not where you expect.
It reduces peritoneal relapse…
Yet DFS and OS don’t improve.
Here’s HIPECT4 final analysis 👇
🧪 Trial
Resectable cT4N0-2M0 colon cancer
n = 184 randomized
⚔️ Arms
🔹 Surgery + adjuvant chemo
🔹 Surgery + HIPEC (mitomycin C 30 mg/m², 60 min) + adjuvant chemo 
📊 Primary endpoint
36-month locoregional control
🔥 Key result
HIPEC improved peritoneal control:
HR 0.19 (95% CI 0.04-0.86), P=0.031 
❗ But the reality check
No significant difference in:
• DFS
• OS 
🎯 Where benefit was strongest
• Definitive pT4: HR 0.08, P=0.017
• Per-protocol (received chemo): HR 0.18, P=0.028 
🧠 What changed biologically?
Less peritoneal relapse
More systemic pattern of recurrence
No added toxicity 
💡 Takeaway
This is NOT a survival-changing trial.
But it is a pattern-changing trial.
👉 HIPEC may matter in selected high-risk T4 patients
👉 Not ready for universal adoption
🔖 Save this before your next tumor board
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #ColorectalCancer #SurgicalOncology @OncoAlert@myesmo@esmo_open@asco@BJSurgery
The first rule of medicine is: first, do no harm!
In oncology, that does not mean feeling obliged to do something for every patient; it means knowing when to avoid unnecessary treatment. Not every chemotherapy regimen, every combination, or every later-line treatment provides real benefit. Sometimes the right decision is not to add more treatment, but to stop the toxicity. Knowing what to give matters; knowing what not to give matters even more.
#oncology #cancer
High Variation in Expert Assessment of Peritoneal Malignancy
by Bhatt A, Sharma V (...) Glehen O et 42 al. in Ann Surg Oncol
🪡 read our summary 👉 https://t.co/gwkSm12Usn
📖 read the article: https://t.co/TXZzJkEXMw
Join us tomorrow, March 26th at 7pm for a webinar led by Dr. Lambert & team at @nyulangone reviewing @NCCN Guidelines for #appendicealcancer, as well as the current Peritoneal Surface Malignancy Consortium Guidelines for this #rarecancer.
Register: https://t.co/14um1LxMly
The IARC Working Group summarizes guidance on 𝘏. 𝘱𝘺𝘭𝘰𝘳𝘪 screen-and-treat programs for gastric cancer prevention and concludes that prevention is the most effective strategy amid a rising global burden. Learn more: https://t.co/fyqf8Zd0RV