✳️ Imaging the hallmarks of cancer
☢️Imaging techniques reveal the hallmarks of cancer in the precision oncology era
⚠️But decision-making will not change, yet...
📖Grimm J, et. al. Nat Rev Cancer. 2026
🌐DOI: 10.1038/s41568-026-00950-y
When Kaplan–Meier Curves Fool You 📉
A flat survival tail can look exciting…
but sometimes it reflects very few patients remaining under follow-up.
The curve alone is never enough.
Always check: • Number at risk
• Censoring patterns
• Follow-up maturity
• Late-tail denominator
A “long-term survivor plateau” is meaningful only when enough patients are still being observed.
One of the most important lessons in interpreting immunotherapy trials.
#Oncology #MedEd #Biostatistics #Immunotherapy #ClinicalTrials #KaplanMeier #MVOnco
1/n
Daraxonrasib (RMC-6236), the first-in-human oral 💊RAS(ON) multi-selective tri-complex inhibitor, in previously treated RAS-mutated pancreatic cancer phase I/II study is now published in the New England Journal of Medicine @NEJM
A novel💡 way to shut down ⚔️RAS, one of the most important oncogenic drivers in cancer that had long been considered “undruggable.”
🔗https://t.co/ptfNVcxrb4
Shout out to Brian Wolpin, @CentralParkWMD@GarridoLagunaMD@AlexSpiraMDPhD@salmanpunekar@MeredithPelster@bherzbergmd Nilo Azad Aparna Hegde @DavidHongMD and the whole team who dedicated to this study. @EileenMOReilly
#HBP #HumansBeyondPatients
✳️ Agonistas GLP-1: el medicamento del siglo?
Tx: Diabetes y Obesidad
✴️Promueven liberación de insulina mediada x glucosa
✴️Reducen vaciamiento gástrico
✴️Inhiben la secreción de glucagón
✴️Cambios benéficos en microbioma intestinal
✴️Regulan las vías del hambre y la saciedad
KRAS is not a mutation problem, It’s a context problem
KRAS behaves as a dynamic node within a network
KRAS ≈25% of cancers
-NSCLC: ORR ~40%, mPFS >6 mo
-CRC: rapid EGFR-driven rebound
-PDAC: stromal, metabolic, immune resistance
⚠️⚠️Tumors escape through:
EGFR/SHP2 , MAPK/PI3K, YAP/STAT3, plasticity
What this means in practice:
-combinations matter (e.g., KRAS+EGFR in CRC)
-targeting networks works better than targeting a mutation alone 👀
-trials should be built around biological context
https://t.co/WHIk3WuDk1 @OncoAlert@KRASKickers
🚨 Practice-changing in pancreatic cancer?
Daraxonrasib shows a massive OS benefit in phase 3 RASolute 302.
👥 Study population:
Previously treated metastatic PDAC (RAS-mutant & WT)
⚔️ Trial arms:
🟣 Daraxonrasib 300 mg OD
🔵 Investigator’s choice chemotherapy
📊 Key results:
✔️ OS: 13.2 vs 6.7 months
✔️ HR 0.40 (p < 0.0001)
✔️ PFS also significantly improved
🛡️ Safety:
Well tolerated, no new safety signals
💡 Why this matters:
Post-progression options in PDAC have been weak.
A ~2x OS improvement is something we’ve almost never seen here.
⚠️ But:
Topline press release data only
Full breakdown (subgroups, ORR, QoL) awaited at ASCO
🔥 Takeaway:
If confirmed, RAS(ON) inhibition may redefine PDAC beyond KRAS G12C
#OncoTwitter #MedTwitter #GIOnc #PancreaticCancer
@OncoAlert@myesmo@esmo_open
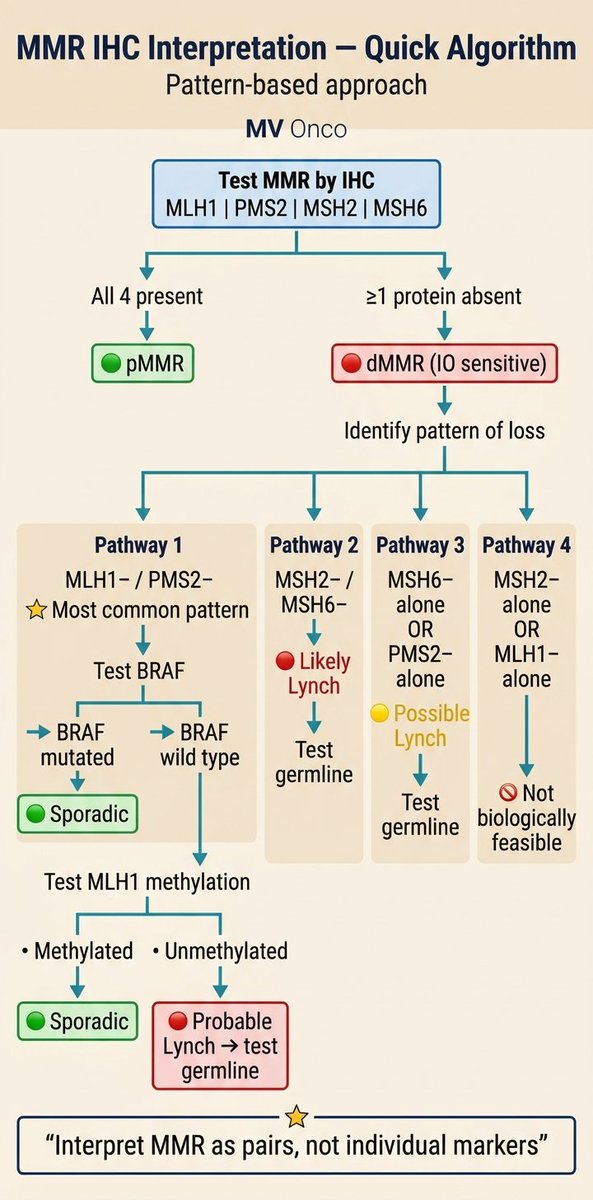
MMR IHC Interpretation – Super Simple Quick Algorithm 🔥
Test the 4 proteins → All present? → pMMR (good)
One or more missing? → dMMR (needs attention)
Then follow the exact pattern of loss:
MLH1 & PMS2 lost (most common) → Check BRAF & MLH1 methylation
MSH2 & MSH6 lost → Likely Lynch
Only MSH6 or only PMS2 lost → Possible Lynch
Weird single losses (MSH2 alone or MLH1 alone) → Not possible, recheck!
Key rule: Always read MMR as pairs, not single markers!
(MLH1 protects PMS2 • MSH2 protects MSH6)
Saves time in daily practice. Save & share!
#MVOnco #Oncology #Pathology #MedEd
MMR IHC — Don’t get the pairs wrong!
Think of MMR proteins as a team of 2:
👉 MSH2 works with MSH6
👉 MLH1 works with PMS2
There’s always a “boss” + “assistant”
🧠 Key rule:
If the boss is lost → assistant cannot survive
But assistant can be lost alone
So if you see:
❌ MSH2 absent but MSH6 present
❌ MLH1 absent but PMS2 present
👉 That pattern is biologically impossible → recheck the report
💡 Easy memory:
“No boss → no assistant”
#Oncology #Pathology #MedEd #MVOnco
To clarify:
✴️Do we need non-inferiority trials?
✴️What is the optimal cutoff point for their evaluation?
✴️Who would actually benefit from them?
✴️Compare the “current” standard ... is time-appropriate?