Been working with @SamAsante on a new company.
Today we’re releasing our first product.
It’s called Typeahead and we’re live on Product Hunt.
You type and inline suggestions appear right in the text field. Tab to accept the full suggestion or right arrow for one word at a time. It learns how you actually write.
Everything runs locally on your Mac, works offline, and you pay once. $79 and you own it forever.
If you write a lot on a Mac, check it out and let us know what you think.
Live on Product Hunt right now → https://t.co/5H9VwvqmcS
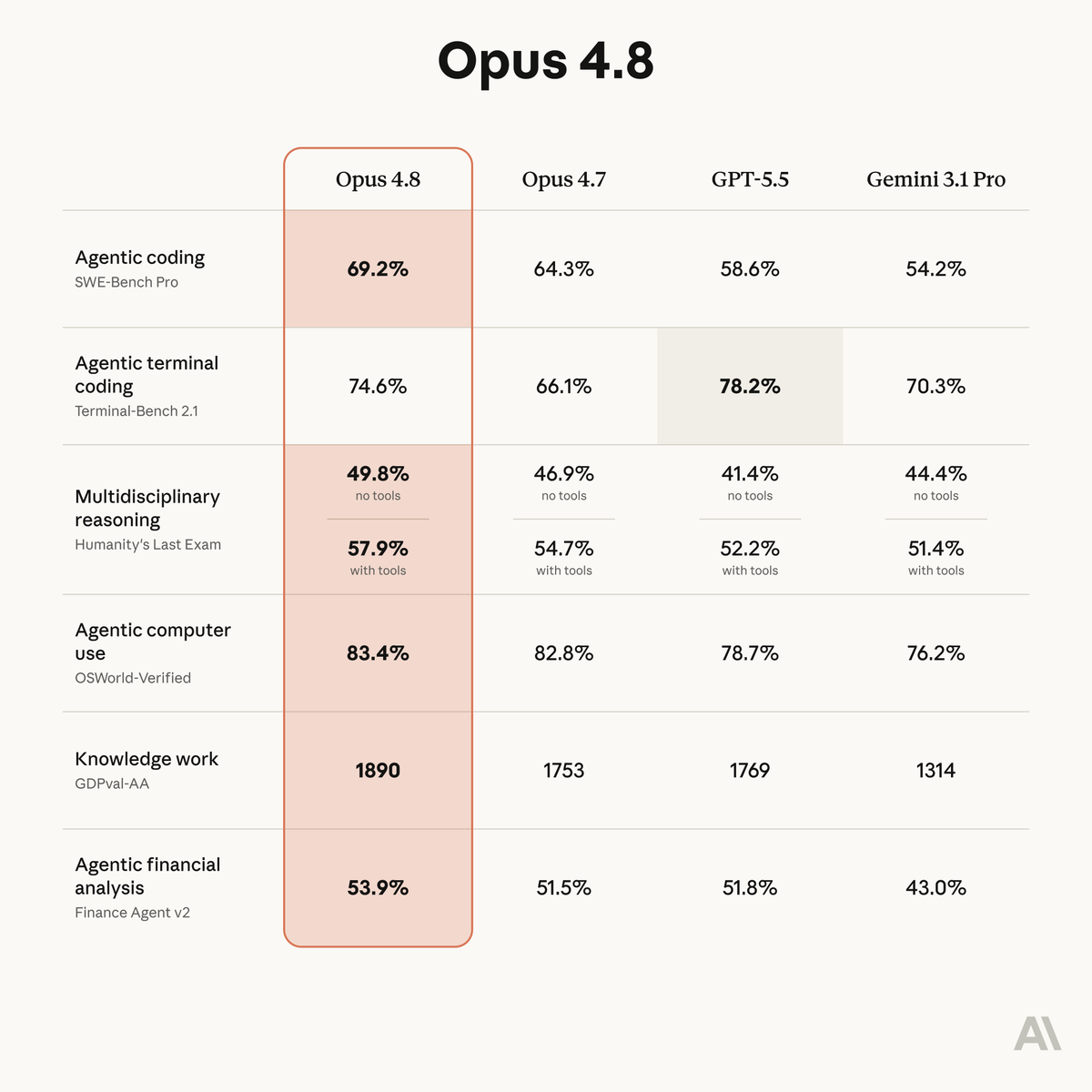
Introducing Claude Opus 4.8: it builds on Opus 4.7 with sharper judgment, more honesty about its own progress, and the ability to work independently for longer than its predecessors.
Available today at the same price.
Data at population scale often falls apart when it meets real world scenarios. Hats off to Bryan and Kate for being at the vanguard and driving huge awareness for what may be possible ahead.
We now have a female Bryan Johnson.
It’s Kate Tolo.
She will become the most measured female in history.
+$2 million of spend per year
+ Developing a female-specific protocol
+ Sharing everything for free
To start, she will spend 3 months mapping her baseline. Men, in contrast, can get their baseline done in 1 or 2 weeks.
+ 3 months for baseline measurement
+ across 4 time points per cycle
+ doing the same thing every day
+ a dedicated full-time medical team
For context on the extensiveness of measurement, during the past 5 years, we’ve collected 1.5 billion data points on my body. I suspect Kate will exceed that given technology has improved since I started.
The goal is to create a repeatable waveform of hundreds of life-critical biomarkers. Once the baseline is acquired, she will begin interventions.
We will try to answer practically useful questions and share all of the data + learnings for free.
Can fertility be improved?
+ Should women cold plunge?
+ Can PMS symptoms be alleviated?
+ What should a female sauna protocol be?
+ Should dosage change throughout the month?
+ What keeps a cycle regular?
+ Does the body need more iron, magnesium, or protein at specific phases?
+ Should women fast?
+ Should recovery protocol change by phase?
+ What's the earliest detectable signal of perimenopause?
+ Can perimenopause be slowed?
+ How is cognitive load & mood affected?
+ Does stress impact men and women the same?
Kate has suspected endometriosis. 10% of all women do. We will try to tackle this too. I am excited for all of the surprising things we will hopefully uncover.
Unlike me, Kate does not have the innate desire to wake up at 4:30am and do six hours of longevity therapies.
She’s the cofounder of Blueprint, building in the trenches with me since day one. She understands the game and how hard it is.
In many ways, this is a sacrifice for her. She is a creative person, going from a life of freedom and spontaneity to a rigid protocol.
Traditionally, RCTs have been viewed as the gold standard. But RCTs have underserved women. The FDA banned women from clinical trials for 16 years (1977 to 1993), and most "medicine for women" is still medicine tested in men. Demanding RCT-only evidence for women's health is demanding evidence that doesn't exist. There is not enough practical scientific literature for women to reference only RCTs. It leaves half the population without a path to know what to do.
N=1 medicine is gaining ground and picking up where RCTs specifically fail. Individual science experiments give us signals that answer what to do on a day-to-day basis. This is even more important for women.
If you’re new to Kate and my world, I want you to understand that we have your back. Our intentions are to be a sturdy, reliable force in your life. To care for your best interest as we’d care for our own. We want what’s best for you and our loyalty is to your existence.
It’s pretty cool to be living in a time when we may be the first generation to not die. I’m not suggesting immortality, but lifespans so long that we stop thinking about lifespans.
At the end of the day, the one thing we each care about more than anything else is one more breath. I’m proud of Kate for taking on this responsibility. It’s painful, exhausting and costly.
The beginning of the world’s first n=2.
Cancer kills because it's caught late. Adialante is changing that by making mobile MRI accessible — dropping its costs to hundreds per scan and wait times to hours. Annual cancer screening will be the norm.
Congrats on the launch, @ET_adialante &
@ManW_dePlan!
https://t.co/9HlPNjExdl
We’re training models wrong and it’s due to chatGPT. Even the modern coding agents used daily still use message-based exchanges: They send messages to users, to themselves (CoT) and to tools, and receive messages in turn.
This bottlenecks even very intelligent agents to a single stream. The models cannot read while writing, cannot act while thinking and cannot think while processing information.
In our new paper, see below, we discuss LLMs with parallel streams. We show that multi-stream LLMs can …
🔵Be created by instruction-tuning for the stream format
🔵Simplify user and tool use UX removing many pain points with agents and chat models (such as having to interrupt the model to get a word in)
🔵Multi-Stream LLMs are fast, they can predict+read tokens in all streams in parallel in each forward pass, improving latency
🔵 LLMs with multiple streams have an easier time encoding a separation of concerns, improving security
🔵 LLMs with many internal streams provide a legible form of parallel/cont. reasoning. Even if the main CoT stream is accidentally pressured or too focused on a particular task to voice concerns, other internal streams can subvocalize concerns that would otherwise not be verbalized.
Does this sound related to a recent thinky post :) - Yes, but I don’t feel so bad about being outshipped with such a cool report on their side by 23 hours. I’ll link a 2nd thread below with a more direct comparison. I actually think both are complementary in interesting ways.
I’ve always believed the No.1 application of AI should be to improve human health.
That work started with AlphaFold, and now at @IsomorphicLabs with the mission to reimagine drug discovery and one day solve all disease!
We are turbocharging that goal with $2.1B in new funding.
FinalDose is building the first programmable drug platform - a single smart drug molecule that finds diseased cells by their DNA and destroys them. They're starting with all cancers.
Congrats on the launch, @Jeffliu6068Liu, @sklin_lite, and @liyaohuang2!
https://t.co/uKJgl7lpmR