Oh yeah I eat high animal fat and yes OQC never tested adipose yet but should. Yeah from you were saying seems like you need low fat to burn away the LA. I’ve tested a few times over the years and generally between 12-18% AA:EPA is still relatively high at 8:1 seeing something 1:1 and such low AA is wild
Yep points taken I would say look through that link I sent of the UK Biobank data and check it out pretty eye opening. Of course that takes some intellectual curiosity which many don’t have time for.. If you truly want whats best for your patients it’s good to have a balanced approach where you don’t just ignore all data that’s not in an RCT and hand wave away without also coming to grips with the huge caveats and limitations all pharma funded RCTs have which I’m sure you know a lot about.
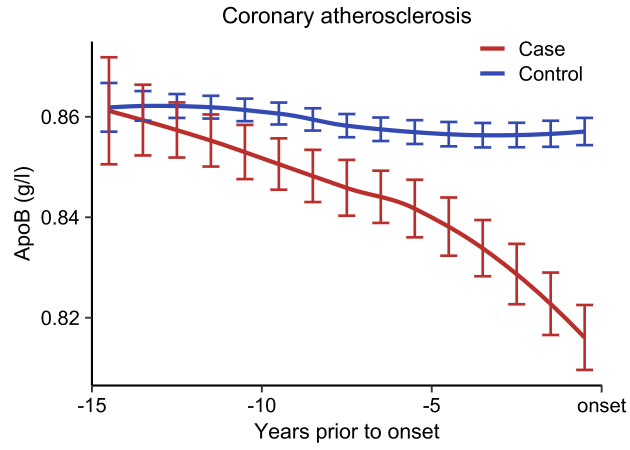
The question is what data are you basing it on, certainly not well powered observational data over time from say UK Biobank. Because if you did it would tell a different story. You can play around with the UK Biobank data here if you are curious: https://t.co/tM5PsNcnHk and when you tell me these data are flawed because of "confounders" check your priors. Why does ApoB drop decades before disease onset? At best you can say ApoB levels have poor discriminatory levels. The funny thing is LDL-c looks the same!
@AKA_Sadrien@trikomes Yeah good insights people miss n9 balance in this whole thing, also importance of nervonic acid which specifically attaches to sphingolipids (SM 24:1) is near essential
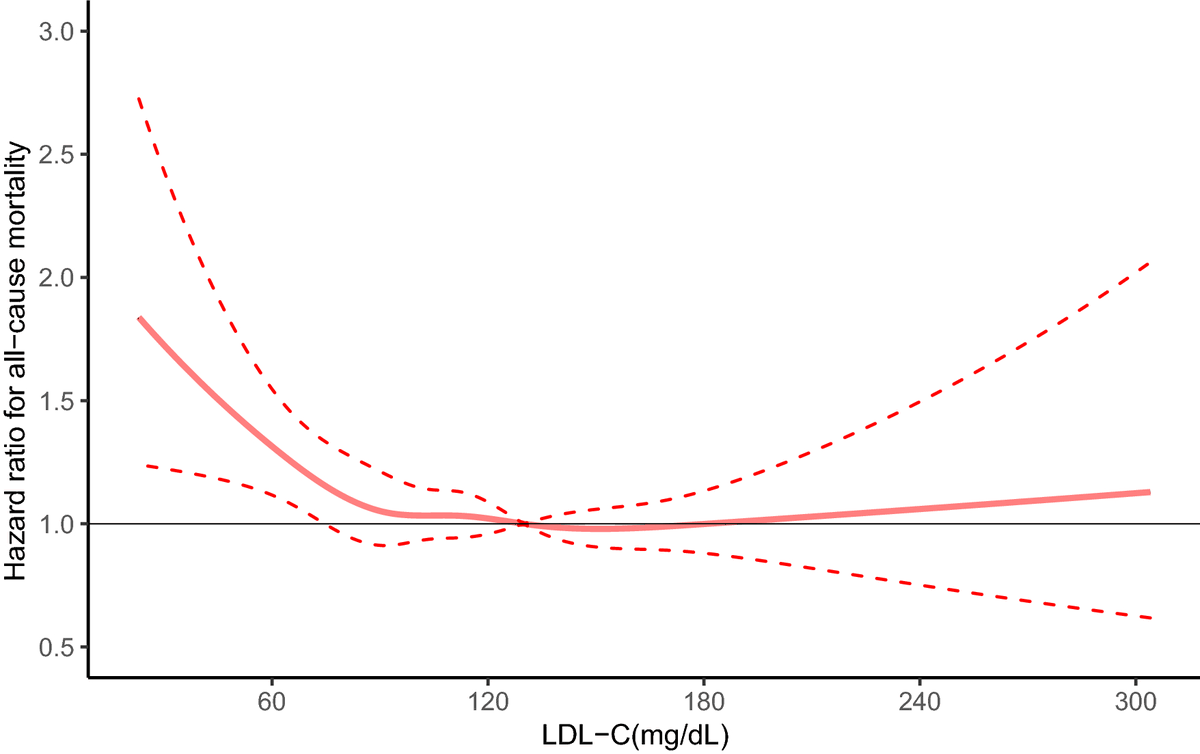
It's oxidized LDL that's the problem, and ApoB measures the number of particles that could get oxidized. Now this: to the people who claim low LDL is healthy and lower is better can't explain why mortality dramatically increases the lower your LDL-c gets.
NHANES study: PMID 34764414
@anonemus349832@ChrisMasterjohn@cremieuxrecueil Yeah but where does that oxidation come from not the saturated fat. All lipids with double bonds are susceptible to oxidation and then ROS comes off that.
Not sure any of this makes sense to me? What is a "toxicity threshold" and what are the better outcomes you are talking about? I guess one of my main points is we lump all fat together and talk about them only on the saturation level of the acyl chains but the head group and context and ratios and location and flux matter. TG-DHA is an inferior source of n3 than LPC-DHA for example.
@ChrisMasterjohn@cremieuxrecueil Yeah also I don’t think measuring one fatty acid circulating is sufficient to give you a picture of their oxidized n6 fat consumption and circulating lipids are not as instructive as long lived low turnover tissue lipids. You don’t want stem cells with high LA low n3..
So serum linoleic acid is not a good read out for consumption of factory produced industrial vegetable oils.
Things to consider when interpreting serum fatty acid data are it’s not RBC or tissue based so more transient, it doesn’t tell you which lipid type the LA chain is on (big difference between plasmalogen 18:2 vs TG 18:2), also ratios matter more in this than raw concentration and n6 and n3 need to balance 3:1 ideally or lower so AA:EPA is a better read out of increased n6 consumption due to how the enzymes work and the ratio with omega 3 fats matter more. Also it’s the tissue balance of LA in ratios with other fats that matter the most. Lipid ratios are tightly controlled and enzymatic SNPs in the eicosanoid pathway based on genetics can change individual FAs but you need the full fatty acid profile in ratio with omega 3 to see the whole picture and it needs to be RBC. I’ve seen well powered RBC based n6:n3 ratios and when it gets higher in UK biobank it’s not good higher CVD and mortality.
Yes and people will say it’s because inflammation itself lowers cholesterol, called the lipid paradox but wrote an article recently that you can also think of it the other way around LDL-c has critical immune functions and is part of the innate immune system can protect vs infection those with sepsis and high LDL-c do better. I don’t think the lipid paradox is really a paradox https://t.co/EPEVTTGifp