#acc26 Six reasons why CHAMPION AF should not change oral anticoagulation for AF
I will have a formal post up on @theheartorg but here is a short summary
1) Stroke and Ischemic Stroke went the wrong way.
All S -> 33 vs 50 [HR 1.46 95% CI, 0.94-2.27)]
IS -> 27 vs 45; [HR = 1.61; 95% CI, 1.00-2.59)]
Look at those upper-bounds.
2) NI would not have been met for efficacy had they used a margin with both rate ratio and risk difference, which is standard practice.
The margin of 4.8% is based on event rates at 12%, which is 1.4 in relative terms (40% higher). But when event rates come in lower, as they did: 4.8% vs 5.7%, the 4.8% margin is too lenient.
The 0.9% higher rate of the primary endpoint has a 95% CI of (-0.8-2.6%), so 2.6% is less than the margin of 4.8%. Now do it with relative risk.
It's in table 2. The relative risk is 1.20. The 95% confidence intervals were 0.87-1.66. Note that 1.66> 1.40 so LAAC is not noninferior based on rate ratio margins
3) The primary safety endpoint is flawed because it excludes periprocedural bleeding and uses nonmajor bleeds, such as gum bleeds and bruising. It's open label trial so who which group will complain of more nonmajor bleeding?
4) When counting all events, Watchman barely reduced major bleeds. Also in the main results table is that major bleeds were 83 vs 87 (5.5% vs 5.8%; HR 0.92 95% CI 0.68-1.24)
5) Net Clinical Benefit was also flawed because they used nonprocedural bleeding and nonmajor bleeds.
A normal patient would simply say, there were 17 more strokes and only 4 less bleeds. Hardly a good trade.
6) Bayes: trials don't give answers, they update priors. For Watchman, you have PREVAIL failing against warfarin, CLOSURE AF clearly failing against best med Rx (mostly DOACs) so priors are pessimistic. To go from pessimistic priors to enthusiastic posteriors you'd need hugely positive data. CHAMPION is not that.
Don't believe the stories that CLOSURE failed due to them using other LAAC devices. In the AMULET IDE trial, Watchman and Amulet were similar. Also, if you believe that German operators are worse than US authors, you need to travel more.
Conclusion: Oral anticoagulation for AF is one of the most evidence-based practices in all of medicine. To upend that would take much stronger data.
Don't be bamboozled by this trial, which was designed to be positive before the first patient was enrolled.
#ACC2026
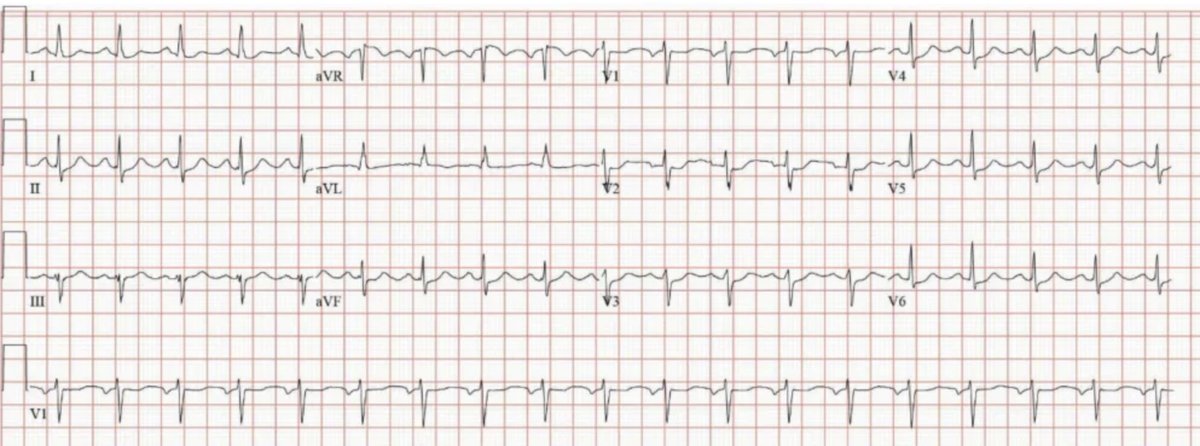
Exactly like everyone has stated. There’s OMI sign diffusely hard to determine culprit. Echo showed distal septal and apical WMA. LHC showed RCA dominant with 30% stenosis through LAD, LCx and RCA. Total occlusion at distal diag-1, thought to be 2/2 emboli!
I have decided. No cardiology (or EM) trainee should be credentialed unless they can pass a simple ECG reading course. I am sorry, but the ECG read is often a life or death test. It costs a few dollars and is done in seconds. Maybe AI will get there, but it is not there yet. And AI will not be able to use prior Pb distribution;
@ecgandrhythmRoe NSVT;
V1: LBBB pattern ->RV or septal
I: downright -> lateral or apical
Inferior leads: upright -> inferior axis
Precordial transition at v3
V1 + inferior leads + precordial leads make me think RVOT, but lead I doesn’t fit the picture? 🤔
@ecgandrhythmRoe 1st strip PVC bigeming
2nd strip PVC trigeminy, the prolonged PR might be a result of delay conduction 2/2 PVC retrograde conduction causing AV node to be in refractory?
@ecgandrhythmRoe Patient hx/age medium pretest probability. Interested in any cardiac risk factor. ECG not diagnostic with possible HATW-looking aVL and STD in III. For me, overall low-med confidence for OMI. Will do serial ECG/trop, and echo for lateral WMA. Excited to learn!