Detecting lung cancer 5 years before it happens, in @CellCellPress courtesy of the @CharlesSwanton group.
Astonishing translational work !
https://t.co/EvUmIGVLgs
#ASCO26
This one is special.
This is the hottest paper of 2026 and potentially in the history of pancreatic cancer.
Let’s dive in.
RASolute 302: Daraxonrasib vs investigator’s choice chemotherapy in previously treated metastatic pancreatic cancer
Abstract LBA5 (soon!)
Presentation: May 31, 2026, 3:21-3:33 PM CDT
For decades, pancreatic cancer has been where good ideas go to die.
We have optimized chemotherapy. We have sequenced chemotherapy. We have celebrated modest gains.
But the central driver of PDAC has always been sitting there in plain sight:
RAS.
More than 90% of pancreatic cancers have oncogenic RAS mutations, and until recently, we had essentially nothing direct to do about it.
Daraxonrasib is an oral RAS(ON) multiselective inhibitor targeting the active GTP-bound state of mutant and wild-type RAS.
And in RASolute 302, it delivered.
Quick hits:
📌 Phase 3 international randomized trial 500 patients with previously treated mPDAC Daraxonrasib vs investigator’s choice chemotherapy
🧬 RAS G12 population
91.8% of patients had RAS G12 mutations
📈 OS in RAS G12 population
13.2 vs 6.6 months
HR 0.40
P<0.001
📈 OS in overall population
13.2 vs 6.7 months
HR 0.40
P<0.001
📊 PFS in RAS G12 population
7.3 vs 3.5 months
HR 0.45
P<0.001
📊 PFS in overall population
7.2 vs 3.6 months
HR 0.49
P<0.001
🔥 12-month OS
Overall population: 53.2% vs 17.3%
⚠️ Toxicity matters, but this was not just more efficacy for more toxicity
Grade ≥3 AEs: 61.8% vs 69.6%
TRAEs leading to discontinuation: 1.2% vs 11.2%
This is the kind of survival curve we almost never get to see in pancreatic cancer.
This validates RAS(ON) inhibition in the most RAS-addicted major cancer. It takes a target we have talked about for decades and turns it into a clinically meaningful survival benefit in a randomized phase 3 trial.
The next questions come fast: 1L combinations, maintenance, perioperative disease, sequencing, resistance, toxicity management, and whether this becomes a new backbone.
RAS is here, and it couldn’t have come sooner.
https://t.co/Y4WJRlRRTk
@TheGutonclab@UGrewalMD@TimothyJBrownMD@OncoAlert@Onco_Nexus@ASCO@NazliDizman@LauraAlderMD@DVAraujoMD@DrBarbiOnc@LauraEsfeller@FunchainMD@YGaritaonaindia@DrSAHaddad@jgong15@iandresmeraz@SakditadMD@RamilaShilpakar@RohitBanwar@lungoncdoc
🚨 Prostate cancer care has changed fast. Here’s the 2025 snapshot.
The new Lancet Seminar lays out how prostate cancer management has transformed across the disease spectrum 🌍🧬
🔍 Early disease
Active surveillance is the default for low-risk tumors, avoiding overtreatment while maintaining excellent outcomes. MRI-first pathways improve detection of clinically significant cancer.
⚖️ Localized to high-risk
Surgery and modern radiotherapy offer equivalent cancer control. Hypofractionation and SBRT shorten treatment without compromising efficacy. High-risk disease needs multimodality care.
🚀 Metastatic hormone-sensitive
ADT alone is no longer enough. Doublet or triplet therapy with ARPIs ± docetaxel is now standard, with prostate RT benefiting low-volume disease.
🎯 mCRPC era
Treatment is biology-driven: PARP inhibitors for HRR alterations, Lu-177 PSMA radioligand therapy after ARPI and taxanes, cabazitaxel preferred over ARPI sequencing.
🧠 Big takeaway
Sequencing, patient selection, toxicity, and shared decision-making matter as much as drug choice.
📖 Valérie Fonteyne et al. Lancet 2025
A must-read, practice-defining review for every GU oncologist 🔖
#OncoTwitter #MedTwitter #ProstateCancer #GUOncology @TheLancet@myESMO@OncoAlert@ASCO
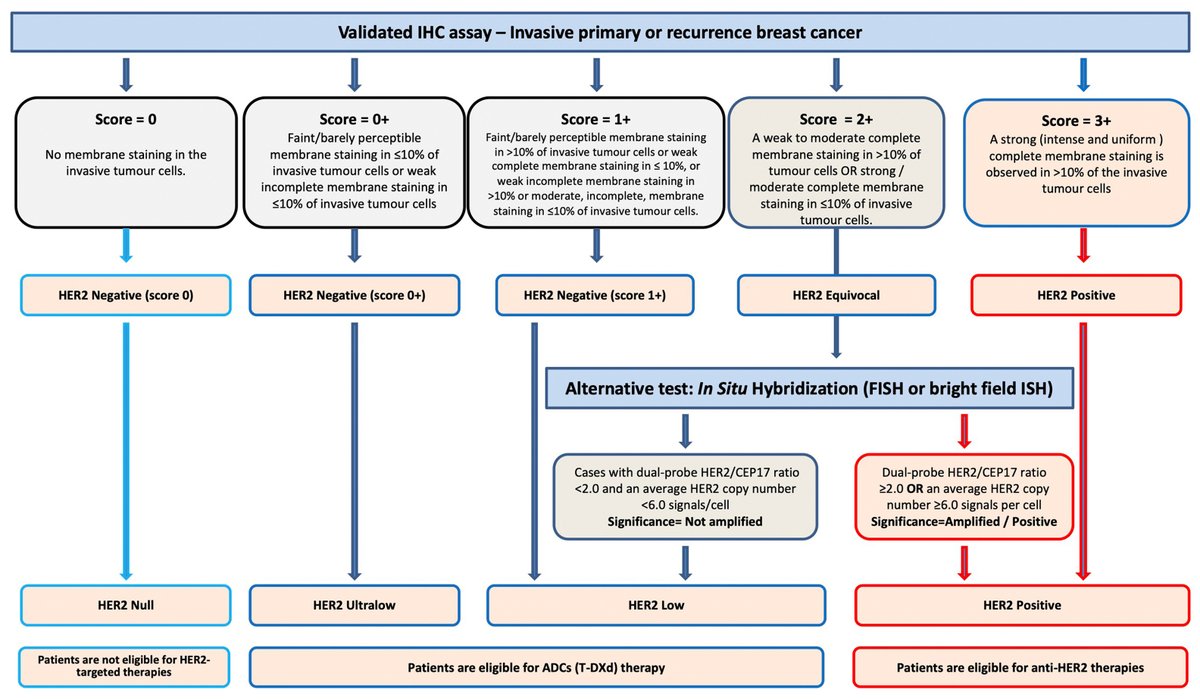
Evolution of HER2 Classification
The story of HER2 has moved beyond the binary of positive and negative; it’s now an evolving spectrum from low to ultralow to null—where the gray tones of biology are rewriting clinical decisions
Recommended HER2 Algorithm👇
https://t.co/vdBZMym44R
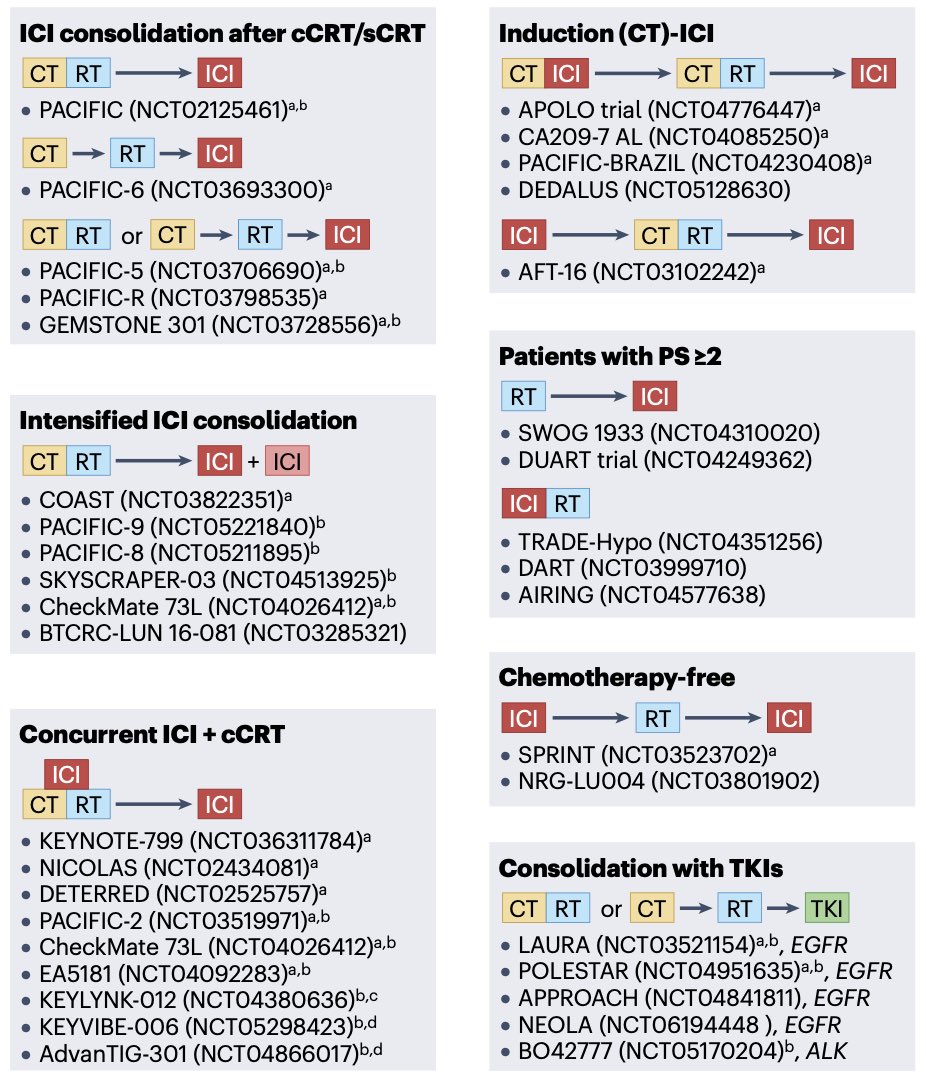
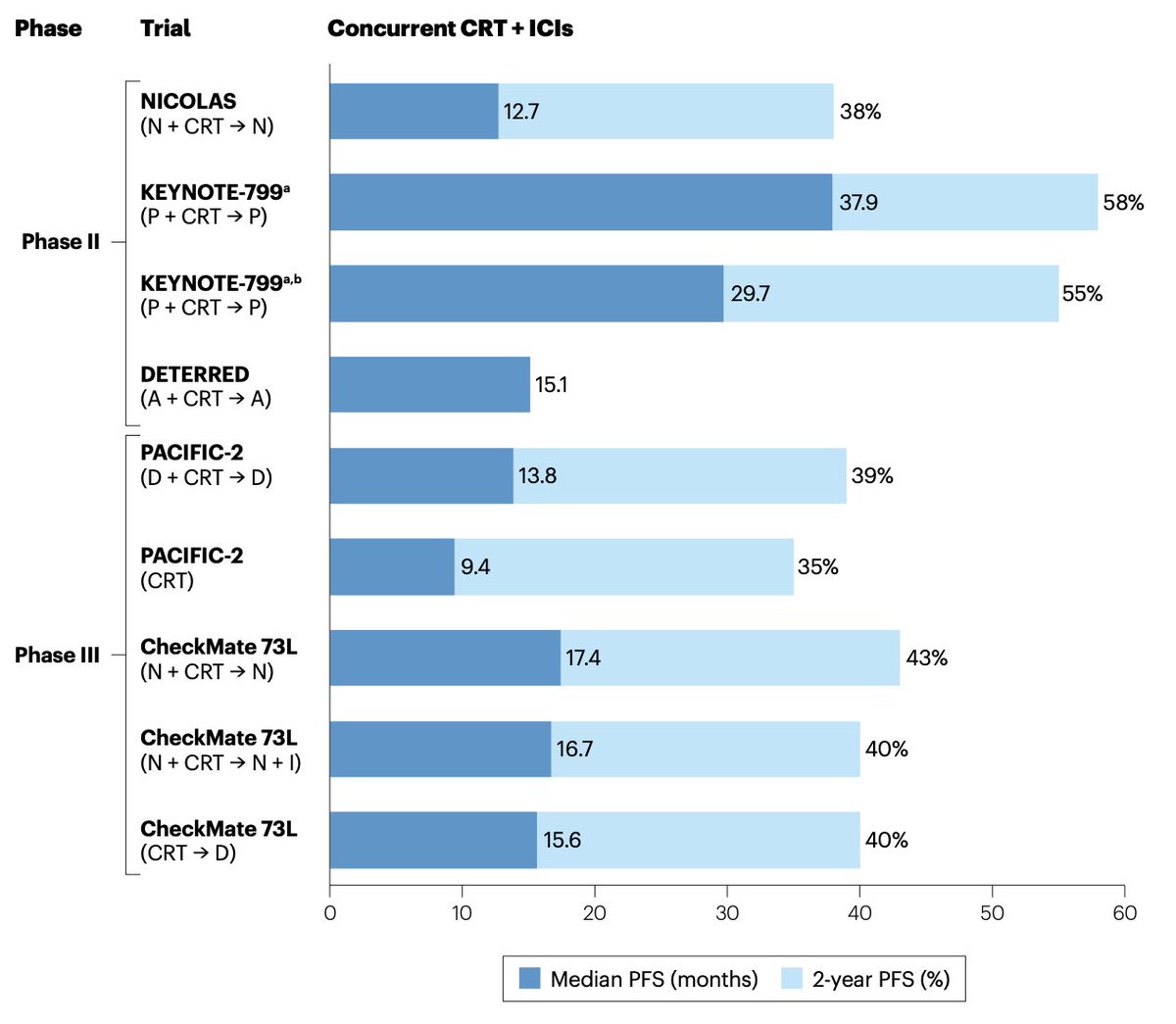
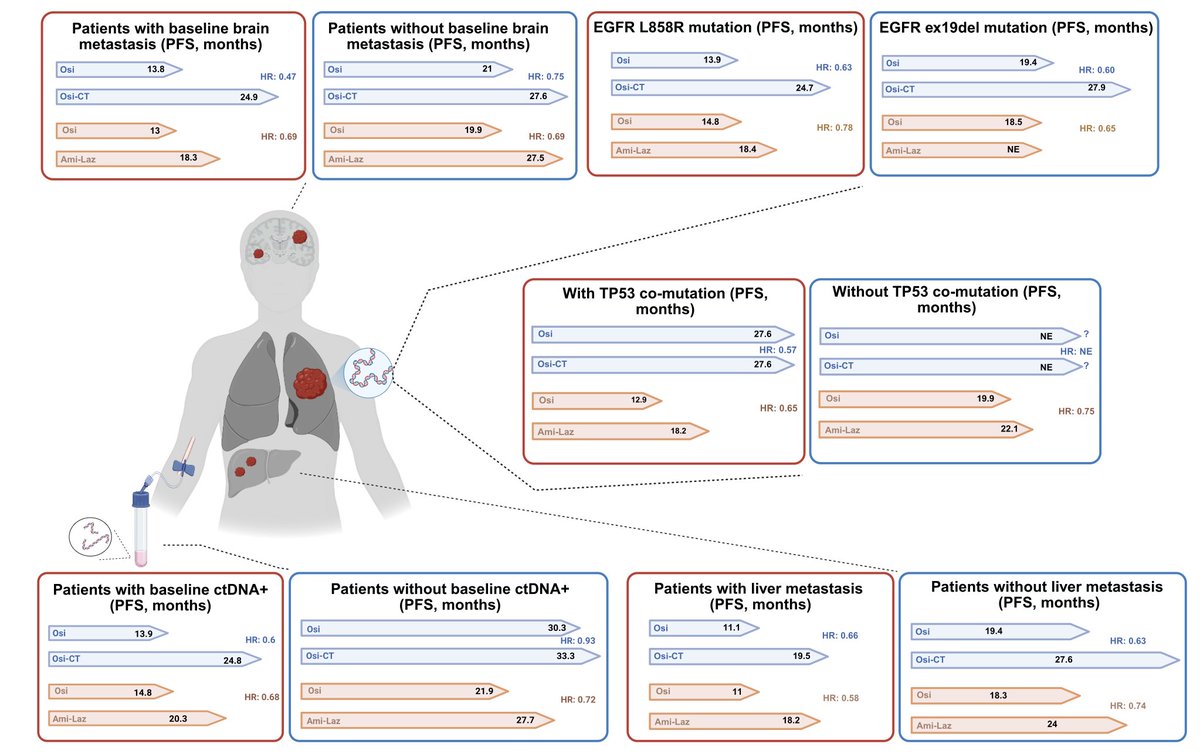
🫁 Unresectable stage III NSCLC: current landscape and future directions.
Durvalumab after chemoradiotherapy is standard, and osimertinib has transformed outcomes in EGFR-mutant disease.
ctDNA monitoring, novel radiotherapy, and chemo-ICI combinations may further refine treatment.
📖 @NatRevClinOncol@JordiRemon
DOI 👉🏻 https://t.co/4zC4lW8TPH
#CánCare #lcsm #NSCLC
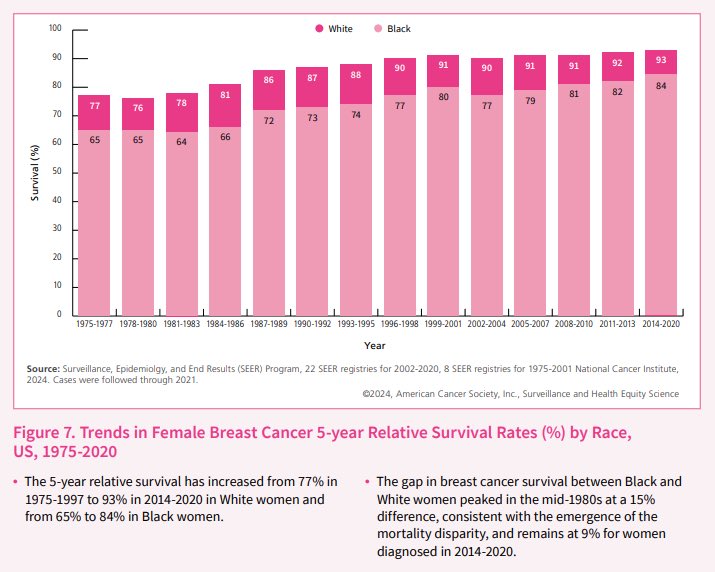
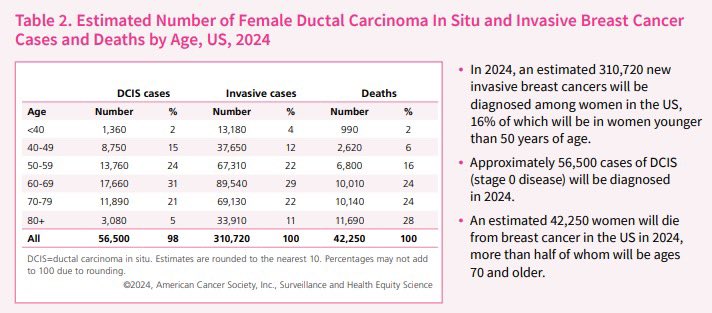
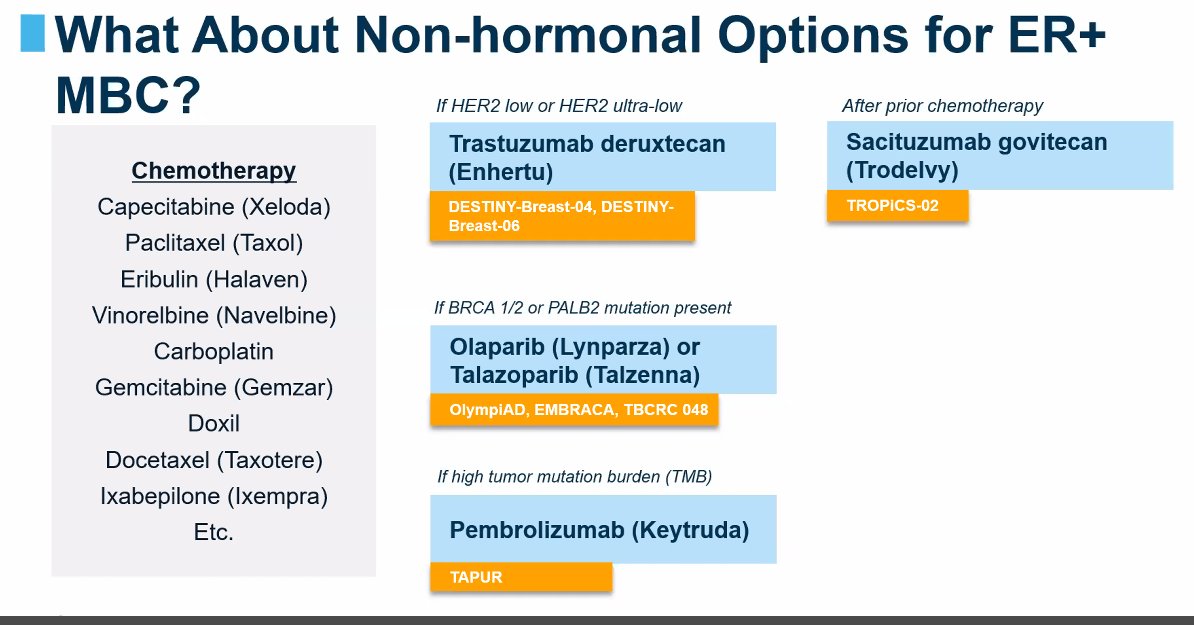
Breast Ca still remains the most common cancer in women (1 in 8 risk), with ⬆️300,000 new US cases yearly.
- Most recommend yearly mammograms starting at 40.
- Early detection=Early disease=Better outcomes (Rx paradigm 👇👇 by @IlanaSchlam)
#BreastCancerAwarenessMonth
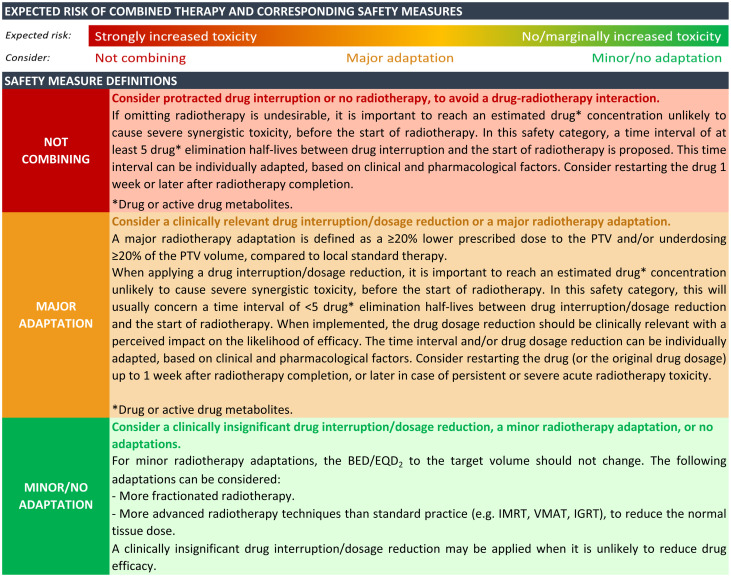
🆕article in press: ESMO-ESTRO consensus statements on the safety of combining radiotherapy with immune checkpoint inhibitors, VEGF(R) inhibitors, or multitargeted tyrosine kinase inhibitors @myESMO@ESTRO_RT
https://t.co/ixNmuaZa6G
📌 Prostate cancer remains the most common non-skin cancer in men, with >1.4M cases annually worldwide.
Advances in risk stratification, AR pathway inhibitors & chemo are reshaping management, but metastatic disease survival is still poor.
📖 @JAMA_current
DOI 👉🏻 10.1001/jama.2025.0228
#CánCare #oncology #prostatecancer
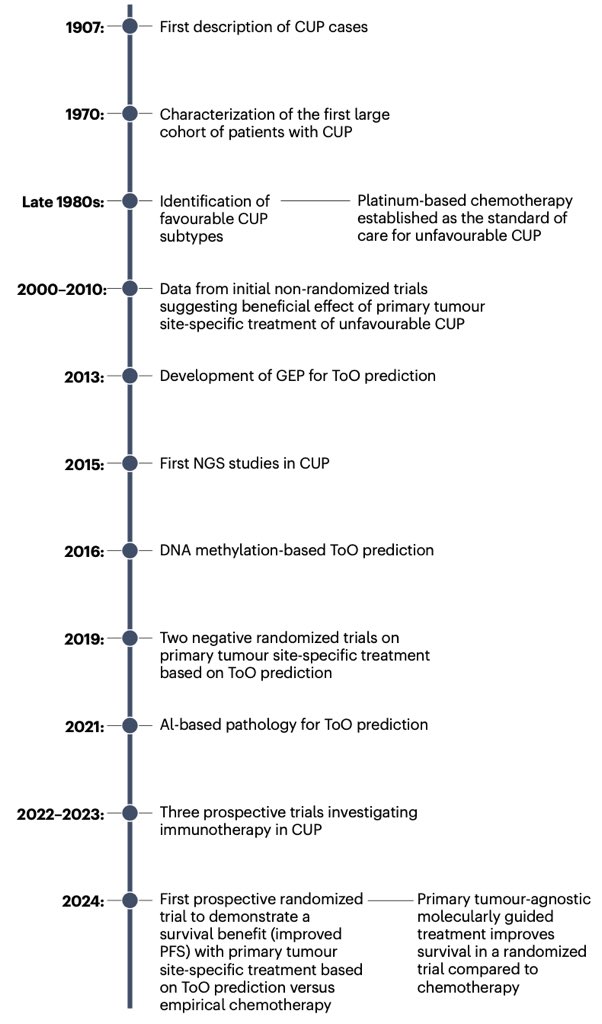
🚨 Cancer of unknown primary (CUP) has long been a therapeutic challenge with poor outcomes.
New data show that molecularly guided therapy and immunotherapy can improve survival, while ctDNA, methylation profiling, and AI-based pathology enable precision strategies.
📖 @NatRevClinOncol
DOI 👉 https://t.co/JelxgNVLUk
#CánCare #oncology #CUP #precisiononcology
Este folheto informativo foi elaborado para os doentes com TNE para os orientar passo a passo na sua jornada de tratamento. Disponível em 15 idiomas. Baixe agora --> https://t.co/ekWhXLmXPv
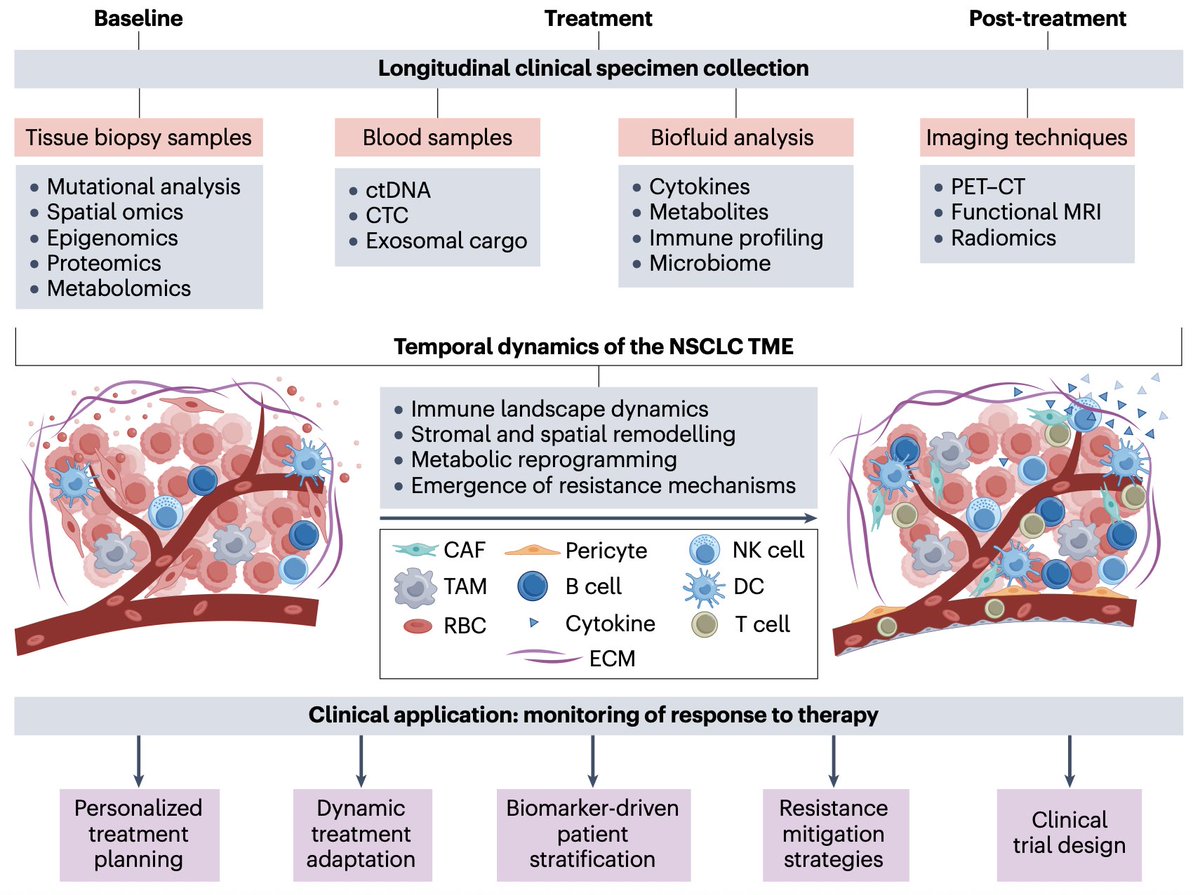
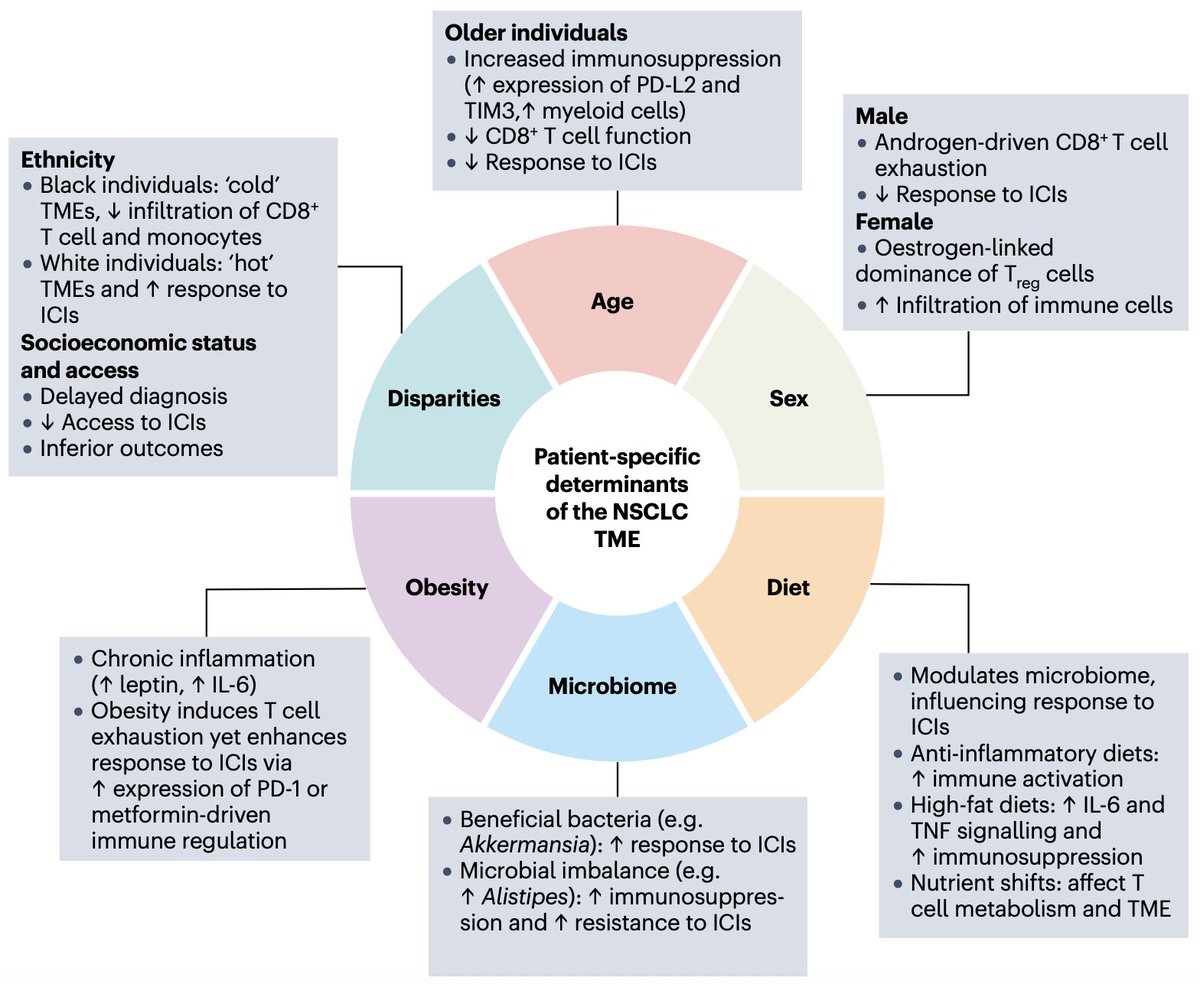
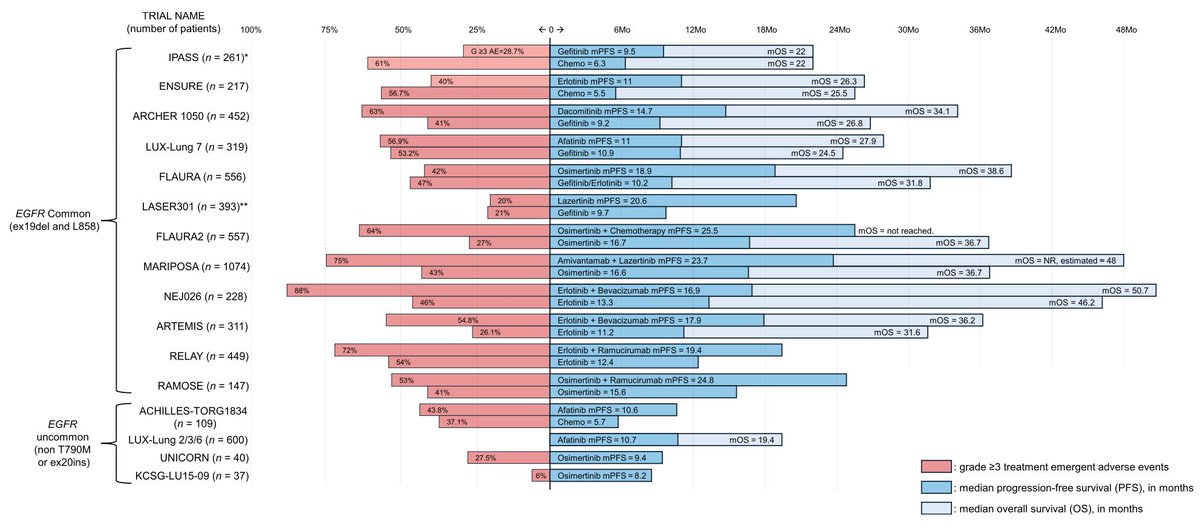
Mutations in the tyrosine kinase domain of EGFR represent one of the most common druggable alterations in #NSCLC. This recent review provides a comprehensive clinical overview of the management of patients with EGFR-mutant NSCLC.
https://t.co/DsurY1HqxY
@OncoAlert@Alfdoc2