Anyone still love dig like I do? This comprehensive perspective @JCardFail summarizes everything you need to know and think about in the contemporary landscape of #FunctionNotFailure@HFSA
https://t.co/P327ZxBwbN
ARISE-FLUIDS has arrived and it's awesome 🥳
For over a decade, the Surviving Sepsis Guidelines recommended that septic patients get at least 30 cc/kg fluid. In the United States, these guidelines were weaponized into performance metrics, pressuring clinicians to prescribe arbitrary volumes to every patient.
Evidence-based clinicians have LONG known that this guideline lacked evidentiary support. For example, I've attached a picture of a blog I wrote about this back in 2017. Despite the lack of evidentiary support and some evidence of harm, the Surviving Sepsis Guidelines INSISTED on perpetually recommending 30 cc/kg fluid resuscitation.
We finally have a prospective RCT demonstrating that mandating early administration of 30 cc/kg fluid (as compared to early vasopressors) doesn't help and may actually cause harm.
It's important to note that all of the hard endpoints in this trial were neutral (e.g., mortality, days free of organ support).
I still think that 30 cc/kg fluid is a pretty reasonable volume of fluid for *most* patients. But the study does suggest that giving too much fluid may promote edema - so we should be *thoughtful* about this intervention rather than mandating it for every septic patient.
Based on the subgroup analysis, the fluid-conservative strategy may have helped the subgroup of pneumonia patients the most. This is statistically nonsignificant but aligns with my expectation. ARDSy patients often don't respond well to fluid. (In contrast, I really doubt that a liter of fluids in either direction matters for most urosepsis patients.)
This is a great example of the over-reach of guidelines and protocoled medicine. People get all upset about practice variation, so sometimes they try to stomp it out using guidelines and protocols. But these guidelines are highly fallible, so what may occur is that you standardize care in a way that harms everyone equally. 🤦♂️
Cardiovascular considerations BEFORE cancer therapy🫀
The first of a 3 part #JACCCardioOnc Expert Panel series exploring CV care before, during, & after cancer therapy.
🫀Goals of CV evaluation Prior to cancer therapy:
📍Identify and treat subclinical CVD and cardiovascular risk factors 📍Optimize management of pre-existing CVD and cardiovascular risk factors 📍Perform targeted risk assessment to help inform cancer treatment decisions 📍Establish baseline cardiovascular function 📍Optimize primary prevention therapies 📍Plan cardiovascular surveillance during treatment
🫀Current tools include clinical assessment, biomarkers, 12-lead ECG, #EchoFirst, & risk scores
🫀Important evidence gaps includes cardiotoxicity mechanisms, impact of pre-treatment CV evaluations on clinical outcomes, validation&implementation of risk scores, & the role of AI.
Read more in @jaccjournals: https://t.co/cTCY0Acg99
#CardioOncology
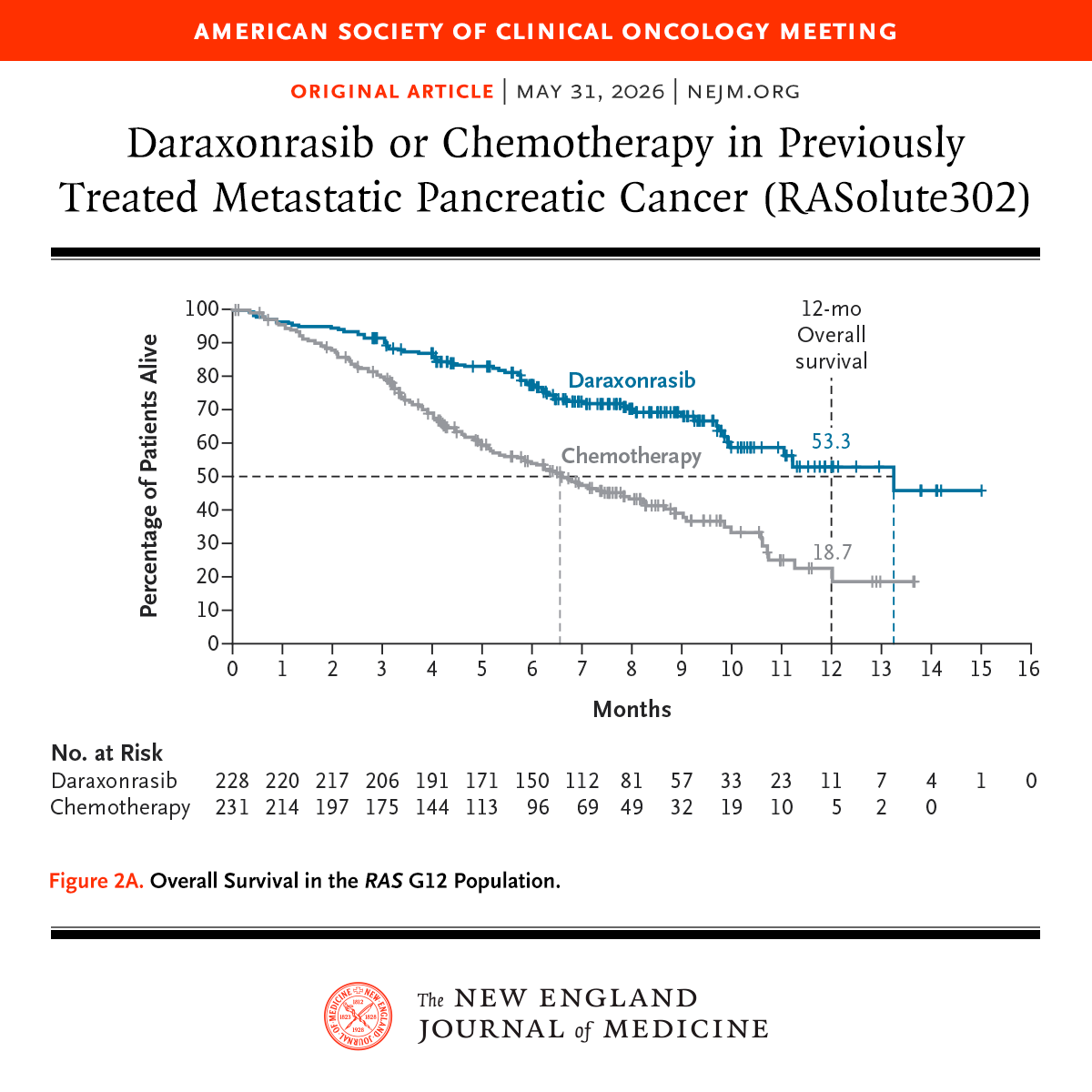
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
Just published on @ESC_Journals
Intracoronary imaging for left main percutaneous coronary intervention: a clinical consensus statement of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC and the European Bifurcation Club (EBC) https://t.co/Fe6iDNuwZD
Semaglutide and walking capacity in people with symptomatic peripheral artery disease and type 2 diabetes (STRIDE): a phase 3b, double-blind, randomised, placebo-controlled trial - The Lancet https://t.co/wWPWfKJAvI
Management of Peripheral Artery Disease in Adults With Diabetes: 2025 ACC Scientific Statement: A Report of the American College of Cardiology | JACC https://t.co/SxcMPGnxTs
REC-CAGEFREE I: DCB Angioplasty With Rescue Stenting vs. Intended DES in Patients With de novo Noncomplex Coronary Artery Lesions - American College of Cardiology https://t.co/UcBjjshrc0
SCAI Door to Lactate Clearance (SCAI DLC) Cardiogenic Shock Initiative: Definition, Hypothesis, and Call to Action - Journal of the Society for Cardiovascular Angiography & Interventions https://t.co/KnvYjzHxAd