A really thought-provoking study at #ASCO26 (Abstr 4512, Clinical Science Symposium): decision regret after adjuvant pembrolizumab in RCC.
🔹 The question
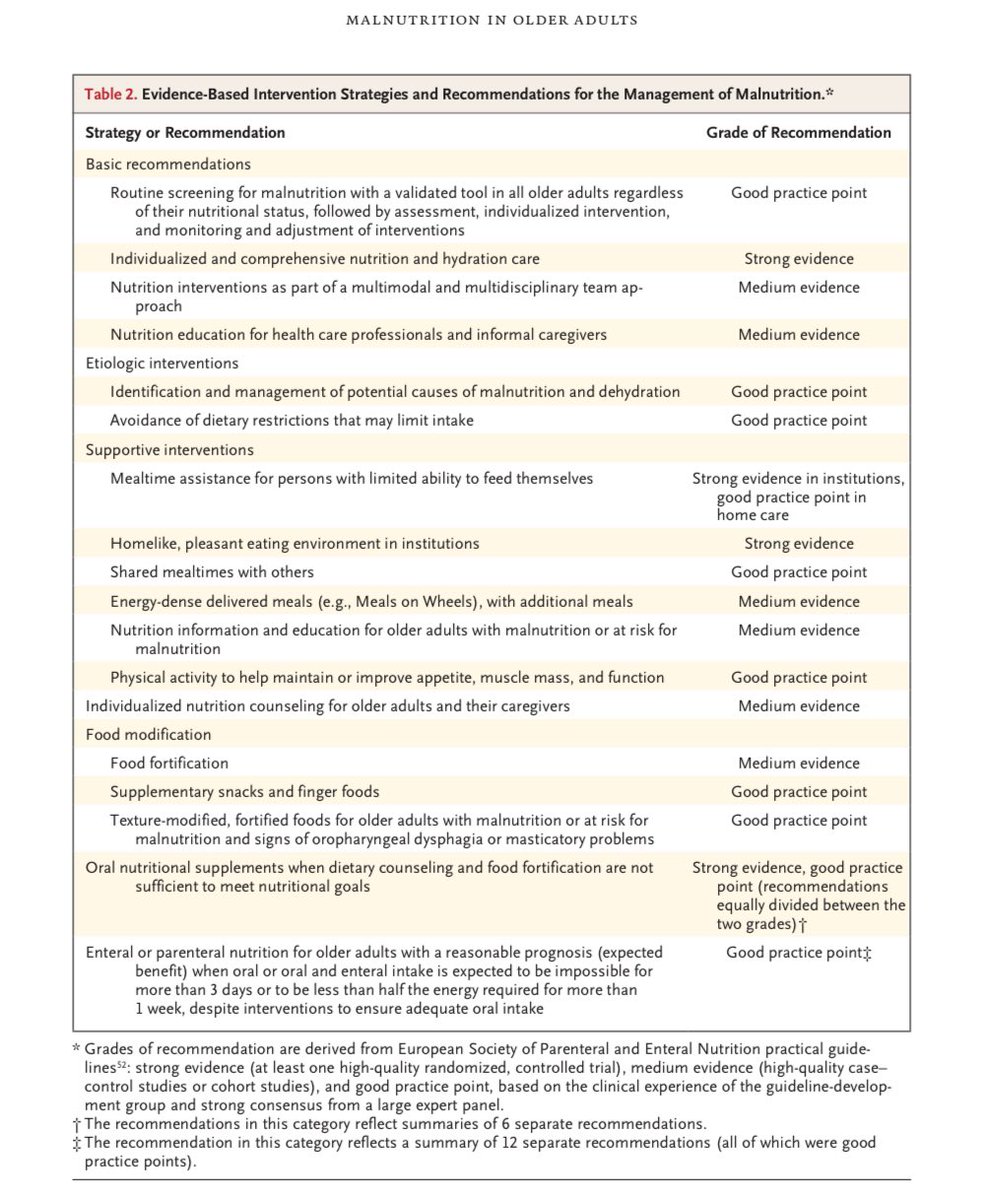
Do patients regret receiving adjuvant pembro — and if so, is it driven by long-term toxicity that CTCAE grading doesn't adequately reflect? They built a patient co-designed tool focused on long-term toxicity.
🔹 The study
104 RCC pts post-adjuvant pembro across 3 London centres, median f/u 30 mo. Pts completed the Ottawa Decision Regret Scale alongside their own rating of irAEs as life-changing, significant, or non-significant.
🔹 What they found
28% rated their toxicity as significant and 11% as life-changing — but these ratings did NOT correlate with CTCAE grade (a third of G1–2 events were rated significant), and regret was identical for G1–2 vs G3–4 irAEs. Regret was driven by patient-perceived long-term toxicity, especially permanent endocrine and MSK irAEs — and not by disease recurrence (only 1/14 who relapsed expressed regret). Lower baseline expectations of toxicity → more regret.
🔹 My take
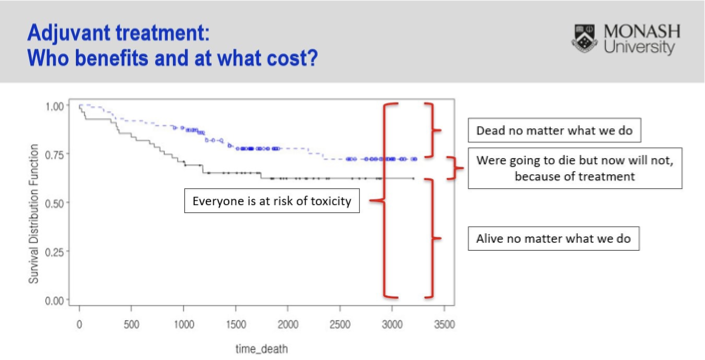
Striking that >1 in 4 reported significant and >1 in 10 life-changing toxicity. What concerns me most isn't that CTCAE missed these events — it's that the grade didn't correlate with how significant patients found them, nor with regret at all. That deviates from the very purpose of grading. The hard part: a regret analysis is tough to contextualize when the alternative, no treatment, risks recurrence — arguably worse than a long-term toxicity. Adjuvant therapy is challenging by nature: most patients are either cured already or destined to recur regardless — we expose everyone to toxicity to benefit a minority. We urgently need biomarkers to find the few who truly benefit. This slide from @Prof_IanD says it all 👇
Looking forward to seeing the presentation!
🔗 https://t.co/laVM7xBbxr
#kcsm #ASCO26
@BethN01@tompowles1
Wow! The absolute BEST symptom management & survivorship committee meeting @SWOG spring meeting! Energized & Excited after the brainstorming session! Cannot wait for the future! ☀️🕶️#APP#Research#scientist#collaboration
Fascinating, important convo on the role of APPs in #clinicaltrial research & patient access to trials. APPs have been an important part of my cancer experience, including a PA who advocated to get me scanned the night I was diagnosed. Let’s break down the barriers! #SWOGSpring26
Highlights from @SWOG’s high-impact oncology trials & future vision 🧬 by our new #SWOG co-chairs, @PrimoLaraMD@DrDawnHershman
✅ S1609 DART: 53 rare cancer cohorts, one basket study
✅ ctDNA clearance predicts outcomes in NSCLC
And so many more!
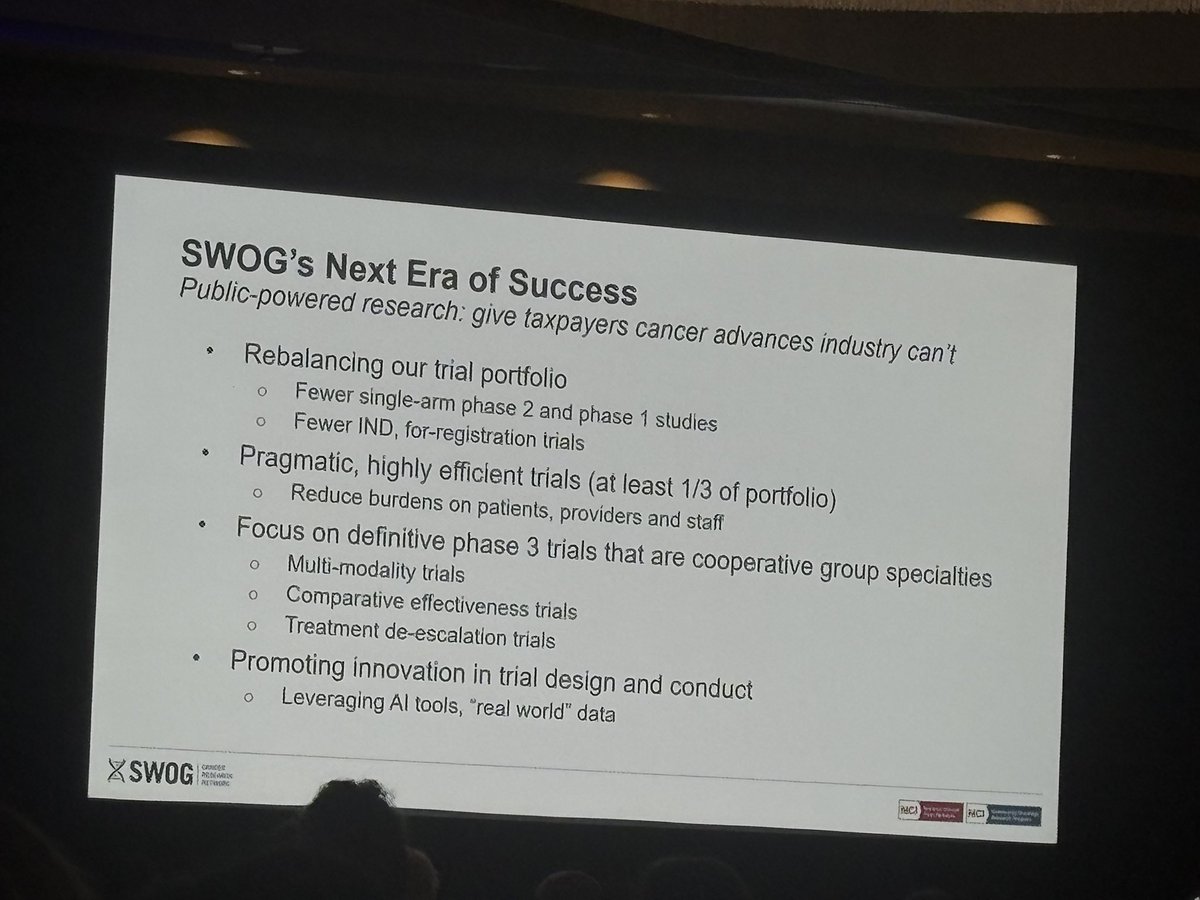
🔭 SWOG’s next era: public-powered research tackling what industry can’t 🚀
• Fewer phase I → more definitive phase III trials 📊
• Pragmatic, efficient studies (⅓ of portfolio) ⚡
• Multi-modality strategies & treatment de-escalation 🎯
• AI + real-world data accelerating innovation 🤖📈
@SupportingSWOG
#Oncology #ClinicalTrials #CancerResearch
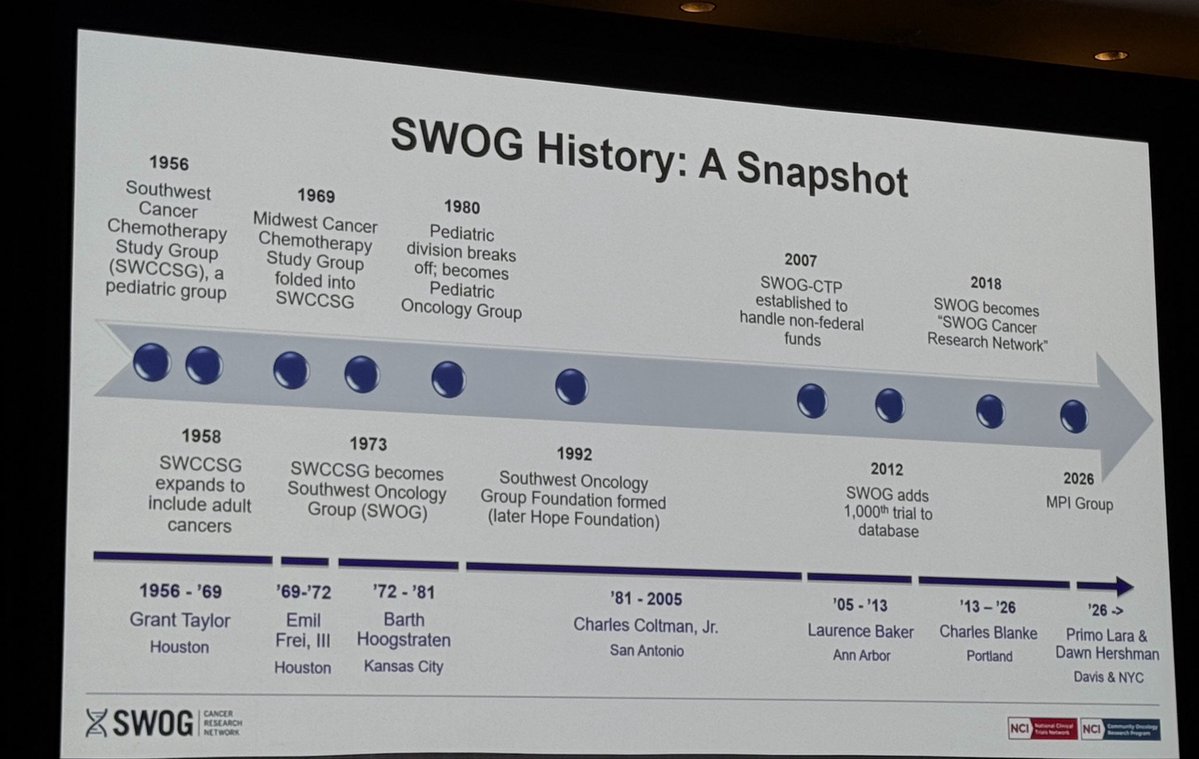
In the 2026 @SWOG plenary session, new co-chairs @PrimoLaraMD@DrDawnHershman honor the outgoing chair @CharlesBlanke & share SWOG’s history, extensive membership, accomplishments& their vision on next generation of @SWOG trials (important for young investigators to know)👇
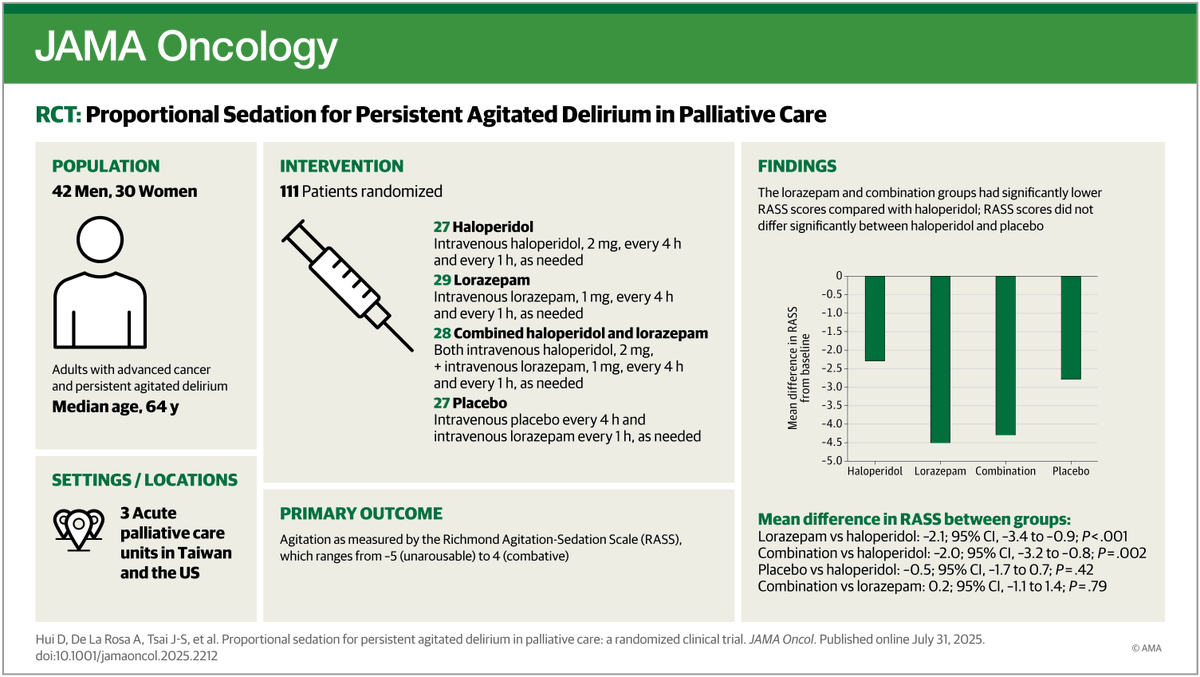
Scheduled lorazepam, alone or combined with haloperidol, more effectively reduced agitation and restlessness in palliative care patients with advanced cancer and delirium than haloperidol or placebo. https://t.co/aZIYoeFRzs @drdavidhui
Microsoft claims their new AI framework diagnoses 4x better than doctors.
I'm a medical doctor and I actually read the paper. Here's my perspective on why this is both impressive AND misleading ... 🧵
Happy Birthday to MD Anderson!
As @DGlaucomflecken recently told us, growing up as a child in Deer Park, Houston, he simply couldn’t figure out why the good “Dr. Anderson” had the “MD” before his name. 😆
P.S. - it’s Monroe Dunaway
#AI has improved my efficiency in clinic. But in other industries, AI in the name of efficiency turns employees into "Quantified Workers". #Doctors aren't immune. In @NEJM,@CohenProf@iajunwa & I propose a Clinician Bill of Rights to prioritize autonomy during the AI revolution
Did you know you can donate blood in honor of an @MDAndersonNews patient? If they don't need🩸, they get an honorarium credited to their account. I'm giving platelets today in honor of one of my pts. Talk about immediately reducing #financialToxicity in small but measurable ways!
This painting (Fildes’ The Doctor) is like a Rorschach test of how I’m feeling as a physician
Often I see the virtue of presence, where we literally cultivate our bedside manner
Other times I discern the intractable progression of disease we are powerless to halt
It’s both
Two reasons for caution in our expectations for how AI may affect administrative overhead in healthcare are:
- Most areas of admin friction were readily addressable through the technology of 10-20 years ago, but remain with us
- Most problems are not computational at their core
Our patients deserve honest prognostic discussions and quality EOL care. Even "novel" therapies don't change the fundamental importance of knowing when to shift focus from disease-directed to comfort-focused care
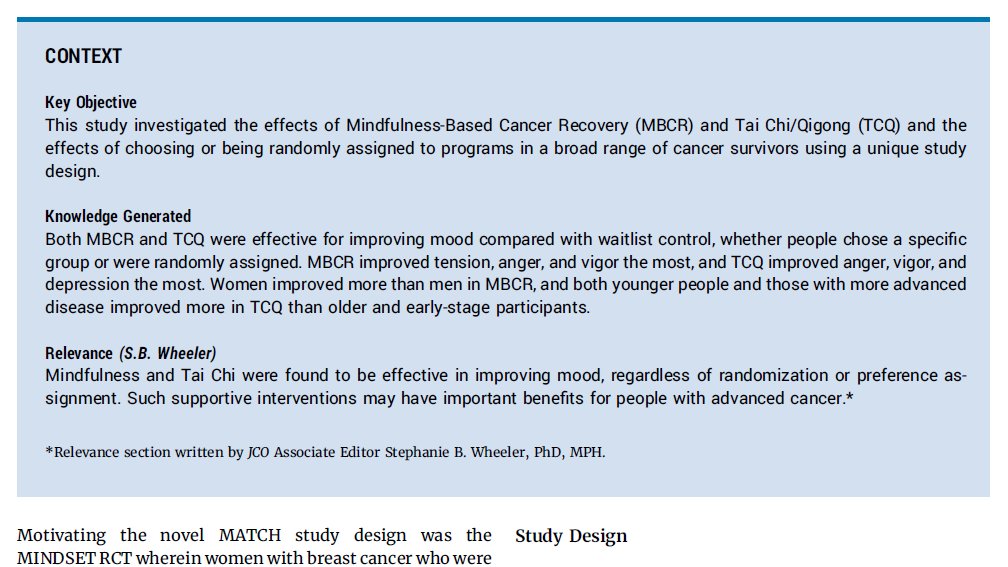
Very excited the primary psychosocial outcomes of the MATCH (Mindfulness and Taichi for Cancer Health) trial were published today in the @ASCO Journal of Clinical Oncology. Largest comparative trial of #mindbody therapies to date.
Free full-text here: https://t.co/r8D3SGqD97
Important reading for all clinical trialists: always be aware of (and transparent about!) the event „classification“ for your study endpoints. Great work by @ABCSGVienna led by Dominik Hlauschek! https://t.co/6cy1hUAYCY @MedUni_Wien