We prescribe statins to prevent heart attacks and strokes. But could they also prevent frailty?
We already consider statins in older adults for CV risk. This adds another reason to have that conversation.
Frailty prevention may be a statin benefit hiding in plain sight.
New research shows SGLT2i + GLP-1RA may work synergistically against atrial fibrillation
In patients undergoing CABG, AF tissue showed ↑ inflammation, NF-κB activation, oxidative stress & fibrosis.
In vitro, combining both drug classes reversed these pathways
New data on finerenone in CKD: per 1000 patients treated over 3 years, it prevented 33 composite kidney/CV events in diabetic patients and 40 in non-diabetic patients — with only a modest increase in hyperkalaemia hospitalizations (~9–10 events).
Most echocardiography laboratories have adopted the 2016 diastolic guidelines. With the release of the 2025 update, an important question arises:
What are the key conceptual differences between the 2016 and 2025 approaches to diagnosing diastolic dysfunction?
https://t.co/FPkUqRtmYd
@JGrapsa
Digoxin is back — and the data backs it up 💊🫀
Just published in JAMA, this meta-analysis pooling three major trials (DIG 1997, DIGIT-HF 2025, DECISION 2026) delivers a clear verdict on digitalis glycosides in heart failure. The primary composite outcome — cardiovascular death or worsening HF — was reduced by 15% (HR 0.85, 95% CI 0.80–0.90), with zero heterogeneity across trials (I²=0%). Worsening HF events alone were cut by 25% (HR 0.75, 95% CI 0.69–0.81). A drug discovered over 200 years ago, long sidelined over safety concerns, is now showing consistent, reproducible benefit across modern trial populations. The question is no longer whether it works — but for whom, and when.
#HeartFailure #Digoxin #DigitalisGlycosides #JAMA #Cardiology #HFrEF #MetaAnalysis #CardioTwitter #MedTwitter #EvidenceBasedMedicine
Good news for CKD patients who love their morning coffee ☕🫘
A new review in Nephrology Dialysis Transplantation (Vieira et al., 2026) challenges the routine restriction of coffee in chronic kidney disease — and the evidence is surprisingly reassuring. Moderate intake under 400mg/day is associated with 11–30% lower risk of incident CKD and slower progression, improved GFR, lower ESKD risk, cardioprotection, and even neuroprotection in stages 2–3. Not all coffee is equal though — filtered coffee preserves bioactives without raising cholesterol, while unfiltered and espresso-based drinks increase LDL via diterpenes. Risks remain for CYP1A2 slow metabolizers, those with sleep disorders, and advanced CKD stages 4–5. The bottom line: routine coffee restriction in CKD is likely unnecessary. Individualize, don’t generalize.
#CKD #ChronicKidneyDisease #Nephrology #Coffee #Caffeine #KidneyHealth #CardioRenal #NephrologyTwitter #MedTwitter #EvidenceBasedMedicine
A promising target, a disappointing result — and an important lesson 🧬💊
Published in JACC (White WB et al., 2026), this randomized Phase 2 trial tested XXB750 — a first-in-class NPR-1 agonist — in 189 patients with resistant hypertension already on 3+ antihypertensive medications. The biology made sense: activating natriuretic peptide receptor 1 should drive vasodilation and natriuresis via cyclic GMP. And indeed, XXB750 did engage its target dose-dependently — cyclic GMP rose significantly at 120mg and 240mg. But the primary endpoint told a different story: no meaningful reduction in 24-hour systolic BP at any dose. Target engagement without clinical effect. It’s a stark reminder that mechanistic plausibility doesn’t guarantee therapeutic success — and that resistant hypertension remains one of cardiology’s hardest problems to crack.
#ResistantHypertension #Hypertension #NPR1 #XXB750 #ClinicalTrials #JACC #Cardiology #DrugDevelopment #CardioTwitter #MedTwitter #Phase2
Iron deficiency definitions and their clinical and prognostic associations across the spectrum of left ventricular ejection fraction in heart failure
Iron deficiency is common and clinically relevant across the HF spectrum, irrespective of definition, and is associated with impaired quality of life and adverse outcomes in patients with LVEF <50%
@ESC_Journals@SJGreene_md@gcfmd@mvaduganathan@safchat@HSkouri@Hragy@GianluSava
https://t.co/gfbJ9kbiXF
💊 Practical algorithm for diuretic resistance in acute HF from #HeartFailure26— this is the slide to save!
Start: Furosemide 120-160 mg
↓ Still congested?
Add Chlortalidone 12.5-50 mg/24h
↓ Still congested?
Tailor to the problem:
• Metabolic alkalosis → Acetazolamide 120-500 mg/24h
• Hyponatremia → Tolvaptan 15-50 mg/24h
• rLVEF + hypopotassemia → MRA 25-100 mg/24h
And running through the whole algorithm:
➕ Add iSGLT2 throughout
➕ Add sacubitril/valsartan if LVEF <49%
➕ Consider parenteral route if oral absorption is the issue
Clean. Practical. Evidence-based. 💯
(Adapted from de la Espriella R et al. Nefrologia 2021)
#CardioTwitter #HeartFailure #Cardiology #Diuretics #HFrEF
🧵 Why do loop diuretics stop working in acute heart failure? Dr. Ana Belen Mendez Fernandez breaks it down at #HeartFailure26
Diuretic resistance = mismatch between drug delivery & tubular response. 3 main culprits:
1️⃣ Impaired drug delivery
• Gut edema → poor oral absorption
• Reduced renal perfusion
• Hypoalbuminemia
2️⃣ Tubular adaptation (“braking phenomenon”)
• Distal nephron hypertrophy
• ↑ Na reabsorption distal to loop of Henle
3️⃣ Neurohormonal activation
• RAAS activation
• Sympathetic nervous system activation
Know the mechanism → pick the right counterstrategy 💡
#CardioTwitter #HeartFailure #Cardiology #Diuretics
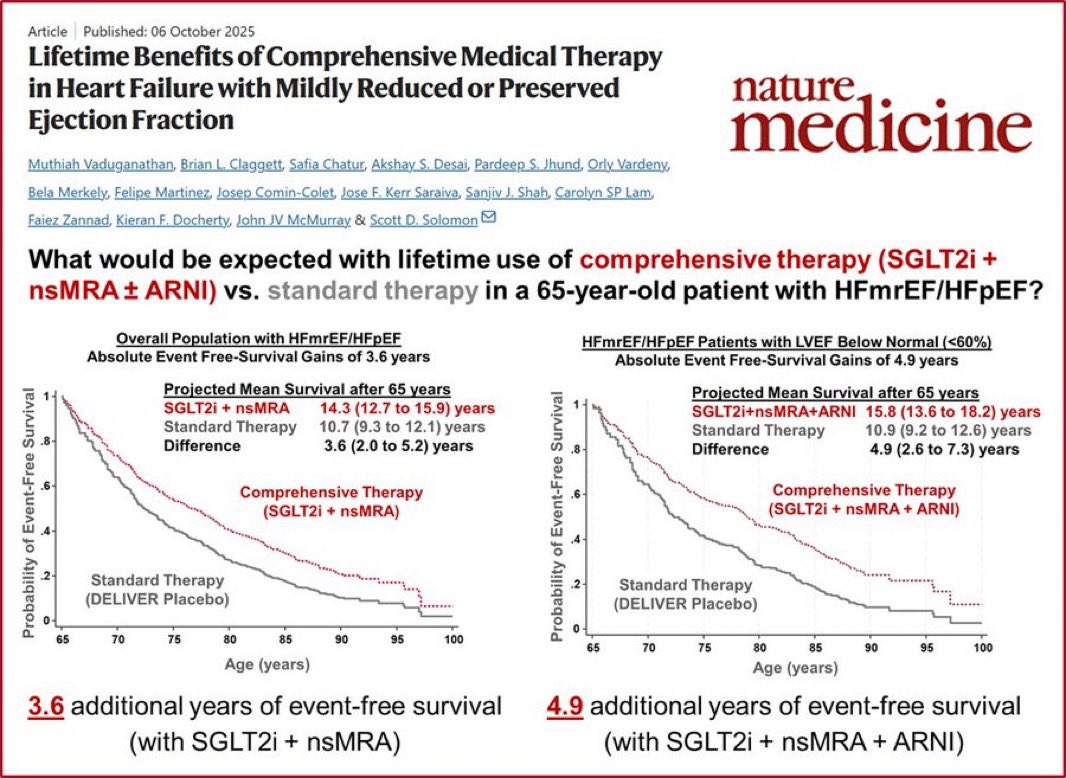
💊🫀 What does optimal therapy actually buy a 65-year-old with HFmrEF/HFpEF?
From Nature Medicine (Vaduganathan et al., 2025):
🔴 SGLT2i + nsMRA → +3.6 years event-free survival
🔴 SGLT2i + nsMRA + ARNI → +4.9 years (LVEF <60%)
vs. standard therapy alone.
Nearly 5 extra years without hospitalization or death.
💡 These drugs exist. They work. Are all eligible patients receiving them?
Vaduganathan et al. Nature Medicine, Oct 2025
@mvaduganathan
#HeartFailure #HFpEF #HFmrEF #SGLT2i #ARNI #Cardiology #MedTwitter #NatureMedicine
📄 LGE phenotype vs burden in cardiac sarcoidosis: does pattern matter more than quantity?
🔗 DOI: https://t.co/3KZvuxjuft
🫀 In cardiac sarcoidosis, risk stratification for ventricular arrhythmias remains challenging.
This prospective study compares LGE burden vs LGE phenotype on CMR for predicting arrhythmic events.
✨ Key findings:
🔹 The “pathology-frequent” LGE phenotype strongly predicts ventricular arrhythmias
➡️ All arrhythmic events occurred only in this phenotype
🔹 Both approaches perform well:
LGE burden (quantitative %)
LGE phenotype (pattern-based)
👉 BUT:
🔹 LGE phenotype achieved 100% negative predictive value
➡️ No events in patients without this phenotype
⚡ Practical advantages of LGE phenotyping:
✅ Much higher reproducibility (κ = 0.97 vs 0.41)
✅ ~5x faster than LGE quantification
✅ Easier to apply in clinical routine
📊 Additional insights:
👉 Arrhythmic risk is mainly linked to scar-related re-entry, not inflammation
👉 FDG-PET did not add independent prognostic value
💡 Clinical take-home message:
👉 Pattern recognition may be as important as quantification
👉 LGE phenotype could:
improve risk stratification
guide ICD decision-making
simplify clinical workflows
🚨 Bottom line:
In cardiac sarcoidosis, how scar looks may matter more than how much scar there is.
#Cardiology #CardiacSarcoidosis #CMR #LGE #Arrhythmia #SuddenCardiacDeath #Imaging #RiskStratification #Electrophysiology 🫀⚡📊
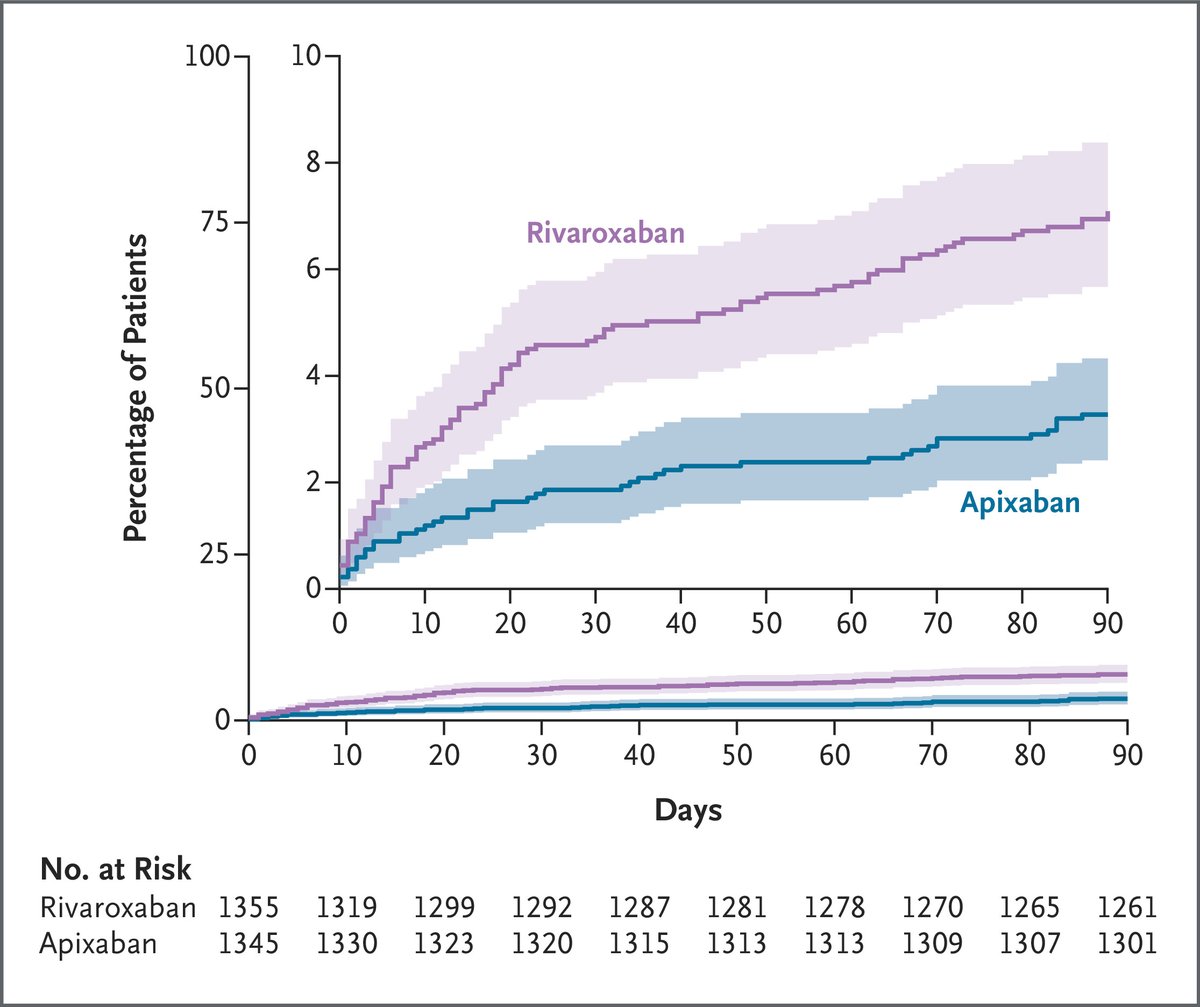
Finally published: the COBRRA trial, the first randomized head-to-head comparison of major DOACs — something the companies would never have done themselves, as a direct confrontation goes beyond their commercial interests. This was driven by independent investigators. The results somewhat support the idea of apixaban being the “safer” DOAC. That said, the list of study limitations is long, and for me, labeling something as “safe” is not enough — after all, even placebo is “safe” when it comes to bleeding. https://t.co/eYehndGzvB
AI no different from MD in diagnosis or appropriateness of treatment but worse in practicality (p = 0.003) and cost effectiveness (p = 0.004). https://t.co/oUoetuLxfp
Diastolic Dysfunction in Acute and Critical Illness: Acute Pathophysiology to Chronic Heart Failure
Acute HFpEF is a systemic inflammatory syndrome driven by comorbidities, extending beyond the myocardium.
In critical illness, acute diastolic dysfunction is common, but its link to mortality is complex.
New therapies (SGLT2i, GLP-1 RAs) and AI-driven diagnostics are revolutionizing HFpEF care.
#Cardiology #MedTwitter #CardioTwitter #HeartHealth #Healthcare
@JACCJournals@ACCinTouch@mvaduganathan@hvanspall@DrMarthaGulati@SJGreene_md@gcfmd@biljana_parapid@hfcollaboratory@Hragy
https://t.co/R2xtRLubYY
⏳ Aortic stenosis with #HFrEF: beyond the valve.
GDMT optimisation + TAVI strategy must go hand in hand. On 21 March (8:30-9:30), #iHFCourse 2026 explores integrated care in complex AS patients.
📅 20-21 March 2026 | Online | 100% free
👉 Programme: https://t.co/jq1enXNyCg
#AorticStenosis #TAVI #HeartFailure #Cardiology