🚨 RESET-C trial: single-cycle neoadjuvant pembrolizumab in stage I–III dMMR colon cancer (n=85)
https://t.co/j2KFLLOdVg
🎯 pCR 44% || MPR 57%
💥 DFS and OS rates: 96% and 98% at 18.4 months
▪️ Grade ≥3 AEs in 11%; only 1 recurrence reported
One shot and the tumor may already be hitting the RESET button 🔄
@OncoAlert@OncoReporte@myESMO@_SEOM@GrupoTTD
@ChandrakanthMv So in practice , what would be the best test after biopsy ? Send straight for a molecular panel? CGP or targeted panel? any recommendations on indian labs ?
@ChandrakanthMv Longest OS, but the control arm also performed spectacularly well (20 months) compared to 13 months in Imbrave 150. I think the two are comparable
Premenopausal HR+/HER2+ eBC – Adjuvant ET
• RD after NAT → OFS + AI
• pCR after NAT → risk-adapted
– Stage III → OFS + AI
– Stage I–II → AI or TAM ± OFS
• Upfront surgery → baseline stage-driven ET
Principle:
RD = ER-dependent, chemo-resistant → needs ET intensification
Great editorial👇
https://t.co/AuDXPhHDoi
@ChandrakanthMv CD 34 is a marker of immaturity (present on stem cells). As promyelocytes are more mature, they lack CD34 expression. That's how I remember.
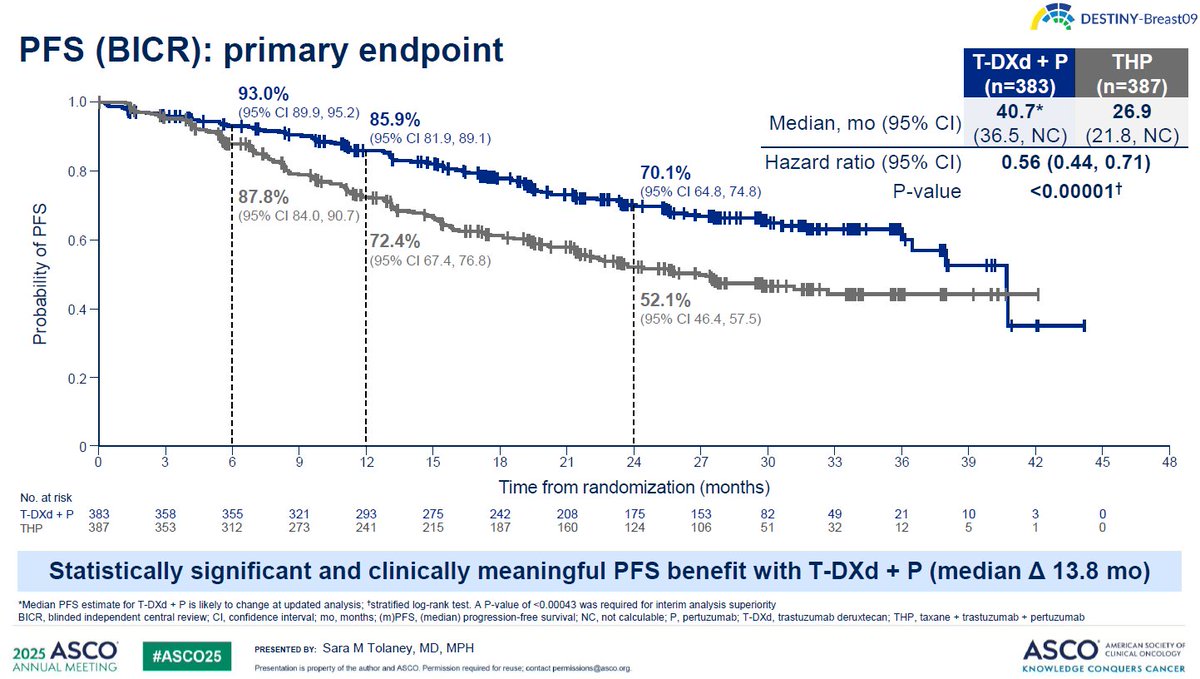
Why Induction Should Be Performed With T-DXd + Pertuzumab (IMO)
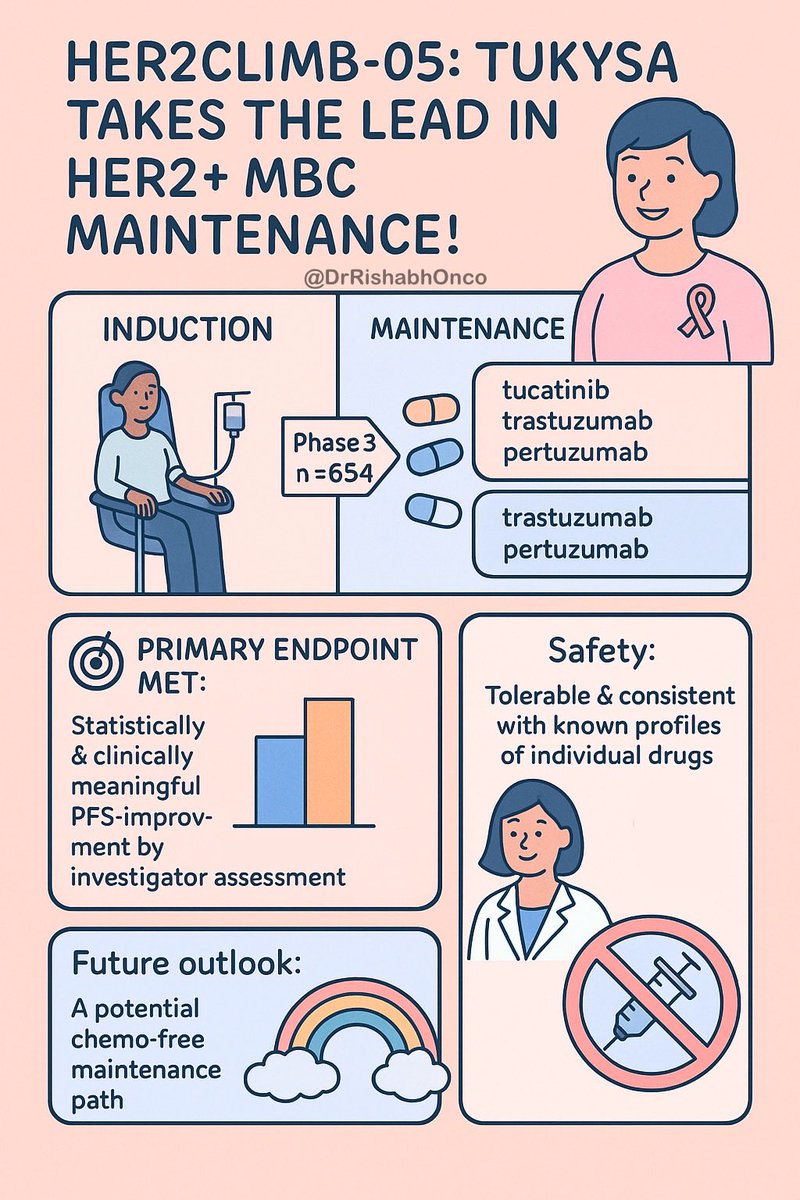
The key distinction of DESTINY-Breast09 compared with HER2CLIMB-05 and PATINA is randomization at true treatment initiation. In both HER2CLIMB-05 and PATINA, only patients who did not progress during THP induction were randomized; early progressors were excluded by design.
DESTINY-Breast09 therefore captures the full early-risk population. At 6 months—approximately the end of induction—12.2% of patients in the THP control arm had already experienced a PFS event, compared with 7.0% in the T-DXd + pertuzumab arm, corresponding to an absolute 5.2% reduction in early progression within the first 6 months. Importantly, this separation is not transient. By 12 months, the absolute PFS difference widens to 13.5%, indicating that T-DXd + pertuzumab not only prevents early progression but continues to deepen benefit over time.
By contrast, PATINA and HER2CLIMB-05 never randomized the initial ~12% of patients who progressed during THP induction. Had induction been performed with T-DXd + pertuzumab instead of THP, a substantial proportion of these early progressions—approximately 5% in absolute terms—might have been prevented. These patients would not have been lost upfront and could have proceeded to effective maintenance strategies rather than being excluded at the outset.
At present, because maintenance trials have uniformly used THP as induction, there are no prospective data evaluating palbociclib- or tucatinib-based maintenance following T-DXd + pertuzumab induction. Nevertheless, indirect inferences from DESTINY-Breast09 suggest a pragmatic clinical strategy: in patients who develop tolerability issues, treatment may reasonably be initiated with T-DXd + pertuzumab, followed by maintenance tailored to hormone receptor subtype once maximal disease control is achieved. This approach leverages early disease suppression while preserving the opportunity for durable, subtype-specific maintenance therapy.
Critically, in HR–positive disease, ET must remain an integral component of maintenance and should not be omitted.
@Niva_Bupa@Niva_Bupa@NivaBupaSupport your people need to learn sales skills, not antagonize your customers with hate and threats. I was planning on renewal and have learnt my lesson. No way as a doctor will I ever recommend Niva Bupa to anyone. Hope the upper management knows this
@NivaBupaSupport@Niva_Bupa@irdaindia Had a terrible experience with the agents from Niva Bupa. I was explaining that I was planning to change the policy rather than renew it, and they were issuing threats of terminating the policy.
Such crass, deplorable behavior.
This person called Tanya was just shouting over the phone saying, all other agents are cheats and then just abused me and threatened termination of the policy. All this, beciased I dared to consider another policy. @Niva_Bupa